Cerebral toxoplasmosis with reference to standard pathology book or robbin
Reading File
Finding Sources
Finding Sources
Searching PubMed
cerebral toxoplasmosis pathology immunocompromised
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete answer:
Cerebral Toxoplasmosis
Sources: Adams & Victor's Principles of Neurology 12th Ed, Medical Microbiology 9e (Murray), Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine
The Organism
Toxoplasma gondii is a tiny (2-5 μm), obligate intracellular parasite belonging to the Apicomplexa clade, related to Plasmodium and Cystoisospora. It is readily recognized on Wright- or Giemsa-stained preparations.
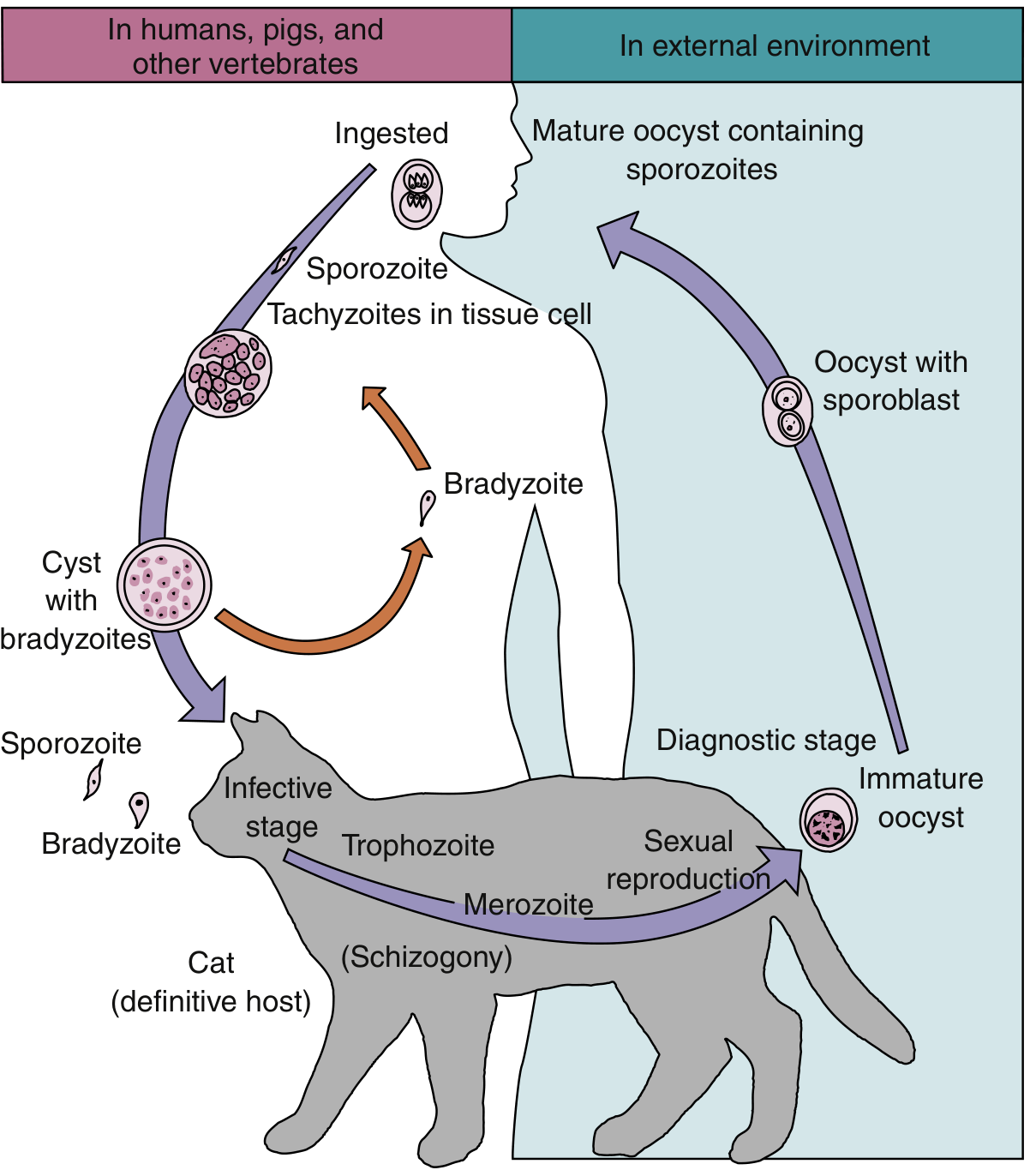
The organism exists in three forms:
- Tachyzoites - slender, crescentic, rapidly multiplying forms responsible for initial infection and tissue damage
- Bradyzoites - slow-growing, shorter forms that form cysts in chronic infection
- Oocysts - passed in cat feces, maturing into infective forms within 3-4 days
The cat (and other felines) is the definitive host - sexual reproduction occurs in feline intestinal cells, with oocysts shed in feces. Humans and other vertebrates are intermediate hosts.
Epidemiology
- Seroprevalence is wide: approximately 40% of American city-dwellers have specific anti-toxoplasma antibodies
- Routes of infection in humans:
- Ingestion of undercooked/raw meat containing tissue cysts
- Ingestion of oocysts from cat-feces-contaminated soil, water, or food
- Transplacental (congenital) transmission
- Organ transplantation or blood transfusion
- Accidental inoculation of tachyzoites
- Prior to the AIDS epidemic (1975), only 45 well-documented adult cases existed in medical literature; half had underlying immunosuppressive conditions
- Today, toxoplasmosis is the most common cause of focal cerebral lesions in HIV patients
- In regions with antiretroviral therapy (ART) access, cerebral toxoplasmosis has become much less common
Pathogenesis
The manifestations of toxoplasmosis are entirely dependent on host immune status. Cell-mediated immunity is the key defense. In immunocompetent individuals, infection is controlled and becomes latent - bradyzoite-filled cysts reside silently in brain and muscle tissue.
Reactivation - not primary infection - is the mechanism of cerebral toxoplasmosis in AIDS patients. When CD4+ T-cell counts fall below 100/μL, latent bradyzoites reactivate to rapidly dividing tachyzoites, resulting in progressive tissue destruction.
Gross and Microscopic Pathology
This is the core pathological picture (Adams & Victor's Neurology):
Gross findings:
- One or more foci of inflammatory necrosis - essentially abscesses
- Free and encysted T. gondii organisms scattered throughout both white and gray matter
- Rare cases show large areas of necrosis manifesting as mass lesions
- Predilection for the basal ganglia, thalamus, and gray-white junction
Microscopic findings:
- Central coagulative necrosis with surrounding inflammatory infiltrate
- Bradyzoites forming tissue cysts (round structures packed with organisms, up to 200 μm)
- Free tachyzoites in surrounding tissue - crescentic, 2-5 μm, visible on H&E and Giemsa
- Vascular changes may be present
Staining: Wright's or Giemsa stains identify organisms; T. gondii-specific immunoperoxidase staining can be performed on any tissue for definitive identification. PCR on tissue can amplify both tachyzoite and bradyzoite DNA.
Clinical Features
Congenital Toxoplasmosis
Results from maternal parasitemia during primary infection in pregnancy. Features include:
- Classic triad: Hydrocephalus, chorioretinitis, intracranial calcifications
- Fever, rash, seizures, hepatosplenomegaly at birth (active infection)
- Psychomotor retardation
- Subclinical infection presenting months to years later with chorioretinitis
- Many infants succumb; survivors have variable degrees of deficit
Acquired Toxoplasmosis in Immunocompetent Adults
- Usually subclinical
- May present as painless lymphadenopathy or mononucleosis-like syndrome
- Rare fulminant form: encephalitis, myocarditis, polymyositis, rickettsial-like rash
Cerebral Toxoplasmosis in HIV/AIDS (CD4 <100/μL)
Typical presentations:
- Single seizure (often the first manifestation)
- Focal neurological deficit (hemiparesis, aphasia, ataxia - depends on lesion location)
- Headache or features of raised intracranial pressure
- May be discovered incidentally on imaging in some patients
Imaging
MRI with contrast is the investigation of choice. Classic finding is ring-enhancing lesions with surrounding vasogenic edema and mass effect, often multiple, with a predilection for basal ganglia and thalamus.
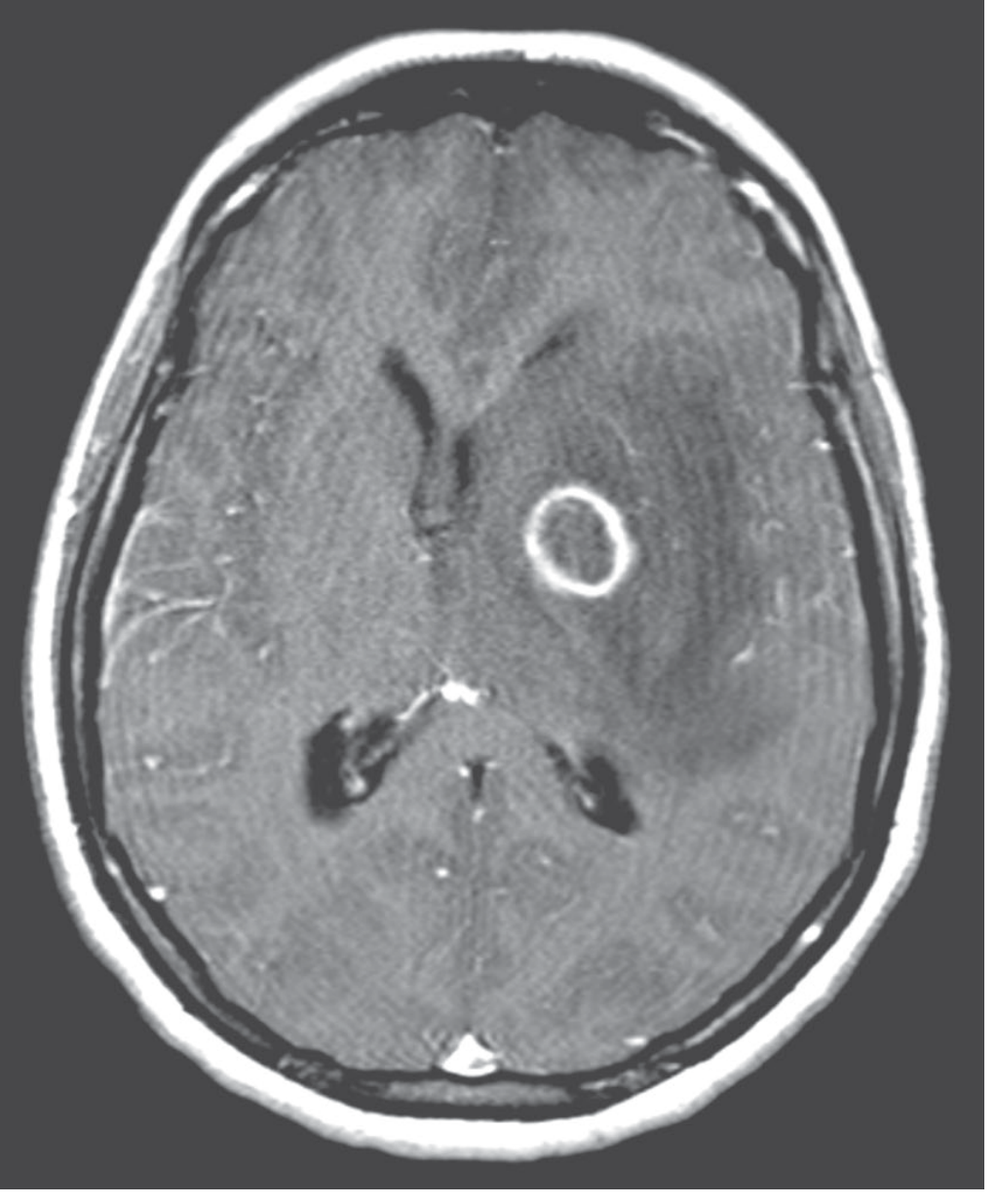
Key differential: CNS lymphoma (also ring-enhancing in HIV, but typically involves deep white matter; FDG-PET and MR spectroscopy help differentiation).
Diagnosis
| Method | Details |
|---|---|
| Imaging | MRI - ring-enhancing lesion(s), basal ganglia/thalamus predilection |
| Serology | IgG/IgM antibody titres; unreliable in HIV (may not show rise) |
| Empiric treatment response | Standard approach in HIV with compatible imaging - improvement in 1-2 weeks confirms diagnosis |
| CSF | Lymphocytic pleocytosis, elevated protein; PCR for T. gondii DNA |
| Brain biopsy | Reserved for non-responders; immunoperoxidase staining identifies organisms |
A presumptive diagnosis can be made clinically in an HIV patient with CD4 <100/μL and compatible imaging, and empiric treatment started. If there is no improvement after 2 weeks, brain biopsy to exclude CNS lymphoma is required.
If a patient has a prior IgG-negative result (never been infected), the likelihood of a mass lesion being toxoplasmosis drops to ~10%, and earlier biopsy is justified (Harrison's 22e).
Treatment
First-line (adults):
- Pyrimethamine 200 mg loading dose, then 50-75 mg/day PO
- Sulfadiazine 4-6 g/day PO (in divided doses)
- Leucovorin 15-20 mg/day PO (to counteract pyrimethamine's anti-folate effect and prevent bone marrow suppression)
- Duration: minimum 6 weeks (acute phase)
Alternative (if sulfa-intolerant):
- Pyrimethamine + Clindamycin (best-studied alternative)
- TMP-SMX (trimethoprim-sulfamethoxazole) is an effective oral alternative
Maintenance (secondary prophylaxis) in HIV:
- Continued at reduced doses until CD4 count exceeds 200-250/μL for at least 6 months on ART
- Without maintenance, relapse rate is ~25% after stopping therapy at 6 weeks
Corticosteroids: Used adjunctively for cerebral edema or ocular toxoplasmosis threatening the macula
Immune Reconstitution Inflammatory Syndrome (IRIS): Starting ART in a patient with active toxoplasmosis can precipitate a fulminant inflammatory response around the parasite abscess - requires careful monitoring
Primary Prophylaxis
Indicated for HIV-positive patients who are IgG-seropositive with CD4 <100/μL:
- TMP-SMX 1 DS tablet daily (also covers Pneumocystis)
- Alternatives: Dapsone + pyrimethamine + leucovorin; atovaquone ± pyrimethamine
Summary Table
| Feature | Details |
|---|---|
| Organism | Toxoplasma gondii - obligate intracellular, Apicomplexa |
| Definitive host | Cat (sexual cycle, oocyst shedding) |
| At-risk group | HIV/AIDS (CD4 <100/μL), transplant recipients, congenital |
| Mechanism | Reactivation of latent bradyzoite cysts |
| Gross pathology | Focal necrotic abscesses, white + gray matter, basal ganglia |
| Microscopy | Necrosis, tissue cysts (bradyzoites), free tachyzoites |
| Imaging | Ring-enhancing lesions on MRI, mass effect |
| Treatment | Pyrimethamine + sulfadiazine + leucovorin |
| Prophylaxis | TMP-SMX (CD4 <100/μL, IgG+) |
References:
- Adams & Victor's Principles of Neurology, 12th Ed - Chapter 31 (pp. 742-744)
- Medical Microbiology 9e (Murray) - Chapter 73
- Harrison's Principles of Internal Medicine 22E (2025)
- Goldman-Cecil Medicine (OI prophylaxis guidelines)
This is a shared conversation. Sign in to Orris to start your own chat.