Immunopathology and AIDS 1.Hypersensitivity Reactions-define, Classify,and discuss 2.Type 1 Hypersensitivity Reaction Discuss and examples** 3.Graft rejection-mechanism and role of HLA antigens 4.Autoimmunity-define,pathogenesis. Autoimmune disorders-mechanisms* 5.SLE- pathogenesis,morphology And diagnosis* 6.HIV- life cycle,etiopathogenesis,lab Diagnosis,clinical stages of AIDS, Neoplasms found in AIDS patients** 2 mbbs pathology refer robbin add easy to draw diagram coloured , answer all question important topics frequently ask topic in muhs exam systemically aswer all
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Here is your complete, exam-ready 2nd MBBS Pathology notes on Immunopathology and AIDS, based on Robbins & Kumar (Basic Pathology + Pathologic Basis of Disease), organized systematically for MUHS exams.
IMMUNOPATHOLOGY AND AIDS
2nd MBBS Pathology - MUHS Exam Notes
(Reference: Robbins & Kumar - Basic Pathology / Pathologic Basis of Disease)
QUESTION 1: HYPERSENSITIVITY REACTIONS
Definition
Hypersensitivity refers to injurious immune reactions that cause tissue damage. These reactions arise when the immune response is:
- Inadequately controlled
- Directed against normally harmless antigens (environmental allergens)
- Inappropriately targeted to host tissues (autoimmunity)
The term implies an excessive or harmful reaction to an antigen in a previously sensitized individual.
Causes of Hypersensitivity
| Cause | Example |
|---|---|
| Autoimmunity (self antigens) | SLE, rheumatoid arthritis |
| Reactions against microbes | Post-streptococcal GN, TB |
| Environmental antigens | Pollen, dust mites, drugs |
Classification (Gell and Coombs - 4 Types)
┌─────────────────────────────────────────────────────────────────────┐
│ CLASSIFICATION OF HYPERSENSITIVITY REACTIONS │
├────────┬───────────────┬───────────────┬────────────────────────────┤
│ TYPE │ MECHANISM │ MEDIATORS │ EXAMPLES │
├────────┼───────────────┼───────────────┼────────────────────────────┤
│ I │ IgE-mediated │ IgE, Mast │ Anaphylaxis, Asthma, │
│ (Imm.) │ (Immediate) │ cells, │ Allergic rhinitis, │
│ │ │ Eosinophils │ Urticaria, Food allergy │
├────────┼───────────────┼───────────────┼────────────────────────────┤
│ II │ Antibody vs. │ IgG, IgM, │ Autoimmune hemolytic │
│ (Cyto.)│ cell/tissue │ Complement, │ anemia, Goodpasture, │
│ │ antigens │ Phagocytes │ Graves disease, MG │
├────────┼───────────────┼───────────────┼────────────────────────────┤
│ III │ Immune complex │ IgG, Comple- │ SLE, Post-strep GN, │
│(IC-med)│ deposition │ ment, Neutro- │ Serum sickness, │
│ │ │ phils │ Arthus reaction │
├────────┼───────────────┼───────────────┼────────────────────────────┤
│ IV │ T cell- │ CD4+ (DTH), │ Contact dermatitis, TB │
│ (DTH) │ mediated │ CD8+ (CTL), │ granuloma, Type 1 DM, │
│ │ │ Macrophages │ Multiple sclerosis │
└────────┴───────────────┴───────────────┴────────────────────────────┘
- Types I, II, III = Antibody-mediated
- Type IV = Cell-mediated (Delayed-type Hypersensitivity)
QUESTION 2: TYPE I HYPERSENSITIVITY (IMMEDIATE / IgE-MEDIATED) ⭐⭐
Definition
Type I hypersensitivity is an immediate (within minutes) immunologic reaction triggered by IgE antibodies bound to mast cells, upon re-exposure to an allergen. Also called Allergy or Atopy.
Mechanism (Step by Step)
┌─────────────────────────────────────────────────────────────────────┐
│ TYPE I HYPERSENSITIVITY - MECHANISM │
└─────────────────────────────────────────────────────────────────────┘
SENSITIZATION PHASE (First exposure):
Allergen → APC presentation → Th2 cell activation
↓
Th2 cells secrete IL-4 and IL-13
↓
B cell class switching → IgE production
↓
IgE binds to FcεRI receptors on MAST CELLS and BASOPHILS
(Mast cells become "armed/sensitized")
ELICITATION PHASE (Re-exposure):
Same allergen re-enters → CROSS-LINKS IgE on mast cells
↓
Mast cell DEGRANULATION (within seconds-minutes)
↓
Release of PRIMARY MEDIATORS from granules:
• Histamine (vasodilation, increased permeability, smooth muscle spasm)
• ECF-A (eosinophil chemotaxis)
• NCF-A (neutrophil chemotaxis)
• Proteases (tryptase, chymase)
↓
Release of SECONDARY MEDIATORS (newly synthesized):
• Leukotrienes (LTC4, LTD4, LTE4) - sustained bronchospasm
• Prostaglandin D2 - bronchoconstriction
• PAF - aggregates platelets
• Cytokines (IL-4, IL-5, TNF) - late phase
Two Phases of Type I Response
Immediate Phase (0-30 minutes):
- Vasodilation, increased vascular permeability
- Smooth muscle spasm
- Hypersecretion of mucus
- Due to: Histamine, prostaglandins
Late Phase (2-24 hours):
- Infiltration by eosinophils, basophils, neutrophils, T cells
- Tissue damage, mucosal edema
- Due to: Leukotrienes, cytokines, eosinophil products (MBP)
Mediators Summary Table
| Mediator | Source | Effect |
|---|---|---|
| Histamine | Granules | Vasodilation, bronchoconstriction, itch |
| LTC4, LTD4 | Newly formed | Sustained bronchospasm (SRS-A) |
| PGD2 | Membrane | Bronchoconstriction |
| IL-5 | Cytokines | Eosinophil activation |
| TNF-α | Cytokines | Inflammation |
| Tryptase | Granules | Marker of mast cell activation |
Clinical Examples
| Condition | Features |
|---|---|
| Anaphylaxis | Systemic - shock, laryngospasm, urticaria, can be fatal |
| Bronchial Asthma | Episodic wheeze, breathlessness, bronchospasm |
| Allergic Rhinitis (Hay Fever) | Sneezing, nasal congestion, watery discharge |
| Urticaria/Angioedema | Skin wheals, dermal edema |
| Food Allergy | Peanuts, shellfish - GI and systemic |
| Drug Allergy | Penicillin - urticaria to anaphylaxis |
| Atopic Dermatitis (Eczema) | Chronic pruritic skin inflammation |
MUHS Exam Tip: Anaphylaxis = most severe systemic Type I reaction. SRS-A (Slow-Reacting Substance of Anaphylaxis) = LTC4 + LTD4 + LTE4.
QUESTION 3: GRAFT REJECTION - MECHANISM AND ROLE OF HLA ANTIGENS ⭐
Types of Graft Rejection
┌────────────────────────────────────────────────────────────┐
│ GRAFT REJECTION │
├──────────────┬───────────┬─────────────┬───────────────────┤
│ TYPE │ TIMING │ MECHANISM │ MORPHOLOGY │
├──────────────┼───────────┼─────────────┼───────────────────┤
│ Hyperacute │ Minutes- │ Preformed │ Thrombosis, │
│ │ hours │ antibodies │ ischemic necrosis │
│ │ │ against HLA │ │
├──────────────┼───────────┼─────────────┼───────────────────┤
│ Acute │ Days- │ T cells │ Tubulointerstitial │
│ Cellular │ weeks │ (CD4+, CD8+)│ nephritis, │
│ │ │ react to │ vasculitis │
│ │ │ donor HLA │ │
├──────────────┼───────────┼─────────────┼───────────────────┤
│ Acute │ Weeks- │ Antibodies │ Necrotizing │
│ Humoral │ months │ to HLA │ vasculitis │
│ │ │ (de novo) │ │
├──────────────┼───────────┼─────────────┼───────────────────┤
│ Chronic │ Months- │ T cells + │ Vascular │
│ │ years │ Antibodies │ intimal thicken- │
│ │ │ │ ing, fibrosis, │
│ │ │ │ "graft vasculo- │
│ │ │ │ pathy" │
└──────────────┴───────────┴─────────────┴───────────────────┘
Mechanisms of Acute T-Cell Mediated Rejection
Two pathways by which T cells recognize alloantigens:
-
Direct pathway:
- Recipient T cells recognize intact donor MHC on donor APCs
- Responsible for early, acute rejection
-
Indirect pathway:
- Recipient APCs process donor antigens
- Present donor peptides (including HLA peptides) to recipient T cells
- More important in chronic rejection
Effector mechanisms:
- CD4+ Th1 cells → secrete IFN-γ → macrophage activation → DTH-type inflammation
- CD8+ CTLs → directly kill graft parenchymal cells (via perforins/granzymes)
- CD4+ Th17 cells → recruit neutrophils
Role of HLA (MHC) Antigens in Graft Rejection
HLA = Human Leukocyte Antigens (encoded by MHC genes on chromosome 6p)
┌──────────────────────────────────────────────────────┐
│ HLA ANTIGENS IN TRANSPLANTATION │
├──────────────┬───────────────────────────────────────┤
│ CLASS I │ HLA-A, HLA-B, HLA-C │
│ (HLA Class I)│ Present on ALL nucleated cells │
│ │ Recognized by CD8+ T cells │
├──────────────┼───────────────────────────────────────┤
│ CLASS II │ HLA-DR, HLA-DQ, HLA-DP │
│ (HLA Class II│ Present on APCs (DC, macrophage, B) │
│ │ Recognized by CD4+ T cells │
└──────────────┴───────────────────────────────────────┘
Why HLA antigens cause rejection:
- Each person has a unique set of HLA molecules (except identical twins)
- Donor HLA molecules on graft cells = foreign antigens to recipient
- Recipient immune system mounts both cellular and humoral attack
- Greater the HLA mismatch → greater the rejection risk
Clinical significance:
- HLA typing done before transplantation (crossmatching)
- Best match = HLA-identical sibling (lowest rejection)
- Immunosuppressants (cyclosporine, tacrolimus) block T cell activation
Hyperacute rejection:
- Caused by preformed anti-HLA antibodies (from prior transfusion, pregnancy, or transplant)
- Complement activation → thrombosis → immediate graft loss
QUESTION 4: AUTOIMMUNITY ⭐
Definition
Autoimmunity is the failure of self-tolerance resulting in immune reactions directed against one's own (self) tissues, leading to tissue injury and autoimmune diseases.
Self-tolerance: The normal state in which the immune system does not react against its own antigens.
Mechanisms of Self-Tolerance (Normal)
-
Central tolerance:
- In thymus (T cells) and bone marrow (B cells)
- Clonal deletion of self-reactive lymphocytes (negative selection)
- AIRE gene controls expression of tissue antigens in thymus
-
Peripheral tolerance:
- Clonal anergy: Self-reactive T cells encounter antigen without co-stimulation → become unresponsive
- Regulatory T cells (Tregs): CD4+CD25+FoxP3+ cells suppress self-reactive T cells
- Activation-induced cell death (AICD): Repeated antigenic stimulation → apoptosis via Fas-FasL
Pathogenesis of Autoimmunity
┌──────────────────────────────────────────────────────────────────┐
│ PATHOGENESIS OF AUTOIMMUNITY │
└──────────────────────────────────────────────────────────────────┘
GENETIC FACTORS ENVIRONMENTAL FACTORS
• HLA genes (HLA-DR2, • Infections (molecular mimicry)
HLA-DR3, HLA-B27) • Polyclonal B cell activation
• Non-HLA genes • Tissue injury releasing
• PTPN22, CTLA4, FoxP3 sequestered antigens
• AIRE mutations • UV light (SLE)
↓ ↓
FAILURE OF SELF-TOLERANCE
• Escape of autoreactive T cells from thymus
• Loss of peripheral anergy
• Deficient Treg function
• Molecular mimicry
• Bystander activation
↓
AUTOIMMUNE DISEASE
(organ-specific or systemic)
Mechanisms in Autoimmune Disorders
| Mechanism | Disease | How It Works |
|---|---|---|
| Antibodies vs cell antigens (Type II) | Autoimmune hemolytic anemia | Anti-RBC IgG → complement lysis |
| Antibodies vs receptor (Type II) | Graves disease | Anti-TSH receptor → stimulation |
| Antibodies blocking receptor (Type II) | Myasthenia Gravis | Anti-AChR → impaired NMJ |
| Immune complexes (Type III) | SLE | Anti-dsDNA complexes → glomerulonephritis |
| T-cell mediated (Type IV) | Type 1 Diabetes | CD8+ T cells destroy beta cells |
| T cell + antibody | Rheumatoid Arthritis | Anti-IgG (RF), T cells in synovium |
Key concept: Molecular mimicry - Streptococcal M protein mimics cardiac myosin → rheumatic fever. EBV, CMV, and HIV cause polyclonal B cell activation → autoantibodies.
QUESTION 5: SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) ⭐⭐
Definition
SLE is a chronic, multisystem autoimmune disease characterized by widespread autoantibodies against nuclear and cytoplasmic antigens, leading to tissue injury via immune complex deposition.
Pathogenesis of SLE
┌─────────────────────────────────────────────────────────────────┐
│ PATHOGENESIS OF SLE │
└─────────────────────────────────────────────────────────────────┘
GENETIC PREDISPOSITION:
HLA-DR2, HLA-DR3 → Susceptibility
C1q, C2, C4 deficiencies → Impaired clearance of apoptotic material
TRIGGER:
UV light, Estrogen (F:M = 9:1), Drugs (hydralazine, procainamide)
DEFECTIVE CLEARANCE OF APOPTOTIC CELLS:
↓ Apoptotic bodies release nuclear fragments (dsDNA, histones, RNA)
↓ Normally cleared; in SLE → persist and stimulate TLRs
↓ TLR activation in pDCs → excessive type I IFN production
LOSS OF SELF-TOLERANCE:
↓ Autoreactive B cells and T cells escape elimination
↓ CD4+ T cell help → B cell hyperactivation
↓ Production of ANA (Antinuclear Antibodies)
KEY AUTOANTIBODIES IN SLE:
• Anti-dsDNA (highly specific for SLE, correlates with disease activity)
• Anti-Sm (Smith antigen - highly specific)
• Anti-histone (drug-induced lupus)
• Anti-Ro/SSA, Anti-La/SSB (neonatal lupus, Sjogren's)
• Antiphospholipid antibodies (thrombosis, recurrent miscarriage)
• ANA (screening test - sensitive but not specific)
TISSUE INJURY:
• Immune complexes (IC) deposit in basement membranes
→ Complement activation → Inflammation → Organ damage
• Direct antibody attack on cells (anemia, thrombocytopenia)
• T cell-mediated tissue injury
Morphology of SLE
1. Skin:
- Butterfly (malar) rash - erythema over cheeks and nose
- Hematoxylin bodies (LE bodies) - characteristic nuclear debris in tissue
- Vasculitis, fibrinoid necrosis
2. Kidneys (Lupus Nephritis - most important):
| WHO/ISN Class | Morphology |
|---|---|
| I | Normal |
| II | Mesangial disease |
| III | Focal proliferative GN |
| IV | Diffuse proliferative GN (most severe, most common) |
| V | Membranous GN |
| VI | Sclerotic GN |
- "Wire loop" lesion - immune complex deposits thicken capillary wall
- Hyaline thrombi in glomerular capillaries
- IF: granular ("lumpy-bumpy") deposits of IgG, IgM, C3
- EM: subendothelial deposits
3. Heart (Libman-Sacks Endocarditis):
- Sterile, small, warty vegetations on BOTH sides of mitral valve
- Due to immune complex deposition + fibrin
- Pathognomonic of SLE
4. Blood vessels:
- Fibrinoid necrosis of vessel walls (acute vasculitis)
- "Onion skin" (concentric fibrosis) in chronic cases - especially in spleen (perivascular fibrosis = "onion skin lesion")
5. Spleen:
- Splenomegaly
- "Onion skin" perivascular fibrosis (pathognomonic)
- Lymphoid hyperplasia
6. Lungs:
- Pleuritis (50%), lupus pneumonitis
- Pulmonary fibrosis
7. Joints:
- Non-erosive synovitis (vs. RA which is erosive)
8. CNS (NPSLE):
- Vasculitis, infarcts, diffuse microangiopathy
Diagnosis of SLE (ACR/EULAR Criteria - 2019)
ANA = Entry criterion (must be positive)
Points-based system across 7 domains:
- Constitutional (fever)
- Hematologic (hemolytic anemia, leucopenia, thrombocytopenia)
- Neuropsychiatric (seizures, psychosis)
- Mucocutaneous (malar rash, oral ulcers, photosensitivity, alopecia)
- Serosal (pleuritis, pericarditis)
- Musculoskeletal (arthritis)
- Renal (proteinuria > 0.5 g/day, biopsy findings)
- Immunology (anti-dsDNA, anti-Sm, complement levels, antiphospholipid antibodies)
Score ≥ 10 = SLE diagnosis
Laboratory investigations:
| Test | Significance |
|---|---|
| ANA (FANA) | Screening - 95% sensitive, NOT specific |
| Anti-dsDNA | Specific (70%), correlates with disease activity |
| Anti-Sm | Highly specific (25-30%) |
| Anti-histone | Drug-induced lupus |
| Low C3, C4, CH50 | Active disease |
| CBC | Anemia, leucopenia, thrombocytopenia |
| Urinalysis | Proteinuria, RBC casts |
| Antiphospholipid Ab | VDRL false positive, thrombosis |
MUHS Exam Tip: LE cells = Neutrophil that has engulfed nuclear material opsonized by anti-histone antibodies. LE cell phenomenon = hallmark, but now replaced by ANA testing.
QUESTION 6: HIV - LIFE CYCLE, ETIOPATHOGENESIS, LAB DIAGNOSIS, CLINICAL STAGES OF AIDS, NEOPLASMS ⭐⭐
HIV Genome (Easy to Draw)
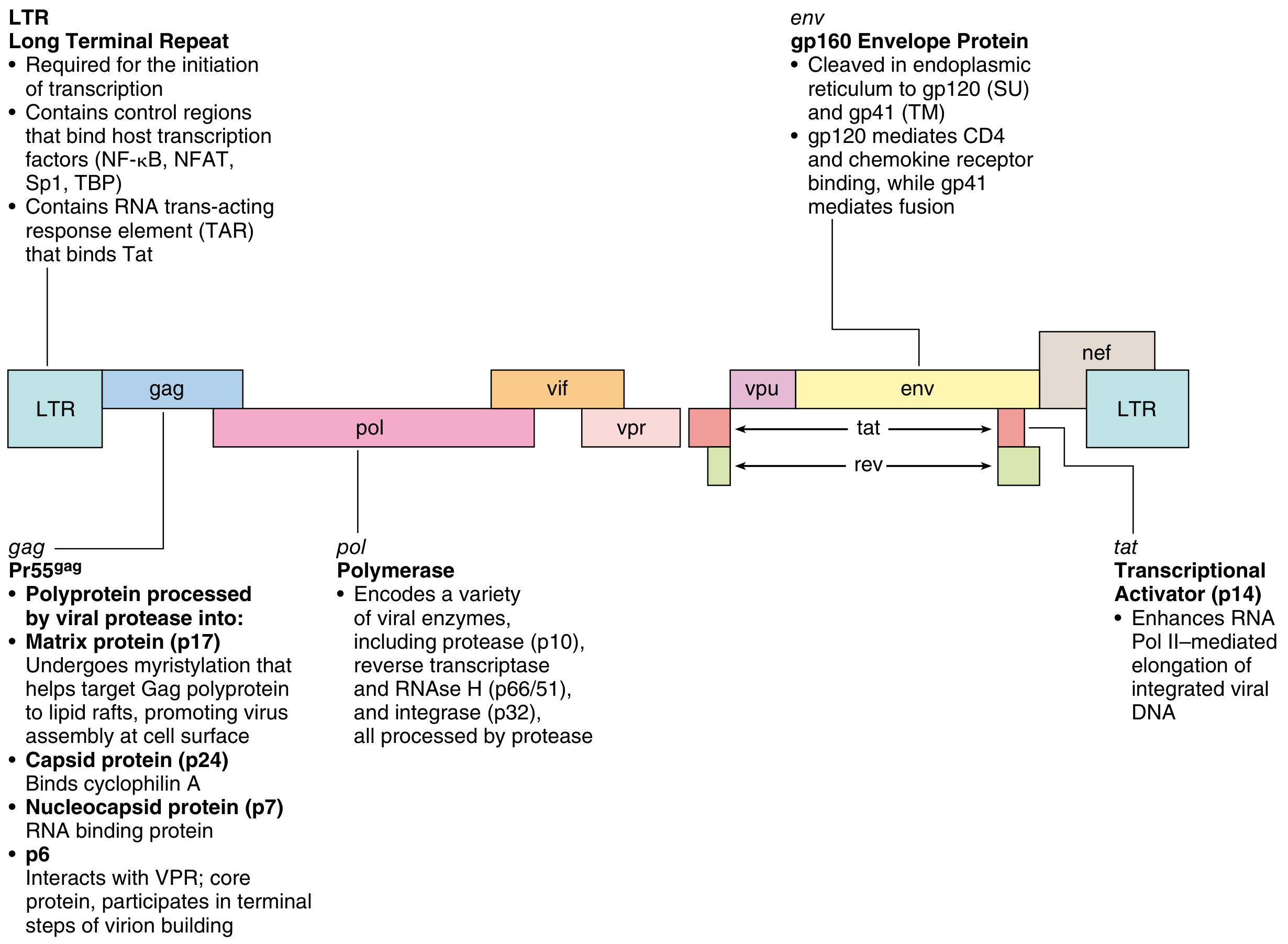
Key genes:
- gag: Encodes core proteins (p24 capsid, p17 matrix, p7 nucleocapsid)
- pol: Encodes enzymes - reverse transcriptase (p66/51), integrase (p32), protease (p10)
- env: Encodes envelope glycoproteins gp160 → cleaved to gp120 (binds CD4) + gp41 (fusion)
- LTR: Long terminal repeats - contain NF-κB, NFAT, Sp1 binding sites; required for transcription
- tat: Transcriptional activator (essential for replication)
- rev: Regulates export of viral mRNA
- nef: Downregulates CD4, MHC-I on infected cells; enhances viral infectivity
- vif: Degrades APOBEC3G (cellular antiviral enzyme)
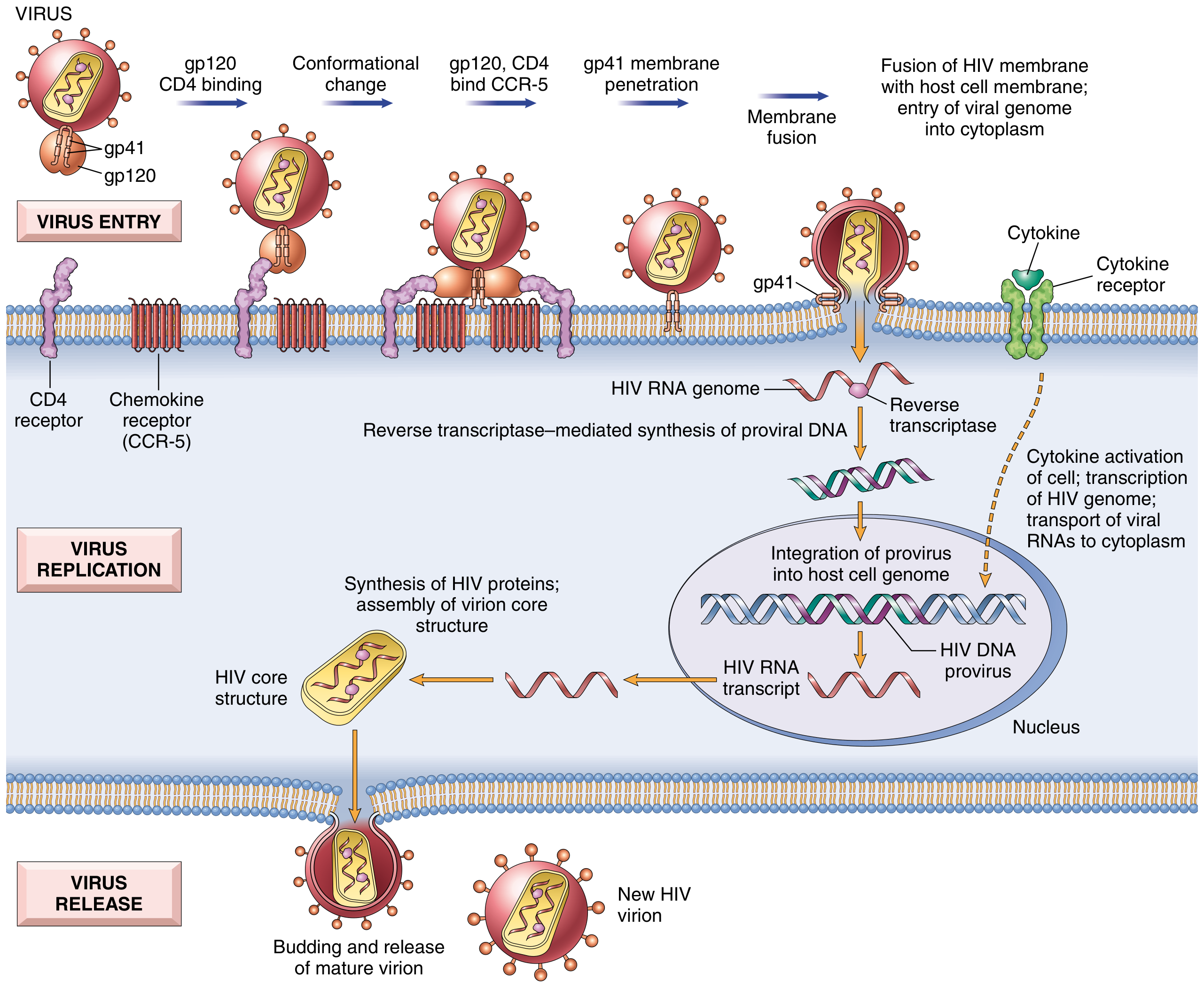
HIV Life Cycle (EASY TO DRAW)
┌─────────────────────────────────────────────────────────────────────┐
│ HIV LIFE CYCLE │
└─────────────────────────────────────────────────────────────────────┘
STEP 1 - ATTACHMENT/ENTRY:
HIV gp120 → binds CD4 receptor (T cells, macrophages, DCs)
↓ Conformational change in gp120
gp120 → binds coreceptor CCR5 (M-tropic, macrophages - early)
or CXCR4 (T-tropic, T cells - late)
↓ Conformational change in gp41
gp41 fusion peptide inserts into cell membrane
↓ Membrane fusion
HIV RNA genome enters cytoplasm
STEP 2 - REVERSE TRANSCRIPTION:
HIV RNA → (Reverse Transcriptase) → dsDNA (proviral DNA)
STEP 3 - INTEGRATION:
Proviral DNA → (Integrase) → integrates into HOST genome
→ LATENT INFECTION (may persist for months/years)
STEP 4 - TRANSCRIPTION (Activation required):
Cell activation (cytokines, infections) → NF-κB activation
→ Transcription of HIV genes via Tat protein
→ HIV mRNA → cytoplasm
STEP 5 - TRANSLATION:
HIV proteins synthesized (Gag, Pol, Env)
→ Core proteins assemble
STEP 6 - BUDDING AND MATURATION:
Immature virus buds from cell membrane
→ Viral Protease cleaves polyproteins
→ Mature infectious HIV virion released
→ CD4+ T cell dies
Drugs targeting each step:
- Entry: Maraviroc (CCR5 antagonist), Enfuvirtide (fusion inhibitor)
- Reverse transcriptase: NRTI (Zidovudine), NNRTI (Nevirapine)
- Integrase: Raltegravir
- Protease: Lopinavir
Etiopathogenesis of AIDS
HIV = Human Immunodeficiency Virus
- Family: Retroviridae, genus Lentivirus
- Types: HIV-1 (worldwide), HIV-2 (West Africa)
- Transmission: Sexual, parenteral (blood/needles), mother-to-child (vertical)
┌─────────────────────────────────────────────────────────────────┐
│ MECHANISMS OF CD4+ T CELL DEPLETION │
└─────────────────────────────────────────────────────────────────┘
DIRECT EFFECTS:
• Productive viral replication → cell lysis
• Accumulation of unintegrated viral DNA → toxic
• HIV-induced apoptosis (via gp120 cross-linking of CD4)
• Formation of syncytia (gp120 on infected cell binds CD4 on uninfected cell)
INDIRECT EFFECTS:
• Immune-mediated killing of HIV-infected T cells by CD8+ CTLs
• Chronic immune activation → activation-induced cell death (AICD)
• Destruction of CD4+ T cell precursors in thymus and bone marrow
• Macrophage and DC dysfunction → impaired antigen presentation
ROLE OF MACROPHAGES AND DCs:
• HIV infects macrophages via CCR5 (early in infection)
• Macrophages are RESERVOIRS of HIV (not killed, virus persists)
• Infected DCs carry virus to lymph nodes → amplify infection
VIRAL LOAD AND CD4 COUNT:
• Normal CD4 = 500-1500 cells/μL
• AIDS defined as CD4 < 200 cells/μL OR AIDS-defining illness
• Viral load correlates with rate of disease progression
Laboratory Diagnosis of HIV
SCREENING TESTS (highly sensitive):
┌─────────────────────────────────────────────────────────┐
│ ELISA (4th generation = detects HIV Ag + Ab together) │
│ • Detects HIV p24 antigen + anti-HIV antibodies │
│ • Window period: ~18 days for 4th gen │
│ • Sensitivity: >99.9% │
└─────────────────────────────────────────────────────────┘
CONFIRMATORY TESTS:
┌─────────────────────────────────────────────────────────┐
│ WESTERN BLOT │
│ • Gold standard confirmatory test │
│ • Detects antibodies to specific viral proteins │
│ • Positive if bands at: p24, gp41, gp120/160 │
└─────────────────────────────────────────────────────────┘
MONITORING TESTS:
• CD4+ T cell count: Immunological status, when to start ART
• HIV RNA viral load (RT-PCR): Treatment response, infectivity
• HIV resistance testing: Guide drug selection
• p24 antigenemia: Early infection, infants
TESTS FOR INFANTS (<18 months):
• HIV DNA PCR or HIV RNA PCR (maternal antibodies persist, ELISA unreliable)
• Positive at 4 weeks → confirmatory test at 4 months
RAPID TESTS:
• Point-of-care, result in 20-30 min
• Used in resource-limited settings, labor/delivery
Clinical Stages of HIV Infection / AIDS
WHO Clinical Staging:
STAGE 1: ACUTE HIV INFECTION (2-4 weeks after exposure)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• Acute retroviral syndrome (mononucleosis-like illness)
• Fever, lymphadenopathy, pharyngitis, rash, myalgia
• High viral load, transient CD4 fall
• Lasts 2-4 weeks, resolves spontaneously
• Anti-HIV antibodies appear (seroconversion)
STAGE 2: CHRONIC ASYMPTOMATIC PHASE (Clinical Latency)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• Typically asymptomatic (may have persistent generalized lymphadenopathy)
• Low-level viral replication in lymph nodes
• Gradual CD4 decline (~50 cells/μL/year)
• Duration: Untreated = 8-10 years (without ART)
• Persistent Generalized Lymphadenopathy (PGL)
STAGE 3: SYMPTOMATIC HIV DISEASE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• Constitutional symptoms: Weight loss, fever, night sweats, diarrhea
• CD4 200-500 cells/μL
• Minor opportunistic infections
• Oral candidiasis, oral hairy leukoplakia (EBV), shingles (VZV)
• Bacterial pneumonias (recurrent)
STAGE 4: AIDS (Full-blown AIDS)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• CD4 < 200 cells/μL OR AIDS-defining illness
• Major opportunistic infections (see below)
• Constitutional: Wasting syndrome (HIV wasting > 10% weight loss)
WHO STAGES: 1 → 2 → 3 → 4 (correlates with CDC classification)
CDC: Category A (acute/asymptomatic) → B (symptomatic) → C (AIDS)
AIDS-Defining Opportunistic Infections by CD4 Count
CD4 < 500: Candida (oral), Kaposi sarcoma, TB reactivation
CD4 < 200: PCP (Pneumocystis jirovecii pneumonia) - MOST COMMON OI
Toxoplasma encephalitis, Cryptococcal meningitis
CD4 < 100: Cryptosporidiosis, Microsporidiosis
CD4 < 50: CMV retinitis, Disseminated MAC (Mycobacterium avium complex)
PML (Progressive Multifocal Leukoencephalopathy - JC virus)
Common Opportunistic Infections:
| System | Pathogen | Presentation |
|---|---|---|
| Lungs | Pneumocystis jirovecii (PCP) | Dry cough, dyspnea, bilateral infiltrates; "ground glass" on HRCT |
| CNS | Toxoplasma gondii | Ring-enhancing lesion on CT; fever, headache, focal neuro signs |
| CNS | Cryptococcus neoformans | Meningitis; India ink = positive; cryptococcal antigen |
| GI | Cryptosporidium | Profuse watery diarrhea |
| Eye | CMV | Retinitis ("pizza pie" appearance); CD4 < 50 |
| Mouth | Candida albicans | White plaques (thrush), pseudomembranous |
| Lungs | MAC (M. avium complex) | Disseminated; fever, weight loss, diarrhea |
| Brain | JC virus (PML) | White matter demyelination; cognitive decline |
| Esophagus | HSV, CMV | Ulcerations |
Neoplasms in AIDS Patients ⭐⭐
25-40% of untreated HIV-infected individuals develop malignancy. All are linked to oncogenic DNA viruses - because HIV-mediated immunosuppression fails to control these latent viruses.
┌──────────────────────────────────────────────────────────────────────┐
│ NEOPLASMS IN AIDS PATIENTS │
├──────────────────┬───────────────┬───────────────────────────────── ┤
│ TUMOR │ VIRUS/CAUSE │ FEATURES │
├──────────────────┼───────────────┼──────────────────────────────────┤
│ KAPOSI SARCOMA │ HHV-8 (KSHV) │ MOST COMMON tumor in AIDS; │
│ ⭐ (KS) │ │ Vascular tumor; purple/red skin │
│ │ │ plaques; also visceral │
├──────────────────┼───────────────┼──────────────────────────────────┤
│ HIGH-GRADE │ EBV │ 2nd most common; diffuse large │
│ B-CELL LYMPHOMA │ │ B cell or Burkitt lymphoma; │
│ │ │ CNS lymphoma (primary) │
├──────────────────┼───────────────┼──────────────────────────────────┤
│ CERVICAL CANCER │ HPV (16, 18) │ In HIV+ women; aggressive course │
├──────────────────┼───────────────┼──────────────────────────────────┤
│ ANAL CANCER │ HPV │ In HIV+ men (MSM) │
├──────────────────┼───────────────┼──────────────────────────────────┤
│ PRIMARY CNS │ EBV │ Ring-enhancing lesion; must │
│ LYMPHOMA │ │ distinguish from toxoplasma │
├──────────────────┼───────────────┼──────────────────────────────────┤
│ PRIMARY │ HHV-8 + EBV │ Pleural/peritoneal effusion; │
│ EFFUSION │ │ Body cavity lymphoma │
│ LYMPHOMA │ │ │
├──────────────────┼───────────────┼──────────────────────────────────┤
│ MULTICENTRIC │ HHV-8 │ B-cell lymphoproliferative; │
│ CASTLEMAN'S │ │ systemic lymphadenopathy │
│ DISEASE │ │ │
└──────────────────┴───────────────┴──────────────────────────────────┘
Kaposi Sarcoma (KS) - Details:
- Most common neoplasm in AIDS patients
- Caused by HHV-8 (human herpesvirus 8 = Kaposi's Sarcoma Herpesvirus, KSHV)
- Morphology: Spindle-shaped cells expressing endothelial + smooth muscle markers; slit-like vascular spaces; mixed inflammatory infiltrate
- Lesions: Purple-red skin plaques (face, extremities, genitals) → disseminates to lungs, GI, lymph nodes
- Incidence fell dramatically with antiretroviral therapy (ART)
- Polyclonal or oligoclonal in early stages (not a true malignant tumor)
- HHV-8 encodes: viral cyclin D homologue, inhibitors of p53 → promotes spindle cell survival
QUICK REVISION SUMMARY FOR MUHS
| Topic | Key Point to Remember |
|---|---|
| Type I HSR | IgE + Mast cells + Histamine + Leukotrienes; SRS-A = LTC4+D4+E4 |
| Type II HSR | IgG/IgM against cell surfaces; complement/phagocytosis |
| Type III HSR | Immune complexes; "lumpy-bumpy" IF; Arthus, serum sickness |
| Type IV HSR | T-cell mediated; DTH; delayed 48-72 hrs; PPD test |
| Graft rejection | Hyperacute = preformed Ab; Acute = T cells; Chronic = both |
| HLA | Class I = HLA-A,B,C (all cells, CD8+); Class II = HLA-DR,DQ,DP (APCs, CD4+) |
| Autoimmunity | Failure of self-tolerance; molecular mimicry; HLA genes |
| SLE | Anti-dsDNA (specific); ANA (sensitive); Wire loop; Libman-Sacks; Onion skin |
| HIV Receptor | gp120 + CD4 + CCR5/CXCR4; gp41 = fusion |
| HIV Stages | Acute → Latent (8-10 yr) → Symptomatic → AIDS (CD4 <200) |
| AIDS tumors | KS (HHV-8); B-cell lymphoma (EBV); Cervical/Anal Ca (HPV) |
| HIV labs | ELISA screen → Western blot confirm; CD4 count + viral load monitor |
Source: Robbins & Kumar Basic Pathology (10th Ed.) and Robbins, Cotran & Kumar Pathologic Basis of Disease (10th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.