Explain me Congenital diaphragmatic hernia from scratch
Reading File
Finding Sources
Finding Sources
Searching PubMed
"congenital diaphragmatic hernia"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have thorough, multi-source content covering all aspects of CDH. Let me compile the comprehensive answer.
Congenital Diaphragmatic Hernia (CDH) - A Complete Guide
What is CDH?
Congenital diaphragmatic hernia (CDH) is a spectrum of developmental conditions in which a defect in the diaphragm allows abdominal contents to herniate into the thoracic cavity, disrupting lung and pulmonary vascular development. The herniated viscera (stomach, bowel, and sometimes liver) compress the developing lungs, leading to the two core pathophysiological problems: pulmonary hypoplasia and pulmonary hypertension.
Epidemiology
- Incidence: approximately 1:2,000 to 1:5,000 live births (some sources report 1:10,000 to 4:10,000)
- Most cases are sporadic, isolated, and non-syndromic
- Left-sided in ~85% of cases (Bochdalek type)
- Right-sided in ~13%
- Bilateral in only ~2%
- When CDH is isolated (no other anomalies): ~60% of cases; when associated with other anomalies, mortality exceeds 85%
- Survival rates with modern neonatal care: 65% to 90% in centers with high-volume, protocolized care
- Sabiston Textbook of Surgery, p. 2675; Creasy & Resnik's Maternal-Fetal Medicine
Embryology - Why Does It Happen?
The diaphragm forms from four embryological structures:
- The septum transversum (central tendon)
- The pleuroperitoneal folds
- Components of the abdominal wall
- The dorsal mesentery of the esophagus
At 3 to 4 weeks of gestation, these structures begin to fuse, separating the pleural and peritoneal cavities. Muscularization from the abdominal wall follows and is typically complete by 9 weeks of gestation.
Incomplete fusion leads to three main defect types:
| Type | Location | Frequency |
|---|---|---|
| Bochdalek hernia | Posterior-lateral | 70-75% |
| Morgagni hernia | Anterior/retrosternal | 23-28% |
| Central hernia | Central | 2-7% |
Several genes (e.g., FOG2, GATA4) share roles in diaphragmatic, pulmonary, cardiac, and foregut development - explaining why CDH is often associated with cardiac defects and gastroesophageal reflux. The etiology is thought to involve genetic, environmental, and nutritional factors.
- Sabiston Textbook of Surgery, p. 2675; Bailey & Love's Short Practice of Surgery
Pathophysiology
Once abdominal contents herniate into the thorax (typically through a Bochdalek defect), a cascade of effects occurs:
1. Pulmonary Hypoplasia
- The ipsilateral lung is most severely compressed
- Both lungs develop fewer bronchial branches, smaller bronchi, and reduced alveolar surface area
- Reduced lung compliance
- Fewer alveoli means reduced gas exchange capacity at birth
2. Pulmonary Vascular Abnormalities
- Increased thickness of arteriolar smooth muscle
- Pulmonary vasculature becomes hypersensitive to vasoactive factors
- Results in persistent pulmonary hypertension of the newborn (PPHN)
3. Right-to-Left Shunting
- Elevated pulmonary vascular resistance causes right-to-left shunting through the foramen ovale and ductus arteriosus
- Leads to profound hypoxemia and worsening acidosis - a vicious cycle
The severity of pulmonary hypoplasia and pulmonary hypertension are the primary determinants of morbidity and mortality.
- Sabiston Textbook of Surgery, p. 2675; Tintinalli's Emergency Medicine
Clinical Presentation
Prenatal (Antenatal)
Routine prenatal ultrasound has enabled diagnosis as early as 15 weeks of gestation.
Sonographic findings (typically at 22-24 weeks):
- Abdominal organs (stomach, bowel, liver) visualized in the chest
- Mediastinal shift away from the defect
- Rightward cardiac deviation in left CDH
- Juxta-cardiac gastric dilatation
- Polyhydramnios
- Absent intra-abdominal stomach bubble
Note: Right-sided CDH is harder to detect because the liver resembles lung on ultrasound; the key clue is leftward cardiac shift.
Postnatal (Neonatal)
The classic triad:
- Respiratory distress - grunting, dyspnea, retractions, cyanosis (the most prominent finding)
- Scaphoid abdomen - because bowel is displaced into the chest
- Bowel sounds in the chest on auscultation
Additional findings:
- Diminished/absent breath sounds on the affected side
- Displaced heart tones
- "Seesaw" or gasping respiratory pattern (due to severely hypoplastic ipsilateral lung)
- Pre-ductal/post-ductal SpO2 difference - indicating right-to-left shunting
Delayed presentations occur in 10-20% of cases (after 24 hours of life), typically with feeding difficulties, recurrent respiratory infections, or pneumonia. Morgagni hernias are often asymptomatic and diagnosed in childhood.
- Sabiston Textbook of Surgery, p. 2676; Tintinalli's Emergency Medicine
Diagnosis
Prenatal Assessment
1. Lung-to-Head Ratio (LHR)
Calculated as: contralateral lung area / head circumference on ultrasound.
| LHR Value | Prognosis |
|---|---|
| < 1.0 | Poor (only ~11% survival without intervention) |
| 1.0 - 1.4 | Moderate |
| > 1.4 | Near 100% survival |
More refined is the Observed/Expected LHR (O/E LHR):
- O/E LHR < 25% → less than 20% survival without intervention
- O/E LHR 25-34.9% → moderate pulmonary hypoplasia
2. Liver position - "liver-up" (herniated into chest) worsens prognosis significantly.
3. Fetal MRI - not limited by maternal habitus or fetal position; provides total fetal lung volume (TFLV) and allows quantification of liver herniation as a continuous variable rather than binary (liver up/liver down).
4. Genetic testing - Chromosomal abnormalities (trisomies, microdeletions) identified in ~6.3% of CDH cases. Array comparative genomic hybridization is currently applicable.
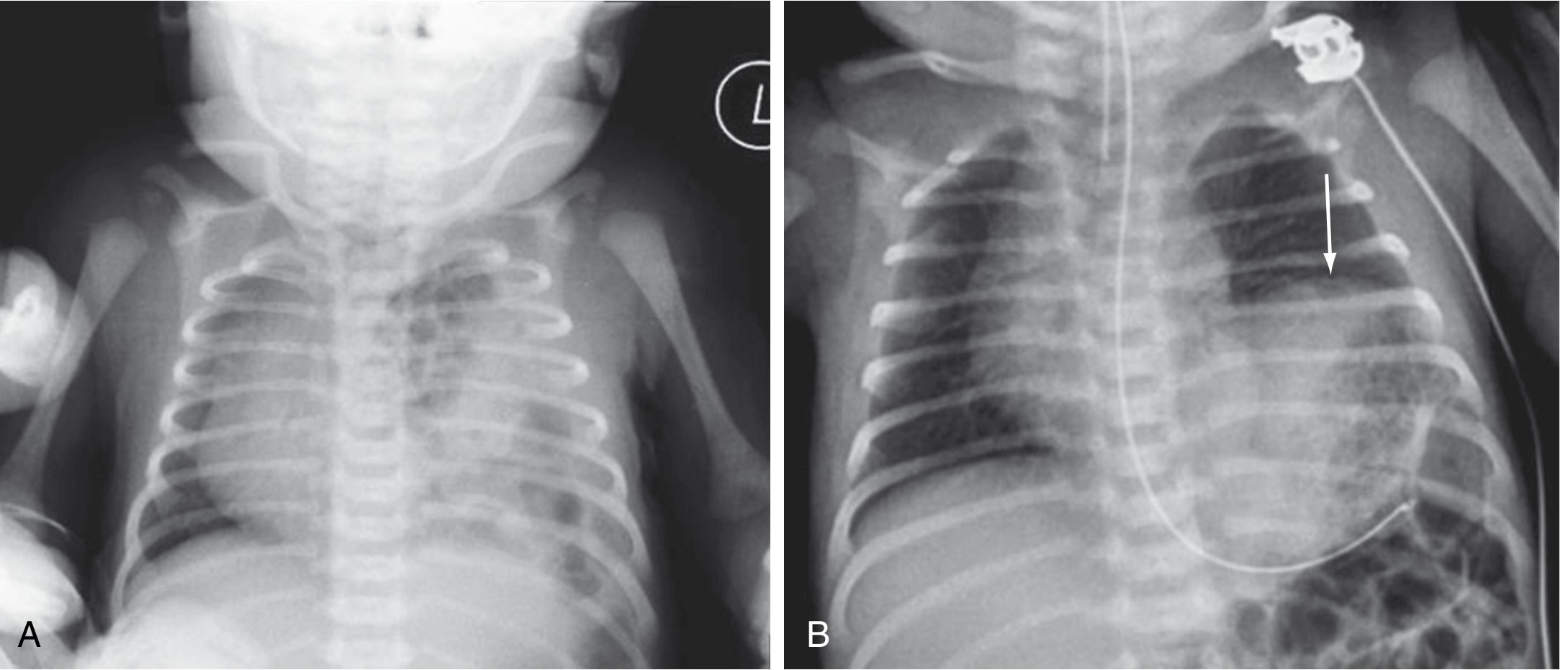
Postnatal
- Chest X-ray: gas-filled bowel loops in the hemithorax, mediastinal shift, absent/small ipsilateral diaphragmatic shadow
- Blood gas: hypoxemia, hypercarbia, respiratory/metabolic acidosis
- Pre- and post-ductal pulse oximetry difference confirms right-to-left ductal shunting
Prognostic Factors (Summary)
| Factor | Better Prognosis | Worse Prognosis |
|---|---|---|
| Side | Right-sided | Left-sided |
| Liver position | Liver-down | Liver-up (in chest) |
| O/E LHR | > 35% | < 25% |
| Anomalies | Isolated CDH | Associated cardiac/chromosomal |
| Total lung volume | > 45% of normal | Severely reduced |
| Diagnosis timing | After 24h (delayed) | Prenatally (implies severe defect) |
Management
A. Prenatal Intervention - FETO
Fetoscopic Endoluminal Tracheal Occlusion (FETO) is the key fetal intervention for severe CDH.
Mechanism: Placing a detachable balloon in the fetal trachea (typically 27-29 weeks) prevents egress of fetal lung fluid. Fluid accumulates, increasing airway pressure and stimulating lung growth. The balloon is removed a few weeks later (before 34 weeks).
Evidence - TOTAL Trials (landmark RCTs):
- Severe CDH (O/E LHR < 25%): TOTAL trial stopped early for efficacy - FETO achieved 40% survival to discharge vs. 15% with expectant management. Benefit sustained at 6 months.
- Moderate CDH (O/E LHR 25-34.9%): No significant survival benefit demonstrated.
Complications of FETO: preterm labor, premature rupture of membranes, premature birth, fetal demise, tracheal injury.
- Sabiston Textbook of Surgery, p. 2716; Creasy & Resnik's Maternal-Fetal Medicine
B. Postnatal - Immediate Stabilization ("Gentle Ventilation First")
The key principle: CDH is NOT a surgical emergency. Stabilization precedes repair.
Unlike traumatic diaphragmatic hernias, urgently reducing herniated bowel does NOT improve gas exchange in CDH. The lungs are anatomically hypoplastic - reducing the hernia doesn't change the underlying lung size immediately.
Step 1: Airway
- Immediate endotracheal intubation (avoid bag-mask ventilation - this inflates the GI tract in the chest and worsens compression)
- Ventilate at 40-50 breaths/min with lowest effective peak inspiratory pressures (minimize barotrauma to hypoplastic lungs)
Step 2: GI Decompression
- Large-bore (10F) orogastric tube on continuous low suction to decompress herniated bowel and reduce lung compression
Step 3: "Gentilation" - Permissive Hypercapnia
- Target gentle ventilation with permissive hypercapnia (PaCO2 45-60 mmHg acceptable)
- Avoid aggressive ventilation that causes barotrauma/volutrauma
- High-frequency oscillatory ventilation (HFOV) may be used if conventional ventilation fails
Step 4: Treat Pulmonary Hypertension
- Inhaled nitric oxide (iNO): pulmonary vasodilator - first-line
- Sildenafil: phosphodiesterase-5 inhibitor, reduces pulmonary vascular resistance
- Milrinone: inodilator, addresses cardiac dysfunction
- Prostaglandin E1 (PGE1) and prostacyclin (PGI2): vasodilation in select refractory cases
- Aim for preductal SpO2 > 85%, pH > 7.25
Step 5: ECMO (Extracorporeal Membrane Oxygenation)
- For severe pulmonary hypertension unresponsive to above measures
- Bridge to surgical repair
- Reserved for patients failing maximal medical management
- Sabiston Textbook of Surgery, p. 2676; Bailey & Love's; Tintinalli's Emergency Medicine
C. Surgical Repair
Timing: Deferred until pulmonary circulation stabilizes (typically 48-72 hours after birth, or after weaning from ECMO in severe cases). There is no benefit to emergency repair.
Approach options:
- Abdominal (open or laparoscopic) - most common
- Thoracic (open or thoracoscopic)
Technique:
- Herniated viscera are reduced back into the abdomen
- Diaphragmatic defect is repaired:
- Small defect: primary suture repair (a few non-absorbable sutures)
- Large defect: patch repair using Silastic (conical) or Gore-Tex (PTFE) patch - to close without tension
- A hernia sac (present in minority) may be removed or plicated
- Bailey & Love's Short Practice of Surgery; Sabiston Textbook of Surgery
Associated Anomalies & Complications
Associated Anomalies (seen in 25-50% of CDH patients):
- Congenital heart disease (most common)
- Chromosomal abnormalities (trisomies 18, 21, 13)
- Neural tube defects
- Genitourinary anomalies
Long-term Morbidities in Survivors:
- Gastroesophageal reflux (GER): very common, often requiring medical or surgical management
- Bronchopulmonary dysplasia (BPD) and chronic lung disease
- Persistent pulmonary hypertension
- Feeding difficulties and growth failure
- Thoracic deformities after repair
- Neurodevelopmental delays
- Hernia recurrence (especially with patch repairs)
- Creasy & Resnik's Maternal-Fetal Medicine; Sabiston Textbook of Surgery
Quick Summary Table
| Feature | Details |
|---|---|
| Definition | Diaphragmatic defect allowing abdominal contents into thorax |
| Incidence | 1:2,000-5,000 births |
| Most common type | Left-sided Bochdalek (70-75%) |
| Key pathophysiology | Pulmonary hypoplasia + pulmonary hypertension |
| Prenatal diagnosis | Ultrasound (15-24 weeks), MRI |
| Best prognostic tool | O/E LHR + liver position |
| Fetal intervention | FETO (for severe: O/E LHR <25%) |
| Postnatal principle | Stabilize FIRST, then repair |
| Key neonatal danger | Avoid bag-mask ventilation |
| Surgical repair | Primary suture (small) or patch (large defect) |
| Survival (modern) | 65-90% |
Sources: Sabiston Textbook of Surgery (21st/22nd ed.), Creasy & Resnik's Maternal-Fetal Medicine (8th ed.), Bailey & Love's Short Practice of Surgery (28th ed.), Tintinalli's Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.