de novo synthesis for purine (nmemonic )\
Reading File
Searching the Web
de novo purine synthesis mnemonic steps
Finding Sources
Reading File
Reading File
Here is a complete, exam-ready breakdown of de novo purine synthesis with mnemonics at every level:
De Novo Purine Synthesis - Complete Mnemonic Guide
The Big Picture
Purines are built on top of ribose-5-phosphate (not made separately and then attached). The end product is IMP (Inosine Monophosphate), which then branches to AMP and GMP.
Site: Primarily the liver (cytosol)
Atom Origin Mnemonic: "GAG CO2 T"
Remember what contributes atoms to the purine ring:
| Contributor | Atoms Donated |
|---|---|
| Glutamine (×2) | N3, N9 |
| Aspartate | N1 |
| Glycine | C4, C5, N7 |
| CO₂ | C6 |
| THF (N¹⁰-formyl-THF ×2) | C2, C8 |
Mnemonic: "Granny Always Gets COugh Twice"
- Granny = Glutamine (×2 nitrogens)
- Always = Aspartate (N1)
- Gets = Glycine (C4, C5, N7)
- COugh = CO₂ (C6)
- Twice = THF ×2 (C2, C8)
The 10 Steps: PRPP → IMP
Classic step mnemonic:
"Prices Paid Going For Asking, Forget All Funny Stupid Intermediates"
| # | Mnemonic Word | Reaction | Key Molecule Added |
|---|---|---|---|
| 0 | Prices | R5P → PRPP | PRPP synthetase (needs ATP) |
| 1 | Paid | PRPP → PRA | Glutamine donates N9 (committed step - GPAT enzyme) |
| 2 | Going | PRA → GAR | Glycine added (C4, C5, N7) |
| 3 | For | GAR → FGAR | Formyl-THF adds C8 |
| 4 | Asking | FGAR → FGAM | Glutamine donates N3 |
| 5 | Forget | FGAM → AIR | Ring closes (ATP used) |
| 6 | All | AIR → CAIR | CO₂ added at C6 |
| 7 | Funny | CAIR → SAICAR | Aspartate added (carries N1) |
| 8 | Stupid | SAICAR → AICAR | Fumarate leaves (N1 stays) |
| 9 | Intermediates | AICAR → FAICAR | Formyl-THF adds C2 |
| 10 | (Ring closes) | FAICAR → IMP | Cyclization, water lost |
Committed Step - Key Exam Fact
Step 1: PRPP + Glutamine → Phosphoribosylamine (PRA)
- Enzyme: Glutamine PRPP Amidotransferase (GPAT)
- Inhibited by: AMP, GMP, IMP (negative feedback)
- This is the rate-limiting / committed step
IMP → AMP and GMP (Branching)
Mnemonic: "AMP needs GTP, GMP needs ATP" (they use each other's energy - cross-regulation)
| Branch | Steps | Energy |
|---|---|---|
| IMP → Adenylosuccinate → AMP | Aspartate added, fumarate leaves | Needs GTP |
| IMP → XMP → GMP | IMP dehydrogenase (IMPDH) | Needs ATP |
Drugs here:
- Mycophenolate & Ribavirin - inhibit IMP dehydrogenase (block GMP synthesis)
- 6-MP / Azathioprine - block multiple steps (GPAT and HGPRT salvage)
Regulation Summary Mnemonic: "PRPP is the GAS, purines are the BRAKES"
- PRPP concentration - drives synthesis (more PRPP = faster synthesis)
- AMP + GMP (+ IMP) - feedback-inhibit GPAT (the committed step)
- PRPP synthetase is also inhibited by purine nucleotides
Quick Recall Summary
R5P → PRPP → PRA → ... (9 more steps) ... → IMP → AMP
↘ GMP
Energy cost: 5 ATP equivalents to make IMP from R5P
Carbons and nitrogens from:
- Glycine (backbone: C4, C5, N7)
- Glutamine ×2 (N3, N9)
- Aspartate (N1)
- CO₂ (C6)
- Formyl-THF ×2 (C2, C8)
One-liner Super Mnemonic (for atom origins)
"A Glut of CO₂ from Glycine Fumes Twice"
= Aspartate, Glutamine (×2), CO₂, Glycine, Formyl-THF (×2)
Sources: Lippincott's Illustrated Reviews Biochemistry, 8th ed.; Basic Medical Biochemistry: A Clinical Approach, 6th ed.
regulation of purine synthesis
Reading File
Reading File
Loading Image
Loading Image
Here is the complete regulation of de novo purine synthesis, drawn directly from the textbooks:
Regulation of De Novo Purine Synthesis
There are 4 key regulated enzymes - 2 control IMP synthesis, 2 control the AMP/GMP branch point.
Overview Diagram
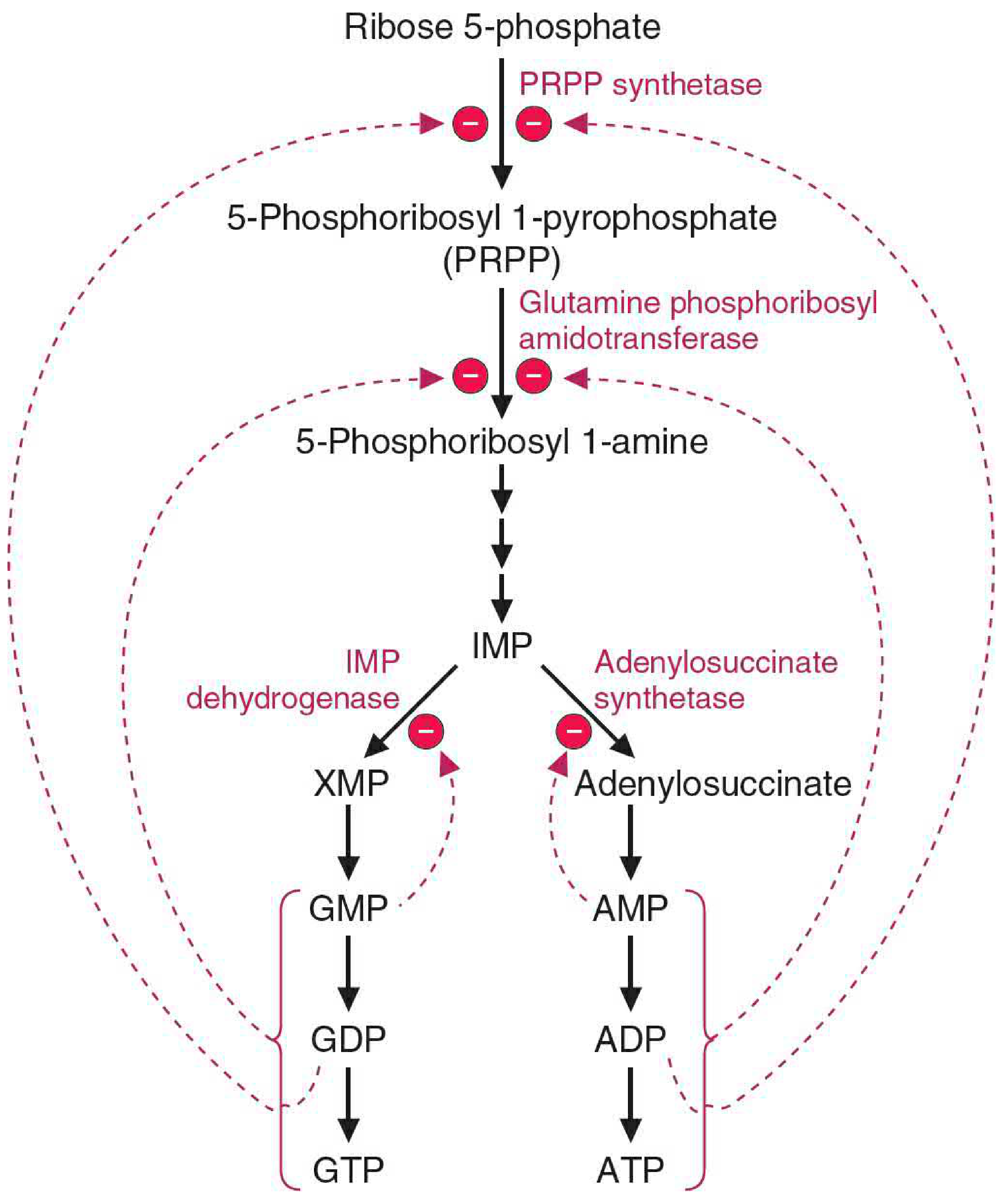
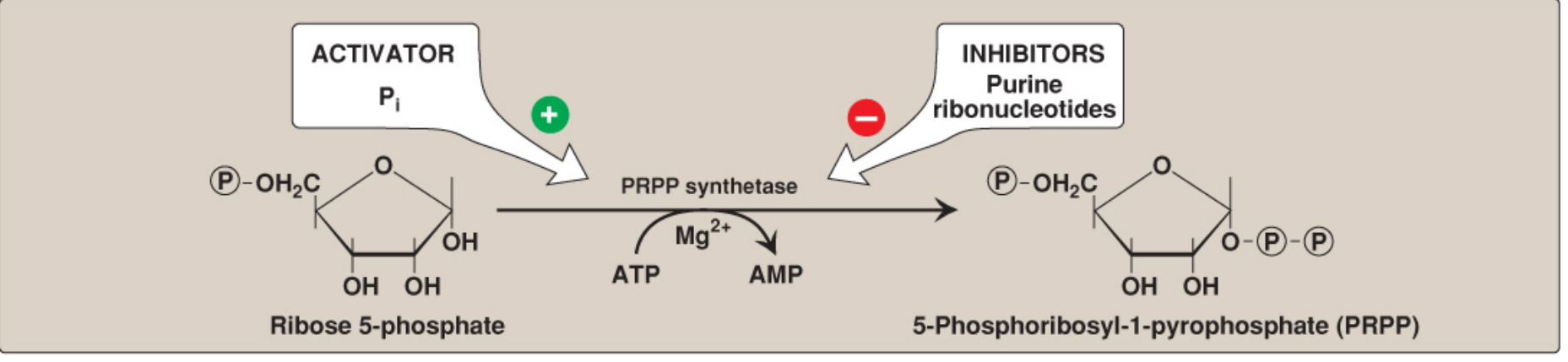
Level 1: PRPP Synthetase (R5P → PRPP)
| Regulator | Effect | |
|---|---|---|
| Activated by | Inorganic phosphate (Pi) | Stimulates synthesis |
| Inhibited by | ADP, GDP (purine ribonucleotides) | End-product inhibition |
Key point: This is an X-linked enzyme. It is not the committed step (PRPP is also used in pyrimidine synthesis and salvage pathways). Both an oxypurine (GDP) and aminopurine (ADP) bind a single allosteric site to inhibit it.
Level 2: Glutamine PRPP Amidotransferase - GPAT (PRPP → PRA) ⭐ COMMITTED STEP
This is the rate-limiting, committed step - the most important regulatory point.
| Regulator | Effect | |
|---|---|---|
| Inhibited by | AMP + GMP (bind distinct allosteric sites) | Strong feedback inhibition |
| Also inhibited by | ADP, GDP, ATP, GTP | Less physiologically significant |
Mechanism of inhibition: AMP and GMP convert the enzyme from an active monomer (133 kDa) → inactive dimer (270 kDa).
Mnemonic: "GPAT is GAG-ged" - GMP and AMP and Glutamine act at GPAT
Key kinetic trick: Cellular PRPP and glutamine concentrations are normally below their Km for GPAT. So any small rise in PRPP or glutamine causes a proportional increase in synthesis rate - this is how the pathway is "accelerated" when needed.
Level 3: Branch Point Regulation (IMP → AMP or GMP)
This is where cross-regulation creates balance between the two end products:
Mnemonic: "AMP needs GTP, GMP needs ATP" - they require each other's energy
| Branch | Enzyme | Inhibited By | Energy Used |
|---|---|---|---|
| IMP → Adenylosuccinate → AMP | Adenylosuccinate synthetase | AMP (feedback) | GTP |
| IMP → XMP → GMP | IMP dehydrogenase (IMPDH) | GMP (feedback) | ATP |
Why this is brilliant:
- When ATP is high → more GTP available → drives GMP synthesis → balances the pool
- When GTP is high → more ATP available → drives AMP synthesis → balances the pool
- This is reciprocal/cross-regulation ensuring neither purine dominates
Complete Regulation Summary Table
| Enzyme | Activated By | Inhibited By | Step |
|---|---|---|---|
| PRPP synthetase | Pi | ADP, GDP | R5P → PRPP |
| GPAT (committed step) | PRPP ↑, Glutamine ↑ | AMP, GMP (+ di/triphosphates) | PRPP → PRA |
| Adenylosuccinate synthetase | GTP (substrate) | AMP | IMP → AMP |
| IMP dehydrogenase (IMPDH) | - | GMP | IMP → GMP |
Clinical Pharmacology: Drugs That Exploit This Regulation
| Drug | Target | Use |
|---|---|---|
| 6-Mercaptopurine (6-MP) | Blocks GPAT + multiple steps (false feedback inhibition) | Leukemia, IBD |
| Azathioprine | Prodrug of 6-MP | Immunosuppression, IBD |
| Mycophenolate | Inhibits IMP dehydrogenase (blocks GMP branch) | Transplant rejection |
| Ribavirin | Inhibits IMP dehydrogenase | Viral infections (HCV) |
| Methotrexate | Inhibits DHFR → depletes formyl-THF → blocks steps 3 & 9 | Cancer, RA |
| Allopurinol | Inhibits xanthine oxidase (degrades purines) | Gout |
One-Line Summary Mnemonic
"PRPP GAS, AMP+GMP BRAKES, Cross-roads at IMP"
- PRPP = accelerator (more PRPP = faster synthesis)
- AMP + GMP = dual brakes on GPAT (committed step)
- IMP = crossroads where AMP inhibits its own branch, GMP inhibits its own branch, but each needs the other's energy to be made
Sources: Basic Medical Biochemistry: A Clinical Approach 6e, p.1420-1421; Lippincott's Illustrated Reviews Biochemistry 8e, p.827-829
gout reasons for precipitating feature
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent content gathered. Here is the complete answer:
Gout: Precipitating Factors - Complete Guide
Understanding WHY Attacks Are Triggered
A gout flare does not simply require hyperuricemia - it needs a sudden change (rise or fall) in urate levels, or local factors that promote crystal formation or crystal shedding from existing deposits. Most people with hyperuricemia never get gout.
The Master Framework: Two Levels of Precipitation
Mnemonic: "CRYSTAL DROPS"
Cold temperature (local)
Rapid urate change (up or down)
Yield of purines from diet
Surgery / trauma
Thiazides and other drugs
Alcohol
Low pH / dehydration
Dehydration (intraarticular)
Renal impairment
Overproduction states (tumor lysis, haemolysis)
Precipitate starters - seed nuclei (cartilage debris, OA)
Starting urate-lowering therapy
Level 1: Causes of Hyperuricemia (Root Cause)
Mnemonic: "90% Under, 10% Over"
- >90% of gout = underexcretion of uric acid by kidneys
- <10% = overproduction (or combined)
A) Underexcretion Causes (RENAL)
| Category | Examples |
|---|---|
| Drugs | Thiazide diuretics, loop diuretics, low-dose aspirin, cyclosporine, pyrazinamide, ethambutol |
| Renal disease | CKD, chronic renal insufficiency |
| Metabolic | Hypertension, metabolic syndrome, insulin resistance |
| Dehydration | Any cause - reduces uric acid clearance |
| Organic acids compete | Lactic acidosis (alcohol, starvation), ketoacidosis (fasting, DKA) - organic acids compete with urate at renal tubule for excretion |
B) Overproduction Causes
| Category | Examples |
|---|---|
| Dietary | Purine-rich foods: red meats, organ meats, shellfish, anchovies, beer |
| Cell lysis | Tumor lysis syndrome, haemolytic anaemia, psoriasis, myeloproliferative disorders |
| Enzyme defects | HGPRT deficiency (Lesch-Nyhan), PRPP synthetase overactivity |
| High fructose intake | High-fructose corn syrup - accelerates purine degradation |
Level 2: Local Crystal Formation Promoters
From Rheumatology (2022 Elsevier) - Box 193.3:
| Promoter | Mechanism |
|---|---|
| Low temperature | MSU crystals precipitate preferentially in cooler peripheral joints (1st MTP, ankle) |
| Low pH | Acidic environment reduces urate solubility |
| Dehydration | Raises local urate concentration |
| Seed nuclei | Cartilage debris, chondroitin, hyaluronate from joint trauma or OA |
| Cation concentration | High Na⁺ promotes MSU crystal nucleation |
| IgG coat | Immunoglobulins provide stable platform for crystal nucleation |
| Osteoarthritis | OA cartilage releases chondroitin sulphate, lowers urate solubility; OA sites co-localise with MSU deposits |
Level 3: Triggers of the Acute Flare (Precipitating Events)
Mnemonic: "SAT DISH"
| Letter | Trigger | Mechanism |
|---|---|---|
| S | Surgery / Postoperative | Rapid fluid shifts, fasting, dehydration, tissue trauma |
| A | Alcohol (especially beer) | Beer = purines + lactic acid (competes at tubule); spirits = dehydration |
| T | Trauma (local) | Crystal shedding from deposits; seed nuclei released |
| D | Dietary binge / Fasting | Binge = purine load; fasting = ketoacidosis competes at tubule |
| I | Intercurrent illness / Infection | Fever, dehydration, systemic inflammation mobilise crystals |
| S | Starting ULT (allopurinol, febuxostat) | Rapid fall in urate causes crystal remodelling and shedding from tophi |
| H | Hospitalisation / Severe illness | NPO status, IV fluids, diuretics - all shift urate rapidly |
The Paradox of Starting Urate-Lowering Therapy
A key exam point: initiating allopurinol or febuxostat paradoxically triggers acute gout flares in the first weeks-months. This happens because:
- Rapid fall in serum urate destabilises existing MSU crystal deposits in tophi
- Crystals are shed into the joint space
- This triggers the same inflammasome-mediated response as new crystal deposition
- Prevention: always co-prescribe colchicine or NSAID prophylaxis for 3-6 months when starting ULT
Pathophysiology of the Flare: The Inflammasome Cascade
Once crystals form or are shed, the sequence is:
MSU crystals in joint
↓
Phagocytosed by synovial macrophages
↓
NLRP3 Inflammasome activated
↓
Caspase-1 activated
↓
IL-1β released (+ IL-6, TNF, complement)
↓
Neutrophil recruitment → lysosomal enzyme release
↓
ACUTE ARTHRITIS (peaks 8-12 hrs, resolves in days-weeks)
Why Night / Early Morning?
Flares characteristically start at night or early morning because:
- Nocturnal dehydration concentrates urate in joint fluid
- Body temperature drops slightly during sleep (promotes MSU crystallisation)
- Cortisol is at its nadir (less natural anti-inflammatory effect)
High-Yield Summary Table
| Precipitant | Category | Mechanism |
|---|---|---|
| Thiazide diuretics | Drug - underexcretion | Compete with urate at proximal tubule |
| Alcohol (beer > spirits) | Dietary + metabolic | Purine load + lactic acidosis + dehydration |
| High-purine diet | Dietary - overproduction | Excess substrate for xanthine oxidase |
| Dehydration | Metabolic | ↑ urate concentration, ↓ renal clearance |
| Surgery | Systemic event | Fasting + fluid shifts + tissue breakdown |
| Trauma | Local event | Crystal shedding + seed nuclei |
| Starting allopurinol | Iatrogenic | Rapid urate fall → crystal remodelling |
| Tumor lysis / chemo | Overproduction | Massive purine release from cell lysis |
| Low-dose aspirin | Drug - underexcretion | Blocks urate secretion at tubule |
| Cyclosporine | Drug - underexcretion | ↓ GFR + ↑ tubular reabsorption |
| Fasting / crash diet | Metabolic | Ketoacidosis competes with urate excretion |
| Cold weather | Local | ↓ temperature → ↓ MSU solubility |
Sources: Goldman-Cecil Medicine International Edition; Rheumatology 2-Volume Set (2022, Elsevier); Robbins & Kumar Basic Pathology; ROSEN's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.