Opioid detailed pharmacology
Reading File
Finding Sources
Finding Sources
Searching the Web
opioid pharmacology receptors mechanisms tolerance dependence 2024
Reading File
Reading File
Finding Sources
Searching PubMed
opioid pharmacology receptor signaling tolerance
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have rich content from Goodman & Gilman, Bradley & Daroff, Goldman-Cecil, Adams & Victor, Katzung, and Kandel's Neuroscience. Let me compile the comprehensive answer now:
Opioid Pharmacology - Detailed Review
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics | Bradley and Daroff's Neurology | Goldman-Cecil Medicine | Adams & Victor's Neurology | Katzung's Basic & Clinical Pharmacology | Kandel's Principles of Neural Science
1. Terminology
| Term | Definition |
|---|---|
| Opiate | Natural or semisynthetic compounds derived from opium (morphine, codeine, oxycodone) |
| Opioid | Broader term - any agent binding to opioid receptors, including fully synthetic drugs (fentanyl, methadone) and endogenous peptides |
| Narcotic | From Greek narkotikos ("stupor"); refers to opioids' sedative/analgesic properties |
2. Opioid Receptors
Opioid receptors are 7-transmembrane G protein-coupled receptors (GPCRs), class A (rhodopsin family). There are four types:
| Receptor | Gene | Chromosome | Primary Endogenous Ligand | Main Functions |
|---|---|---|---|---|
| Mu (μ) | OPRM1 | 6 | β-endorphin, enkephalins | Analgesia, euphoria, respiratory depression, constipation, tolerance/dependence |
| Delta (δ) | OPRD1 | 1 | Enkephalins | Analgesia (inflammatory, bone pain), mood modulation |
| Kappa (κ) | OPRK1 | 8 | Dynorphins | Visceral/neuropathic analgesia, dysphoria, diuresis, stress response |
| NOP/ORL1 | OPRL1 | 20 | Nociceptin/orphanin FQ | Pain modulation, anxiety, stress, memory, feeding - naloxone-insensitive |
The three classical receptors share 55-58% sequence homology. NOPr shares 48-49% homology but has distinct pharmacology.
Mu-receptor subtypes:
- μ1 (supraspinal) - analgesia, euphoria
- μ2 (spinal) - respiratory depression, constipation
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 463
3. Receptor Distribution
Mu receptors: Neocortex, caudate-putamen, nucleus accumbens, VTA, thalamus, hippocampus, amygdala, raphe nucleus, periaqueductal gray (PAG), medulla/pons, dorsal horn of spinal cord, peripheral nerves and skin.
Kappa receptors: Caudate-putamen, nucleus accumbens, amygdala, hypothalamus, pituitary, PAG. Important for stress responses.
Delta receptors: Olfactory cortex, neocortex, caudate-putamen, nucleus accumbens, amygdala. Sparse in dorsal horn.
Non-neuronal: Macrophages, microglia, astrocytes, enteric nervous system of the GI tract. Delta receptors in the heart may afford cardioprotection.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 463
4. Signal Transduction Mechanisms
All classical opioid receptors couple to Gi/Go heterotrimeric G proteins (inhibitory). After agonist binding, both α and βγ subunits transduce signals:
Acute effects of opioid receptor activation:
- Inhibition of adenylyl cyclase → ↓ cAMP → ↓ protein kinase A activity
- Activation of inward-rectifying K+ channels (GIRK) → membrane hyperpolarization → neuronal inhibition
- Inhibition of voltage-gated Ca2+ channels (N-type, P/Q-type) → ↓ presynaptic neurotransmitter release
- Inhibition of substance P and glutamate release presynaptically
Net result: Reduced nociceptive signal transmission at peripheral terminals, spinal dorsal horn, and supraspinal centers.
- Bradley and Daroff's Neurology in Clinical Practice, p. 1084; Goodman & Gilman
5. Endogenous Opioid System
Three major endogenous opioid peptide families:
| Peptide Family | Precursor | Preferred Receptor |
|---|---|---|
| Enkephalins (met-, leu-) | Proenkephalin | δ > μ |
| Endorphins (β-endorphin) | Proopiomelanocortin (POMC) | μ >> δ |
| Dynorphins | Prodynorphin | κ |
6. Drug Classification by Receptor Activity
Full Agonists (μ)
Hydrocodone, codeine, morphine, oxycodone, hydromorphone, methadone, fentanyl, oxymorphone, heroin
Partial Agonist
Buprenorphine - lower intrinsic efficacy than full agonists; ceiling effect to analgesia and respiratory depression. Acts as partial agonist at μ and antagonist at κ.
Mixed Agonist-Antagonists
Pentazocine, butorphanol, nalbuphine, dezocine - antagonize μ receptors while activating κ receptors.
CRITICAL: Never combine with full agonists - can precipitate acute withdrawal and worsen pain.
Antagonists
Naloxone (short-acting, IV) - used for overdose reversal
Naltrexone (oral, long-acting) - used for opioid use disorder maintenance
Atypical Dual-Mechanism Agents
- Tramadol: Weak μ agonist + inhibits norepinephrine and serotonin reuptake. Risk of seizures. Has a ceiling effect.
- Tapentadol: ~2x stronger than tramadol; μ agonist (with ceiling effect) + norepinephrine reuptake inhibitor.
- Bradley and Daroff's Neurology in Clinical Practice, p. 1090; Goldman-Cecil Medicine, p. 272
7. Pharmacological Effects of Opioids
CNS Effects
| Effect | Mechanism/Site |
|---|---|
| Analgesia | PAG (supraspinal), dorsal horn (spinal), peripheral (μ1, δ, κ) |
| Euphoria | Mesolimbic dopamine release - nucleus accumbens, VTA |
| Sedation | CNS depression |
| Miosis | Edinger-Westphal nucleus (μ, κ) - pinpoint pupils in overdose |
| Nausea/Vomiting | Chemoreceptor trigger zone (CTZ) activation |
| Cough suppression | Medullary cough center |
| Dysphoria | κ-receptor activation |
Respiratory System
Respiratory depression - the most dangerous acute effect; mediated via μ2 receptors in the pre-Bötzinger complex (medullary respiratory rhythm generator). Opioids decrease respiratory rate, tidal volume, and blunt the response to CO2. This is the cause of death in overdose.
Cardiovascular
Generally minimal at therapeutic doses. High doses cause bradycardia and hypotension.
GI Effects
- Constipation (μ2 receptors in enteric NS) - does NOT develop tolerance
- ↓ GI motility and secretion
- Spasm of sphincter of Oddi (biliary system)
- Nausea/vomiting early in treatment
Endocrine
- ↓ GnRH, LH, FSH → hypogonadism, sexual dysfunction
- ↑ prolactin, ADH
- Chronic use → accelerated osteoporosis
Genitourinary
- Urinary retention (↓ detrusor tone, ↑ sphincter tone)
Pruritus
- Histamine release (morphine > others); also central μ receptor mechanism
- Not prevented by antihistamines when central
8. Individual Drugs - Key Pharmacology
Morphine (Prototype)
- Onset: Rapid (especially IV); Duration: 2-4 hours
- Oral bioavailability: ~25% (high first-pass metabolism)
- Metabolism: Liver glucuronidation → morphine-6-glucuronide (M6G) (active, accumulates in renal failure) + morphine-3-glucuronide (M3G)
- Caution in renal failure - M6G accumulates → prolonged respiratory depression
- Sustained release: MS Contin (12h), Kadian (24h)
Fentanyl
- 100x more potent than morphine
- Highly lipophilic → rapid CNS penetration; short duration with IV bolus
- Transdermal patch: 12, 25, 50, 75, 100 μg/h; plasma levels rise over 12-18 hours; 72-hour patch; elimination half-life ~21 hours
- Safe in renal failure (hepatic metabolism to inactive metabolites)
- Illicit fentanyl analogues (carfentanil) driving overdose epidemic
Codeine
- Prodrug - converted to morphine by CYP2D6
- Ultrarapid metabolizers (CYP2D6 duplications) can develop acute morphine toxicity
- Poor metabolizers get no analgesia
- Antitussive action partially independent of conversion
Methadone
- Long-acting μ agonist + NMDA receptor antagonist
- Highly variable half-life: 4-130 hours
- Slow onset of peak effect (~2-6 hours)
- Oral bioavailability ~80%
- QTc prolongation risk (blocks hERG K+ channels) → arrhythmia
- Used for maintenance treatment of OUD; doses ≥60 mg/day more effective
- Reduces craving and induces cross-tolerance to other opioids
- Safe in renal failure
Meperidine (Pethidine)
- Active metabolite normeperidine accumulates → myoclonus, seizures, dysphoria
- Avoid for chronic use; serotonin syndrome risk with MAOIs
- Avoid in renal failure
Buprenorphine
- Partial μ agonist - ceiling effect on respiratory depression (major safety advantage)
- High receptor affinity → can displace full agonists; precipitates withdrawal if given when dependent patient still has opioids aboard
- Transdermal (chronic pain) and sublingual/buccal (OUD - Suboxone with naloxone)
Hydromorphone
- 5x more potent than morphine orally; 1.5 mg IV ≈ 30 mg oral morphine ≈ 7.5 mg oral hydromorphone
Naloxone
- Competitive μ (and κ, δ) antagonist
- Rapid reversal of opioid overdose (IV, IM, intranasal)
- Short duration: 30-90 minutes - may require repeat dosing or infusion for long-acting opioids
9. Pharmacokinetics & Routes of Administration
| Route | Notes |
|---|---|
| Oral | Preferred - most convenient; immediate and controlled-release |
| Transdermal | Bypasses GI; fentanyl, buprenorphine; useful when oral not feasible |
| IV | Rapid onset; most predictable absorption; used in acute/perioperative settings |
| IM | Avoid - painful, unreliable absorption |
| Intrathecal/epidural | Direct access to spinal opioid receptors; used perioperatively |
| Rectal | Alternative when oral unavailable |
Equianalgesic dosing is critical for opioid rotation. Example: 30 mg oral morphine ≈ 10 mg IV morphine ≈ 7.5 mg oral hydromorphone ≈ 1.5 mg IV hydromorphone.
10. Tolerance
Tolerance develops to most effects except constipation and miosis (no tolerance to these).
Mechanisms:
- Receptor desensitization - GRK (G protein-coupled receptor kinases) phosphorylate the receptor → β-arrestin recruitment → uncoupling from G proteins
- Receptor internalization/downregulation - reduced surface receptor density
- cAMP-CREB pathway upregulation - neurons adapt by increasing adenylyl cyclase and protein kinase A expression to counteract the chronic inhibition
- Central sensitization changes
Cross-tolerance among opioids is incomplete - opioid rotation can achieve 30-50% dose reduction at equianalgesic level.
11. Physical Dependence and Withdrawal
Mechanism - The cAMP Rebound Model
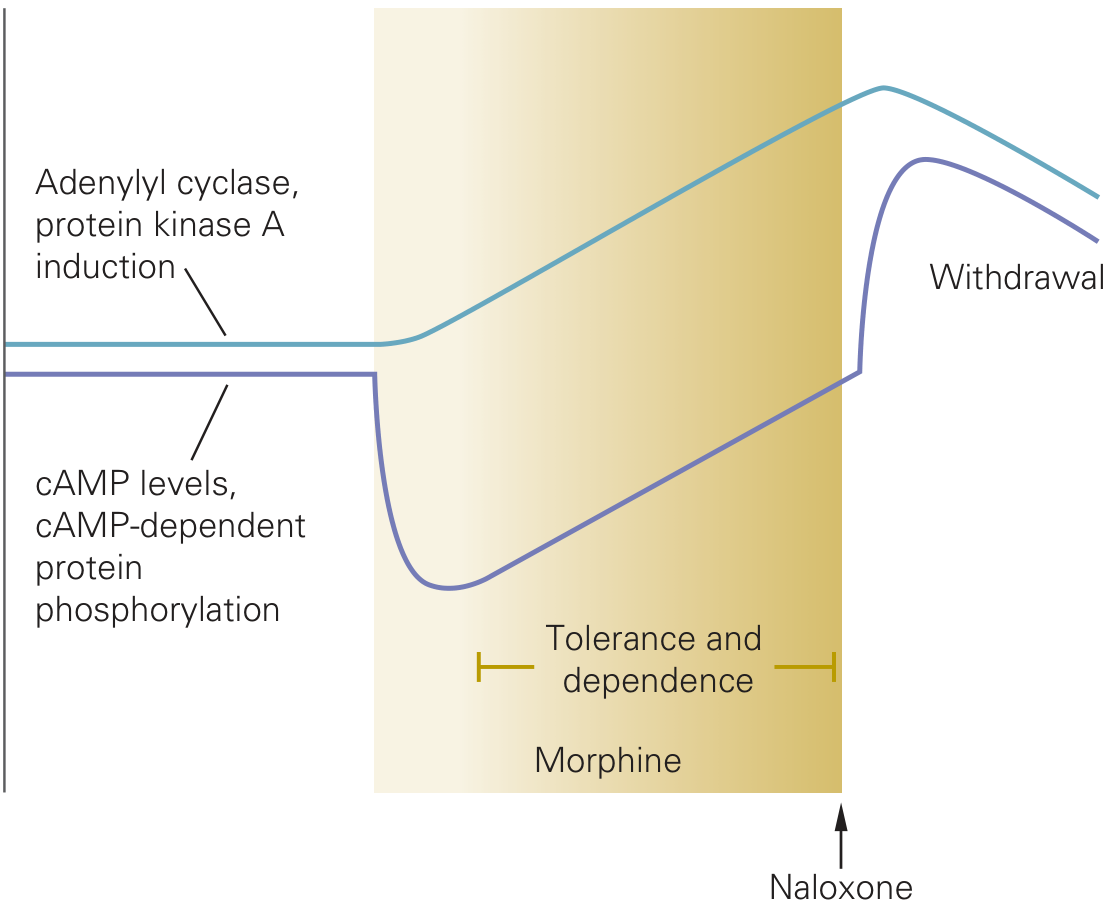
Figure: During chronic opioid exposure (shaded region), cAMP levels are suppressed. The neuron adapts by upregulating adenylyl cyclase and PKA (tolerance/dependence). When opioid is removed or naloxone is given, this upregulated pathway fires unopposed → withdrawal hyperactivity. (Adapted from Kandel's Principles of Neural Science)
During chronic use, neurons of the nucleus accumbens and locus coeruleus upregulate the cAMP-CREB pathway. On discontinuation, this pathway fires unopposed, causing noradrenergic storm - the cardinal feature of withdrawal. ΔFosB also accumulates in reward pathways and contributes to long-lasting neuroadaptation.
Opioid Withdrawal Syndrome (Abstinence Syndrome)
| Timing | Symptoms |
|---|---|
| Early (8-24h for short-acting) | Anxiety, yawning, lacrimation, rhinorrhea, sweating |
| Peak (36-72h) | Mydriasis, tachycardia, hypertension, piloerection, muscle cramps, diarrhea, nausea, vomiting, insomnia |
| Late | Fatigue, insomnia, restlessness (can persist weeks) |
Methadone withdrawal onset is delayed (3-4 days) and less intense due to its long half-life.
Note: Opioid withdrawal is rarely life-threatening in adults (unlike alcohol/benzodiazepine withdrawal) but is intensely dysphoric.
12. Opioid Tolerance vs. Opioid-Induced Hyperalgesia (OIH)
| Tolerance | OIH | |
|---|---|---|
| Definition | Reduced analgesic effect requiring dose increase | Paradoxical increased pain sensitivity from opioid use |
| Character | Original pain worsens | Diffuse, poorly localized pain; allodynia |
| Treatment | Dose increase or opioid rotation | Opioid taper/holiday; ketamine; α2 agonists |
| How to distinguish | Drug holiday - tolerance resolves, OIH may resolve differently |
NLRs/inflammasome signaling (NLRP3) contribute to OIH development (PMID: 38153538).
13. Opioid Use Disorder (OUD) - Neurobiology
OUD involves three features: (1) intoxication/euphoria, (2) pharmacogenic dependence/drug-seeking, (3) propensity to relapse. The mesolimbic dopamine system (VTA → nucleus accumbens) is central to reward and addiction. ΔFosB accumulation in nucleus accumbens neurons after repeated exposure contributes to long-lasting sensitization.
14. OUD Treatment (FDA-Approved)
| Drug | Class | Mechanism | Key Points |
|---|---|---|---|
| Methadone | Full μ agonist | Replaces opioid, reduces craving; cross-tolerance | Dispensed only in licensed clinics; monitor QTc |
| Buprenorphine (+/- naloxone) | Partial μ agonist | Ceiling on respiratory depression; long duration | Can be office-prescribed; precipitates withdrawal if given too early |
| Naltrexone | μ antagonist | Blocks opioid effects; no physical dependence | Requires detoxification first; monthly IM formulation (Vivitrol) available |
Methadone detox protocol: 10 mg orally when objective withdrawal signs appear; repeat q2-4h for 24h (max 40 mg); reduce by 5 mg/day. Buprenorphine requires objective withdrawal signs (COWS scale) before first dose.
- Goldman-Cecil Medicine, p. 273
15. Opioid Overdose - The Classic Triad
Miosis + Respiratory depression + Unconsciousness
Other features: cyanosis, bradycardia, hypotension, pulmonary edema (especially with heroin), hypothermia.
Treatment: Naloxone 0.4-2 mg IV/IM/IN; repeat every 2-3 minutes; may require infusion for long-acting opioids (methadone, extended-release formulations).
16. Special Pharmacology Considerations
Renal Failure
- Avoid: Morphine (M6G accumulates), codeine, meperidine
- Safe to use: Fentanyl, methadone, buprenorphine, hydromorphone (with caution)
Hepatic Failure
- Most opioids metabolized hepatically - reduce doses; monitor closely
- Morphine is relatively preferred
CYP2D6 Interactions
- Codeine, hydrocodone, oxycodone, tramadol are substrates
- CYP2D6 inhibitors (fluoxetine, paroxetine) block conversion → reduced analgesia with codeine
- CYP2D6 ultrarapid metabolizers → toxicity risk
Serotonin Syndrome Risk
- Tramadol + MAOIs, SSRIs, SNRIs → serotonin syndrome
- Fentanyl and meperidine also have some serotonergic activity
Summary Table - Key Receptor Effects
| Effect | μ | δ | κ |
|---|---|---|---|
| Analgesia | +++ | ++ | + |
| Respiratory depression | +++ | + | + |
| Euphoria | +++ | + | - |
| Dysphoria | - | - | +++ |
| Constipation | +++ | + | + |
| Miosis | ++ | - | ++ |
| Tolerance/Dependence | +++ | + | + |
| Sedation | ++ | - | +++ |
Sources:
- Goodman & Gilman's The Pharmacological Basis of Therapeutics - pp. 462-465 (Opioid Receptors, Signaling, Distribution)
- Bradley and Daroff's Neurology in Clinical Practice - pp. 1084, 1090 (Opioid Receptors, Analgesics)
- Goldman-Cecil Medicine International Edition - pp. 272-273 (Opioid Analgesics, OUD Treatment)
- Adams & Victor's Principles of Neurology, 12th Ed. - p. 1203 (Opioid Addiction)
- Katzung's Basic and Clinical Pharmacology, 16th Ed. - p. 353 (Tolerance, Dependence)
- Kandel's Principles of Neural Science, 6th Ed. - p. 1122 (cAMP-CREB mechanism of tolerance)
Sude effects and contraindications
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive, authoritative content from all the major pharmacology references. Let me compile the full detailed response:
Opioid Side Effects & Contraindications
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics | Katzung's Basic & Clinical Pharmacology, 16e | Harrison's Principles of Internal Medicine 22e | Bradley & Daroff's Neurology | Miller's Anesthesia, 10e
SIDE EFFECTS
Overview - What Develops Tolerance and What Doesn't
| Effect | Tolerance Develops? |
|---|---|
| Analgesia | Yes |
| Sedation | Yes |
| Nausea/vomiting | Yes (may persist months) |
| Respiratory depression | Yes (but danger persists at high dose) |
| Euphoria | Yes |
| Constipation | No - persists lifelong |
| Miosis | No |
| Seizure threshold lowering | No |
- Katzung's Basic & Clinical Pharmacology, 16e, p. 888
1. Respiratory System
Respiratory depression is the most dangerous side effect and the primary cause of death in overdose.
- Mechanism: μ2-receptor activation in the pre-Bötzinger complex of the medulla; reduced sensitivity to CO2 (blunted hypercapnic drive) and to hypoxia
- Manifestation: ↓ respiratory rate first (most sensitive indicator), then ↓ tidal volume; apnea at toxic doses
- Falls in O2 saturation represent a critical threshold - requires immediate intervention
- Potentiated by: benzodiazepines (particularly dangerous - avoid co-prescribing), other CNS depressants, alcohol, sleep (loss of cortical drive)
- Tolerance develops with chronic use, but respiratory arrest is still possible even in tolerant patients, especially with co-administered sedatives
- In patients with pain, the pain itself provides a stimulatory counter to sedation - if pain is suddenly relieved (e.g., nerve block), respiratory depression may become unmasked
Histamine release (morphine, codeine):
- Can cause bronchospasm - particularly dangerous in asthmatics
- Fentanyl has minimal histamine release - preferred in patients with asthma/COPD
- Goodman & Gilman, p. 475; Harrison's 22e, p. 988
2. Gastrointestinal System
Constipation
- Most common and clinically significant chronic side effect
- No tolerance develops - persists indefinitely with continued use
- Mechanism: μ receptors in the enteric nervous system → ↓ propulsive motility, ↑ segmental non-propulsive contractions, ↓ GI secretions, ↑ sphincter tone
- Management: Always prescribe stimulant laxatives prophylactically (bisacodyl, senna, polyethylene glycol); fiber alone is insufficient
- Severe refractory cases: Methylnaltrexone (peripherally acting μ antagonist - does not cross BBB, so doesn't reverse analgesia), naloxegol, lubiprostone
Nausea and Vomiting
- Mechanism: Stimulation of the chemoreceptor trigger zone (CTZ) in the area postrema (μ and δ receptors); also vestibular stimulation (exacerbated by movement - ambulatory patients > recumbent)
- Usually occurs early in treatment; tolerance develops with continued use (though may persist months)
- Management: Metoclopramide, haloperidol, ondansetron, scopolamine, hydroxyzine; switching opioids
Delayed Gastric Emptying
- Opioids slow gastric emptying → contributes to nausea, increases risk of aspiration in perioperative settings
Biliary Spasm
- Opioids increase tone of sphincter of Oddi → can worsen biliary colic or cause elevated LFTs/amylase
- Meperidine historically claimed to cause less biliary spasm (not well supported by evidence)
3. Central Nervous System
| Effect | Notes |
|---|---|
| Sedation | Early in treatment; tolerance develops; treat with CNS stimulants if persists (methylphenidate, modafinil) |
| Euphoria | Via mesolimbic dopamine disinhibition (VTA → nucleus accumbens); drives addictive potential |
| Dysphoria | Especially with κ-agonists (pentazocine, butorphanol); also with high doses |
| Miosis | Edinger-Westphal nucleus; no tolerance develops - diagnostic sign of opioid toxicity; pinpoint pupils in overdose |
| Hallucinations/Delirium | More common with morphine (M3G metabolite), meperidine (normeperidine), hydromorphone; switch opioids |
| Myoclonus | Especially high-dose morphine or hydromorphone; accumulation of metabolites |
| Seizures | Normeperidine (meperidine metabolite) - NOT reversed by naloxone; tramadol; high-dose meperidine |
| Sleep disturbances | Suppress REM sleep; impair sleep architecture |
| Cognitive impairment | Driving impairment; chronic users have measurable cognitive deficits |
| Cough suppression | Useful therapeutically (codeine, dextromethorphan) |
- Bradley & Daroff's Neurology, p. 1090; Harrison's 22e, p. 990
4. Cardiovascular System
- Peripheral vasodilation - due to histamine release and reduced sympathetic outflow → hypotension
- Bradycardia - at high doses; vagal effects
- Methadone specifically: QTc prolongation via hERG K+ channel blockade → risk of Torsades de Pointes; requires baseline and follow-up ECG monitoring
- Reduced preload may be beneficial in acute pulmonary edema (morphine used adjunctively, though recent evidence challenges this)
5. Genitourinary System
- Urinary retention - ↑ bladder sphincter tone, ↓ detrusor tone; more common with neuraxial (intrathecal/epidural) administration and in elderly males with BPH
- Antidiuretic effect - via ↑ ADH secretion; tolerance develops
- More common with IV, transmucosal, and epidural routes vs. oral
6. Integument / Allergic
Pruritus
- Very common with neuraxial (intrathecal/epidural) opioids - incidence 30-100% with intrathecal dosing
- Mechanism: Central μ-receptor activation in the spinal cord/brain - NOT primarily histamine-mediated. This is why antihistamines are often ineffective.
- Treatment:
- Naloxone or naltrexone (low-dose, antagonist reversal)
- Nalbuphine (partial agonist - shifts receptor occupancy)
- Ondansetron (5-HT3 antagonism)
- Propofol (low dose)
- Mirtazapine (5-HT3 antagonism + sedation)
- NSAIDs (diclofenac, tenoxicam) may help
- Morphine, codeine cause more pruritus via histamine release at injection site (urticaria, wheals)
True Allergy
- Rare - urticaria, fixed drug eruptions, anaphylactoid reactions
- Wheals at injection site = local histamine release (not true allergy)
- True anaphylaxis is uncommon but reported with IV codeine/morphine
- Miller's Anesthesia, 10e, p. 6125
7. Endocrine and Metabolic (Chronic Use)
| Effect | Mechanism | Clinical Consequence |
|---|---|---|
| Hypogonadism | ↓ GnRH → ↓ LH, FSH → ↓ testosterone/estrogen | Sexual dysfunction, infertility, fatigue, mood changes |
| Osteoporosis | Hypogonadism + direct effects | Accelerated bone loss, fracture risk |
| Hyperprolactinemia | ↑ prolactin release | Galactorrhea, gynecomastia |
| ↑ ADH | Direct hypothalamic effect | Hyponatremia (SIADH-like) |
| Immunosuppression | ↓ NK cell activity, altered cytokine profile | Increased infection susceptibility |
| ↑ Growth hormone | Via hypothalamic effects | Metabolic effects |
| ↑ Feeding/weight gain | CNS effects on appetite | Obesity risk in chronic users |
Addison's disease / hypothyroidism: These patients have prolonged and exaggerated responses to opioids - use with extreme caution and at reduced doses.
- Katzung's Basic & Clinical Pharmacology, 16e, p. 888
8. Neonatal/Obstetric Effects
- Opioids cross the placenta → neonatal respiratory depression; have naloxone available at delivery
- Neonatal Opioid Withdrawal Syndrome (NOWS) in infants born to opioid-dependent mothers
- Breastfeeding: No absolute contraindication as a class; however codeine is contraindicated in breastfeeding mothers as CYP2D6 ultrarapid metabolizers can generate toxic morphine levels in breast milk
9. Drug-Specific Toxicities Summary
| Drug | Specific Toxicity |
|---|---|
| Meperidine | Normeperidine accumulation → myoclonus, seizures (NOT reversed by naloxone); serotonin syndrome with MAOIs/SSRIs; avoid in renal failure, elderly, chronic use |
| Tramadol | Lowers seizure threshold; serotonin syndrome with MAOIs/SSRIs/TCAs; avoid in seizure disorder; weak analgesia ceiling |
| Morphine | M6G accumulates in renal failure → prolonged CNS/respiratory depression; M3G may cause hyperalgesia/neuroexcitability |
| Methadone | QTc prolongation; highly variable PK (t½ 4-130h) - accumulation risk; drug-drug interactions via CYP3A4/2D6/2C19 |
| Codeine | CYP2D6 ultrarapid metabolizers → acute morphine toxicity; CYP2D6 poor metabolizers get no analgesia; contraindicated in breastfeeding |
| Fentanyl | "Wooden chest syndrome" at high IV bolus doses - rigidity of chest wall muscles (treat with neuromuscular blocker or naloxone); illicit analogues (carfentanil) highly lethal |
| Buprenorphine | Can precipitate withdrawal if given while other opioids still occupying receptors; ceiling on analgesia |
| Pentazocine | Psychotomimetic effects (hallucinations, dysphoria) from κ agonism; can precipitate withdrawal in dependent patients |
CONTRAINDICATIONS
Absolute Contraindications
| Condition | Reason |
|---|---|
| Acute respiratory depression/apnea (without intubation) | Will worsen life-threateningly |
| Paralytic ileus | Opioids further suppress GI motility; may worsen |
| Concurrent MAOI use | Risk of hyperpyrexic coma, serotonin syndrome, hypertensive crisis - especially meperidine and tramadol. Relative for other opioids. |
| Naloxone given to opioid-dependent neonate | Precipitates life-threatening opioid withdrawal seizures |
| Known hypersensitivity (true allergy) to specific opioid | Switch to a structurally unrelated opioid |
- Goodman & Gilman, p. 475; Katzung, p. 891
Relative Contraindications / Strong Cautions
| Condition | Risk / Recommendation |
|---|---|
| Acute severe asthma / COPD | Morphine/codeine cause histamine release → bronchospasm; risk of respiratory failure. Use fentanyl if opioid required. |
| Head injury / raised intracranial pressure | Opioids cause CO2 retention → cerebral vasodilation → ↑ ICP; miosis/vomiting obscure neurological assessment. Use cautiously with ventilatory monitoring. |
| Renal failure | Morphine (M6G accumulation), codeine, meperidine, hydromorphone (with caution). Use fentanyl or methadone. |
| Hepatic failure | Most opioids hepatically metabolized - reduced clearance; use lower doses with close monitoring |
| Hypovolemia / hemodynamic instability | Vasodilation from morphine → precipitous hypotension |
| Hypotension from any cause | As above |
| Hypothyroidism / Addison's disease | Exaggerated and prolonged opioid effects - use reduced doses |
| Elderly patients | Reduced renal/hepatic clearance; increased CNS sensitivity; start low, go slow |
| Obstructive sleep apnea (OSA) | Already have impaired respiratory drive; opioids can cause dangerous apneic episodes, especially at night |
| Morbid obesity | Reduced functional residual capacity; impaired respiratory reserve |
| Cor pulmonale / kyphoscoliosis | Operating at respiratory compensation limit; CO2-dependent drive |
| Seizure disorder | Meperidine, tramadol lower seizure threshold |
| Biliary colic | Sphincter of Oddi spasm may worsen pain |
| Bowel obstruction | Worsens ileus |
| BPH / urinary retention | Risk of acute urinary retention - requires catheterization |
| Concurrent benzodiazepines | Synergistic respiratory depression - particularly dangerous in outpatient setting; avoid combination |
| Pregnancy | Neonatal respiratory depression at delivery; neonatal withdrawal syndrome; use cautiously and with informed consent |
| Active substance use disorder | Risk of misuse/diversion; structured monitoring required; consider abuse-deterrent formulations |
| Severe mental illness | Impaired adherence, risk of misuse; careful risk-benefit evaluation |
DRUG INTERACTIONS - Key Table
| Interacting Drug/Class | Effect with Opioids | Clinical Significance |
|---|---|---|
| Benzodiazepines | Synergistic CNS and respiratory depression | HIGH - major cause of overdose death; avoid combination if possible |
| Alcohol | Synergistic CNS depression | HIGH - common in unintentional overdose |
| Other CNS depressants (barbiturates, non-BZD hypnotics, antipsychotics, gabapentinoids) | Enhanced sedation, respiratory depression | HIGH |
| MAOIs (phenelzine, tranylcypromine, selegiline) | Hyperpyrexic coma, serotonin syndrome, hypertension | Relative/absolute contraindication - meperidine and tramadol are worst |
| SSRIs/SNRIs + Tramadol | Serotonin syndrome | Avoid combination |
| CYP3A4 inhibitors (ketoconazole, erythromycin, HIV PIs) | ↓ metabolism of fentanyl, methadone, oxycodone → opioid toxicity | Monitor carefully |
| CYP3A4 inducers (rifampicin, carbamazepine, phenytoin) | ↑ metabolism → reduced opioid efficacy or withdrawal | May need dose adjustment |
| CYP2D6 inhibitors (fluoxetine, paroxetine, bupropion) | Block conversion of codeine/tramadol to active form → reduced efficacy (or accumulate inactive parent drug) | Clinical failure with codeine in pain |
| Antipsychotics | ↑ sedation; accentuate antimuscarinic and α-blocking cardiovascular effects | Use caution |
| Anticholinergics | Additive ↑ urinary retention, constipation, dry mouth | Common in elderly polypharmacy |
| Partial agonists/mixed agonist-antagonists given to opioid-dependent patients | Precipitates acute withdrawal | Critical clinical point |
- Katzung's Basic & Clinical Pharmacology, 16e, p. 891
Management of Side Effects - Quick Reference
| Side Effect | First-Line Management |
|---|---|
| Constipation | Stimulant laxatives prophylactically (senna, bisacodyl); methylnaltrexone for refractory cases |
| Nausea | Metoclopramide, ondansetron, haloperidol; switch opioid; reduce dose |
| Sedation | Reduce dose; opioid rotation; methylphenidate or modafinil if required |
| Pruritus | Low-dose naloxone/nalbuphine; ondansetron; mirtazapine; not primarily antihistamines |
| Respiratory depression | Naloxone (titratable doses 0.04-0.1 mg IV q2-3 min) - use incremental dosing to preserve some analgesia |
| Urinary retention | Catheterization; reduce dose; try α-blocker; opioid rotation |
| Delirium/hallucinations | Opioid rotation; haloperidol; reduce dose; check for metabolite accumulation (morphine → meperidine) |
| Myoclonus/seizures (normeperidine) | Stop meperidine; benzodiazepines for seizures (naloxone will NOT help) |
| Opioid-induced hyperalgesia | Opioid taper; opioid rotation; ketamine; consider NMDA antagonists |
| Hypogonadism | Testosterone/hormone replacement; consider opioid rotation to buprenorphine (less endocrine disruption) |
| QTc prolongation (methadone) | ECG monitoring; avoid other QT-prolonging drugs; reduce dose or switch |
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics - pp. 475-476 (Contraindications by condition)
- Katzung's Basic & Clinical Pharmacology, 16e - pp. 888-891 (Adverse effects table, drug interactions)
- Harrison's Principles of Internal Medicine, 22e - pp. 988-990 (Side effects overview)
- Bradley & Daroff's Neurology in Clinical Practice - pp. 1090-1091 (CNS side effects, management)
- Miller's Anesthesia, 10e - p. 6125 (Pruritus mechanism and treatment)
Distribution of opiodis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive, detailed content from the key pharmacology and anesthesia references. Let me compile the complete answer:
Distribution of Opioids - Detailed Pharmacokinetics
Sources: Barash's Clinical Anesthesia, 9e | Goodman & Gilman's Pharmacological Basis of Therapeutics | Miller's Anesthesia, 10e
The word "distribution" in opioid pharmacology covers two distinct but interrelated concepts:
- Pharmacokinetic distribution - how the drug distributes from plasma into tissues (governed by physicochemical properties)
- Receptor distribution - where opioid receptors are located anatomically, which determines the drug's range of effects
PART 1 - PHARMACOKINETIC DISTRIBUTION
Determinants of Distribution
After IV injection, opioids are first transported to the heart and pulmonary circulation, then disperse to organs and tissues. The key physicochemical properties governing distribution are:
| Property | Significance |
|---|---|
| Lipid solubility | Primary driver of CNS penetration rate and tissue distribution |
| Plasma protein binding (albumin + α1-acid glycoprotein) | High binding → reduced free fraction → less available to cross BBB |
| pKa / ionization state | Only non-ionized form crosses membranes; pH-dependent |
| Molecular size | Affects BBB penetration |
A small increase in pH (e.g., respiratory alkalosis) increases the non-ionized fraction of morphine, fentanyl, sufentanil, and remifentanil - enhancing CNS entry. Active transport systems in the BBB also efflux opioids from the brain (e.g., cyclosporine blocks morphine's efflux transporter, enhancing its effect).
- Barash's Clinical Anesthesia, 9e, p. 1540
Multi-Compartment Distribution Model
After IV bolus, plasma concentration follows a characteristic multi-phase curve:
Phase 1 - α (rapid distribution):
Drug leaves plasma → high-flow organs (brain, liver, kidney, heart)
→ rapid initial fall in plasma concentration
→ rapid onset of CNS effect
Phase 2 - β (slower redistribution):
Drug leaves high-flow organs → lower-flow tissues (muscle)
→ slower fall in plasma concentration
→ termination of CNS effect for most bolus doses
Phase 3 - γ (terminal elimination):
Drug leaves fat/peripheral tissues back to plasma → liver metabolism
→ slow terminal half-life, clinically relevant with prolonged infusions
This is why a single bolus of fentanyl has a short clinical duration despite a long terminal half-life - the drug redistributes OUT of the brain into muscle, even before significant metabolism occurs.
Volume of Distribution (Vd)
| Opioid | Vd (approx.) | Reason |
|---|---|---|
| Fentanyl | ~300 L | Highly lipophilic + moderate protein binding → large peripheral reservoir |
| Sufentanil | ~123 L | Very high lipophilicity but very high protein binding (~92%) offsets |
| Morphine | ~230-400 L | Despite being relatively hydrophilic, extensively distributes to tissues |
| Alfentanil | ~27 L | High protein binding (~90%) limits tissue distribution |
| Remifentanil | ~28 L | Very high clearance + low tissue affinity → small Vd |
| Methadone | ~300-600 L | Highly lipophilic; vast peripheral distribution accounts for variable half-life |
Clinical implication: High Vd drugs (fentanyl, methadone) accumulate in fat/muscle with prolonged use → prolonged clinical effect after stopping infusion.
- Barash's Clinical Anesthesia, 9e, p. 1541
Lipophilicity Comparison - The Clinical Ranking
From most to least lipophilic:
Sufentanil > Fentanyl > Alfentanil > Methadone > Buprenorphine > Heroin > Meperidine > Morphine (most hydrophilic)
| Property | Morphine (Hydrophilic) | Fentanyl (Lipophilic) |
|---|---|---|
| BBB penetration speed | Slow | Fast |
| Onset of CNS effect (IV) | 15-30 min | 1-5 min |
| Duration (single bolus) | Longer (slow redistribution) | Short (fast redistribution) |
| Spinal cord penetration (intrathecal/epidural) | Spreads widely (rostral spread risk) | Stays local |
| Accumulation with infusion | Less | More (large peripheral reservoir) |
| Neonatal CNS penetration | Less | More |
Morphine is hydrophilic - this means proportionately less morphine crosses the blood-brain barrier under normal conditions. However, when the BBB is compromised (e.g., meningitis, trauma) or in neonates (immature BBB), more enters the CNS. Lipophilic opioids (fentanyl) may give more predictable results in neonates.
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Plasma Protein Binding
| Opioid | Protein Binding (%) | Bound To |
|---|---|---|
| Sufentanil | ~92% | α1-acid glycoprotein (AGP) |
| Alfentanil | ~90% | AGP |
| Fentanyl | ~84% | AGP + albumin |
| Methadone | ~85-90% | AGP |
| Buprenorphine | ~96% | AGP + albumin |
| Morphine | ~35% | Albumin |
| Remifentanil | ~70% | AGP |
| Codeine | ~7-25% | Albumin |
AGP (α1-acid glycoprotein) is an acute-phase reactant - levels rise in trauma, surgery, cancer, inflammation → higher protein binding → reduced free fraction → reduced CNS effect at a given dose. This is clinically relevant in ICU patients who may show variable opioid responses.
Context-Sensitive Half-Time (CSt½)
This concept is critical for infusion management - it describes the time for plasma concentration to fall 50% after stopping an infusion, and it depends on the duration of the infusion (the "context").
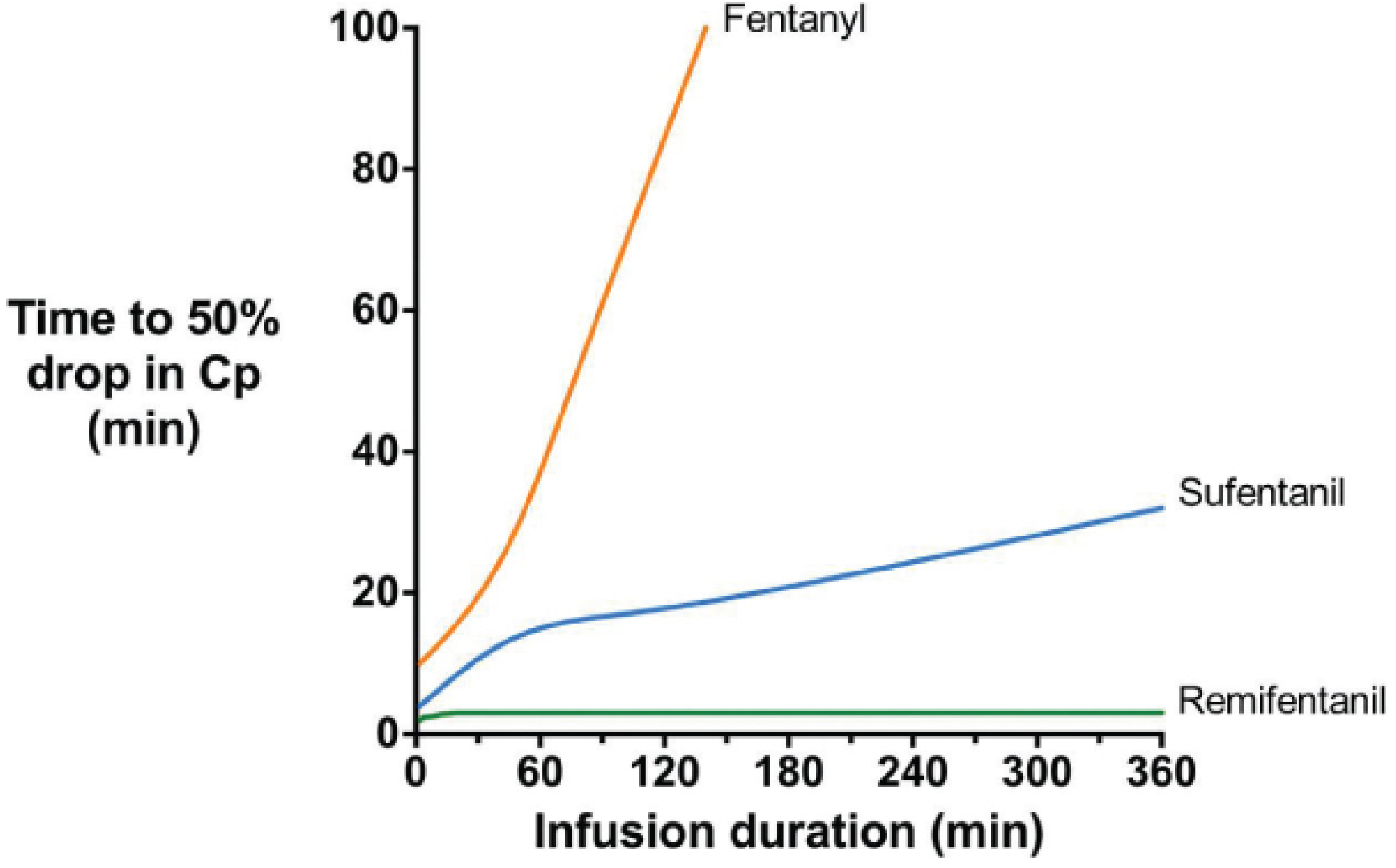
Figure: Time to 50% drop in plasma concentration (Cp) after infusions of varying duration. Remifentanil is constant at ~2 minutes regardless of infusion length. Fentanyl's CSt½ rises steeply - after a 2-hour infusion, it may take >100 minutes to fall 50%. Sufentanil is intermediate. (Barash's Clinical Anesthesia, 9e, p. 1541)
| Opioid | CSt½ Behavior |
|---|---|
| Remifentanil | ~2 min, regardless of infusion duration (ester hydrolysis in plasma/tissues) |
| Alfentanil | Short, relatively stable with increasing duration |
| Sufentanil | Moderate, increases slowly with duration |
| Fentanyl | Rises steeply with infusion duration → unpredictable long offset after prolonged infusions |
| Morphine | Intermediate |
| Methadone | Very long, highly variable (t½ 4-130 hours) |
Why fentanyl and sufentanil differ: Both are highly lipophilic, but sufentanil's very high protein binding limits its free peripheral distribution, creating a smaller peripheral reservoir. Fentanyl has lower protein binding → vast adipose redistribution → large depot that releases back into plasma after infusion ends.
Special Compartments of Distribution
Blood-Brain Barrier (BBB)
- Lipophilic opioids (fentanyl, sufentanil, heroin) cross rapidly → fast onset
- Morphine crosses slowly → delayed onset; peak CNS effect 15-30 min after IV dose
- Compromised BBB → all opioids enter more readily
- Active efflux transporters (P-glycoprotein) pump some opioids OUT of brain → clinically significant with drug interactions
Spinal Cord (Neuraxial Route)
This is a particularly important distribution concept:
| Characteristic | Hydrophilic (Morphine) | Lipophilic (Fentanyl) |
|---|---|---|
| Onset after intrathecal | Slow (30-60 min) | Fast (5-10 min) |
| Duration (intrathecal) | Long (12-24h) | Short (2-4h) |
| Spread in CSF | Wide - rostral spread | Stays near injection site |
| Risk of delayed respiratory depression | High (spreads to brainstem) | Low |
| Risk of pruritus | High | High (both) |
This is why intrathecal morphine is used for postoperative analgesia after major surgery - one dose provides 12-24 hours of analgesia. But it carries a risk of late (6-18h) respiratory depression as drug migrates rostrally to brainstem μ2 receptors.
Fat/Adipose Tissue
- Lipophilic opioids (fentanyl, sufentanil, methadone) accumulate extensively in fat
- In obese patients → larger peripheral reservoir → prolonged duration of action
- In elderly patients → relatively increased fat mass → greater redistribution
Placenta and Breast Milk
- All opioids cross the placenta (lipophilic ones cross faster)
- Appear in breast milk (morphine, codeine at clinically relevant levels)
- Fentanyl in breast milk is generally considered low-risk due to poor oral bioavailability in neonate
- Codeine in breast milk is contraindicated (CYP2D6 ultrarapid metabolizers)
Interpatient Variability in Distribution
Barash notes at least 30-fold variability in plasma concentrations between patients after a standard dose, driven by:
| Factor | Effect |
|---|---|
| Lean body mass / fat mass | Affects Vd - obese patients have larger peripheral reservoir |
| Cardiac output | High CO → faster distribution to CNS; low CO (shock) → more drug stays in central compartment → toxicity risk |
| Hepatic function | Affects first-pass and metabolic clearance |
| Renal function | Affects active metabolite clearance (morphine-6-glucuronide) |
| Age | Elderly: reduced Vd, lower plasma proteins, reduced clearance → higher plasma levels per dose |
| Plasma protein levels | Low albumin/AGP (cirrhosis, nephrotic syndrome) → ↑ free drug fraction → enhanced effect |
PART 2 - ANATOMICAL RECEPTOR DISTRIBUTION
This is the distribution that explains what opioids do where - the pattern of μ, κ, δ, and NOP receptor expression across the nervous system.
Overview
Opioid receptors are distributed both pre- and postsynaptically throughout the peripheral and central nervous system, as well as on non-neuronal cells.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 463
Mu (μ) Receptor Distribution
The mu receptor mediates all clinically important analgesic effects of therapeutic opioids. Its distribution explains every major opioid effect:
| Region | Effect Mediated |
|---|---|
| Periaqueductal gray (PAG) | Supraspinal analgesia (descending pain inhibition) |
| Rostral ventromedial medulla (RVM) | Descending inhibitory modulation to dorsal horn |
| Dorsal horn of spinal cord (superficial layers I, II) | Spinal analgesia - pre + postsynaptic inhibition of nociceptive input |
| Neocortex (superficial + deeper layers) | Affective component of pain; cognitive effects |
| Thalamus | Sensory relay; analgesic and sedative effects |
| Nucleus accumbens | Euphoria, reward, addiction (mesolimbic dopamine disinhibition) |
| Ventral tegmental area (VTA) | Reward pathway - disinhibition of dopamine neurons |
| Hippocampus | Memory effects, cognitive impairment |
| Amygdala | Emotional component of pain; anxiolytic effects |
| Raphe nucleus | Modulation of descending serotonergic pathways |
| Medulla / pons (pre-Bötzinger complex) | Respiratory depression |
| Edinger-Westphal nucleus (oculomotor) | Miosis |
| Chemoreceptor trigger zone (area postrema) | Nausea/vomiting |
| Peripheral sensory nerve terminals | Peripheral analgesia (enhanced under inflammation) |
| Enteric nervous system (GI tract) | Constipation, ↓ secretion, sphincter spasm |
| Bladder / urinary sphincter | Urinary retention |
Two subtypes:
- μ1 (supraspinal, neocortex, thalamus) → analgesia, euphoria
- μ2 (spinal cord, brainstem) → respiratory depression, constipation
Kappa (κ) Receptor Distribution
Concentrated in:
- Caudate-putamen, nucleus accumbens
- Amygdala - stress responses
- Hypothalamus, pituitary - neuroendocrine effects (diuresis, feeding, stress axis)
- PAG, raphe nuclei, pons, medulla
- Dorsal horn (sparse)
- Minimal in cortex
Functions: Visceral and neuropathic analgesia, dysphoria (not euphoria), diuresis, reduced food intake, stress responses. Peripherally restricted κ agonists are under development to treat visceral pain without CNS side effects.
Delta (δ) Receptor Distribution
Concentrated in:
- Olfactory areas - unique distribution among opioid receptors
- Neocortex
- Caudate-putamen, nucleus accumbens, amygdala
- Low levels in dorsal horn
Functions: Modulation of pain (especially inflammatory and bone pain) and mood. Cardioprotective effects in the heart. Promising target for pain + depression co-treatment.
NOP/ORL1 Receptor Distribution
- Most widely distributed of all four receptor types
- Found in most brain regions and spinal cord
- Areas related to pain, reward, anxiety/stress, memory, and feeding
Special feature: Naloxone-insensitive - NOP agonists can actually oppose μ-receptor analgesia at supraspinal sites (anti-opioid effect) while providing analgesia at spinal/peripheral sites.
Non-Neuronal Distribution
| Cell Type | Receptor | Functional Significance |
|---|---|---|
| Macrophages / microglia | μ, κ, δ | Immunomodulation; opioid-induced immunosuppression |
| Astrocytes | μ, κ, δ | Neuroinflammation; tolerance mechanisms |
| Enteric neurons | μ, κ, δ | GI motility, secretion - basis for PAMORAs (peripherally acting mu-opioid receptor antagonists) |
| Peripheral sensory terminals | μ, κ, δ | Peripheral analgesia, especially in inflamed tissue (upregulated in inflammation) |
| Cardiac myocytes | δ | Cardioprotection via ischemic preconditioning |
| Immune cells (T/B lymphocytes) | μ | Immunosuppression with chronic opioid use |
Summary - Integration of Both Concepts
Physicochemical Property → PK Distribution → Receptor Location → Clinical Effect
Lipophilic (fentanyl):
Fast BBB crossing → rapid CNS receptor binding → fast onset
Large Vd (fat depot) → redistribution terminates effect → short bolus duration
Stays at neuraxial injection site → segmental spinal analgesia
Hydrophilic (morphine):
Slow BBB crossing → delayed peak CNS effect
Wide CSF spread → rostral migration → risk of late respiratory depression
Peripheral conversion → active M6G metabolite (renal accumulation risk)
Both reach μ receptors in PAG, dorsal horn (analgesia),
medulla (respiratory depression), enteric NS (constipation)
Sources:
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - pp. 1540-1543 (Opioid Pharmacokinetics, Volume of Distribution, Context-Sensitive Half-Times)
- Goodman & Gilman's Pharmacological Basis of Therapeutics - p. 463 (Opioid Receptor Distribution: μ, κ, δ, NOP)
- Miller's Anesthesia, 10e - p. 6125 (Neuraxial opioid distribution effects)
This is a shared conversation. Sign in to Orris to start your own chat.