Perioperative management of cardiac patient posted for non cardiac surgery in MD Anaesthesia with viva questions
Reading File
Finding Sources
Finding Sources
Searching the Web
perioperative management cardiac patient non cardiac surgery MD anaesthesia viva questions 2024
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from Barash, Fuster & Hurst, and Morgan & Mikhail, plus both key flowcharts. Let me now write the complete MD Anaesthesia-level answer.
Perioperative Management of Cardiac Patient Posted for Non-Cardiac Surgery
MD Anaesthesia - Comprehensive Notes + Viva Questions
PART 1: OVERVIEW AND FRAMEWORK
The perioperative evaluation of a cardiac patient for non-cardiac surgery is NOT about "cardiac clearance" - it is a structured risk-benefit analysis involving three key questions:
- What is the surgical risk?
- What is the patient's cardiac risk?
- What is the patient's functional capacity?
The 2024 ACC/AHA guidelines (updated from 2014) provide the current framework, reinforced by the 2022 ESC/ESA guidelines.
PART 2: SURGICAL RISK CLASSIFICATION
(Barash Clinical Anesthesia 9e, Fuster & Hurst 15e)
| Surgical Risk Category | 30-day MACE | Examples |
|---|---|---|
| Low | <1% | Cataract, breast, endoscopy, superficial procedures |
| Intermediate | 1-5% | Intraperitoneal, intrathoracic, orthopedic (hip/knee), prostate, head & neck |
| High | >5% | Aortic/major vascular surgery, peripheral vascular, emergency surgery |
Classification of surgical urgency (ACC/AHA):
| Class | Definition |
|---|---|
| Emergent | Life/limb threatened; surgery within <6 hours |
| Urgent | Limited evaluation possible; surgery within 6-24 hours |
| Time-sensitive | Delay >1-6 weeks significantly affects outcome (e.g., oncologic) |
| Elective | Can be delayed up to 1 year |
In emergent surgery, proceed immediately with risk mitigation strategies - no time for formal evaluation.
PART 3: ACTIVE CARDIAC CONDITIONS (ABSOLUTE CONTRAINDICATIONS FOR ELECTIVE SURGERY)
These must be evaluated and treated before elective surgery:
- Unstable coronary syndromes - Unstable angina, recent MI (within 60 days)
- Decompensated heart failure (NYHA Class IV, new onset, worsening HF)
- Significant arrhythmias
- High-degree AV block (Mobitz II, complete heart block)
- Symptomatic bradycardia / sick sinus syndrome
- Sustained ventricular tachycardia
- Supraventricular tachycardia with uncontrolled ventricular rate (>100 bpm)
- Severe valvular disease
- Severe aortic stenosis (mean gradient >40 mmHg, AVA <1.0 cm²)
- Symptomatic mitral stenosis
PART 4: PREOPERATIVE RISK STRATIFICATION TOOLS
A. Revised Cardiac Risk Index (RCRI / Lee Index)
(Published by Lee et al., 1999 - most widely used)
6 independent predictors (1 point each):
- High-risk type of surgery (intrathoracic, intraperitoneal, suprainguinal vascular)
- History of ischemic heart disease (MI, positive stress test, current chest pain, NTG use, Q waves on ECG)
- History of congestive heart failure
- History of cerebrovascular disease (TIA or stroke)
- Insulin-dependent diabetes mellitus
- Chronic kidney disease (serum creatinine >2.0 mg/dL)
Risk stratification:
| RCRI Score | Risk of Major Cardiac Complications |
|---|---|
| 0 | 0.4% |
| 1 | 0.9% |
| 2 | 6.6% |
| ≥3 | 11% |
B. Goldman Cardiac Risk Index (Original, 1977)
Predecessor to RCRI; 9 variables with weighted scoring; maximum 53 points; Class IV (≥26 points) = highest risk.
C. ACS NSQIP / NSQIP-MICA
Uses 21 patient-specific variables and CPT codes; better discrimination than RCRI but more complex.
D. Gupta Myocardial Infarction and Cardiac Arrest (MICA) Calculator
Developed from 211,410 patients in the ACS NSQIP database; 5 predictors: type of surgery, functional dependence, ASA class, creatinine, age.
PART 5: ASSESSMENT OF FUNCTIONAL CAPACITY
Expressed in METs (Metabolic Equivalents):
| METs | Activity | Clinical Implication |
|---|---|---|
| 1 MET | Self-care, eating, walking on flat at 2-3 mph | Poor |
| 4 METs | Climbing a flight of stairs, walking at 4 mph | Adequate threshold |
| >4 METs | Golf, dancing, doubles tennis | Good |
| >10 METs | Strenuous sports (swimming, squash) | Excellent |
Clinical significance: Patients who cannot achieve ≥4 METs without symptoms may require further testing before intermediate/high-risk surgery.
The 2018 METS study (Lancet) showed self-reported functional capacity was a poor predictor of perioperative events - objective testing (CPET - cardiopulmonary exercise testing) is preferred when feasible.
PART 6: PREOPERATIVE CARDIAC INVESTIGATIONS
Standard workup:
- 12-lead ECG - Mandatory for patients with known cardiac disease, arrhythmia, or intermediate/high-risk surgery
- Echocardiography - For suspected ventricular dysfunction, valvular disease, or new symptoms
- Chest X-ray
- BNP/NT-proBNP - Now incorporated in 2024 guidelines; elevated levels (BNP >92 pg/mL or NT-proBNP >300 pg/mL) are associated with increased MACE
Functional/Stress Testing - Indications:
Only indicated if:
- Patient has elevated surgical risk (≥1%) AND
- Has poor or unknown functional capacity AND
- Results would change perioperative management
Options:
- Exercise ECG (treadmill)
- Dobutamine stress echocardiography (DSE) - for patients who cannot exercise
- Myocardial perfusion imaging (thallium/sestamibi scan)
- Coronary CTA
The fundamental rule: No testing should be done if results won't change management (Barash 9e).
Coronary revascularization before NCS:
Prophylactic revascularization (PCI/CABG) is NOT recommended solely to reduce perioperative cardiac risk. Revascularization should only be considered if it would be indicated regardless of the planned surgery (e.g., left main disease, triple vessel disease with LV dysfunction).
PART 7: PERIOPERATIVE MEDICATION MANAGEMENT
(Fuster & Hurst 15e, Barash 9e - 2024 ACC/AHA framework)
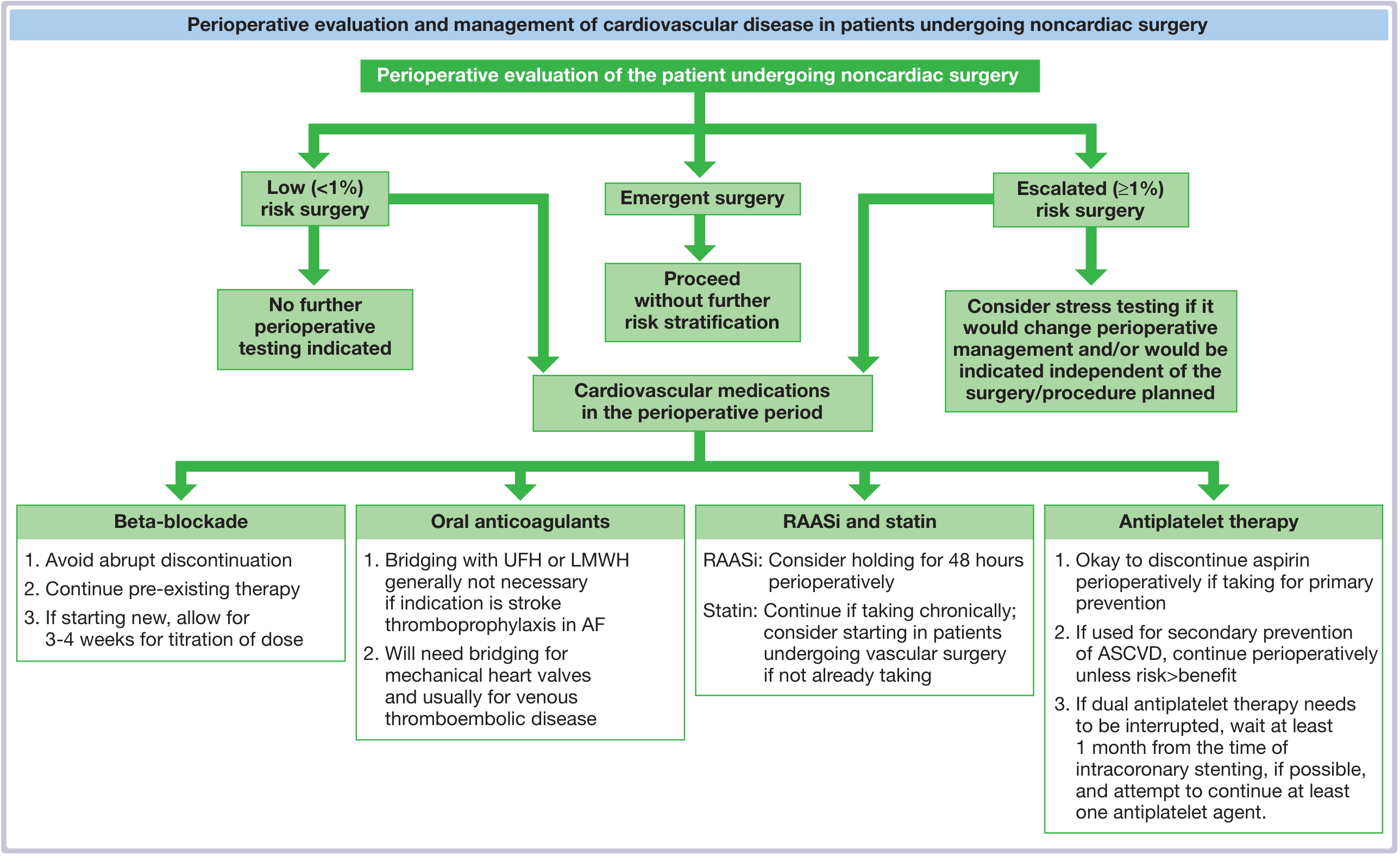
1. Beta-Blockers (Most Examined Topic)
POISE Trial (2008) - Landmark RCT of perioperative metoprolol:
- High-dose metoprolol started 2-4 hours before NCS reduced non-fatal MI but increased total mortality, stroke, and clinically important hypotension
- Lesson: Beta-blockers save hearts but may kill patients through stroke and hypotension when started acutely
Current recommendations:
- CONTINUE beta-blockers in patients already taking them (abrupt discontinuation causes rebound tachycardia and ischemia)
- Do NOT start beta-blockers in the immediate preoperative period (day of surgery)
- If starting new, begin 2-4 weeks before surgery with dose titration (target HR 60-65 bpm)
- Consider starting in patients with high RCRI score (≥3) undergoing vascular surgery if time permits titration
2. Statins
- Continue in patients taking them chronically (pleiotropic, anti-inflammatory, membrane-stabilizing effects)
- Consider starting in patients undergoing vascular surgery if not already taking
3. ACE Inhibitors / ARBs (RAASi)
- Associated with profound intraoperative hypotension due to inability to compensate with angiotensin II
- Hold for 24-48 hours preoperatively (2024 ACC/AHA recommendation) - though patient-specific decisions are needed
- Restart postoperatively when hemodynamically stable
4. Aspirin / Antiplatelet Therapy
- Primary prevention: Can discontinue perioperatively
- Secondary prevention (ASCVD): Continue perioperatively unless bleeding risk outweighs thrombosis risk
- Exceptions: Neurosurgery, spine surgery (catastrophic bleeding risk) - discontinue even in secondary prevention
5. Dual Antiplatelet Therapy (DAPT) & Coronary Stents
Critical timing windows:
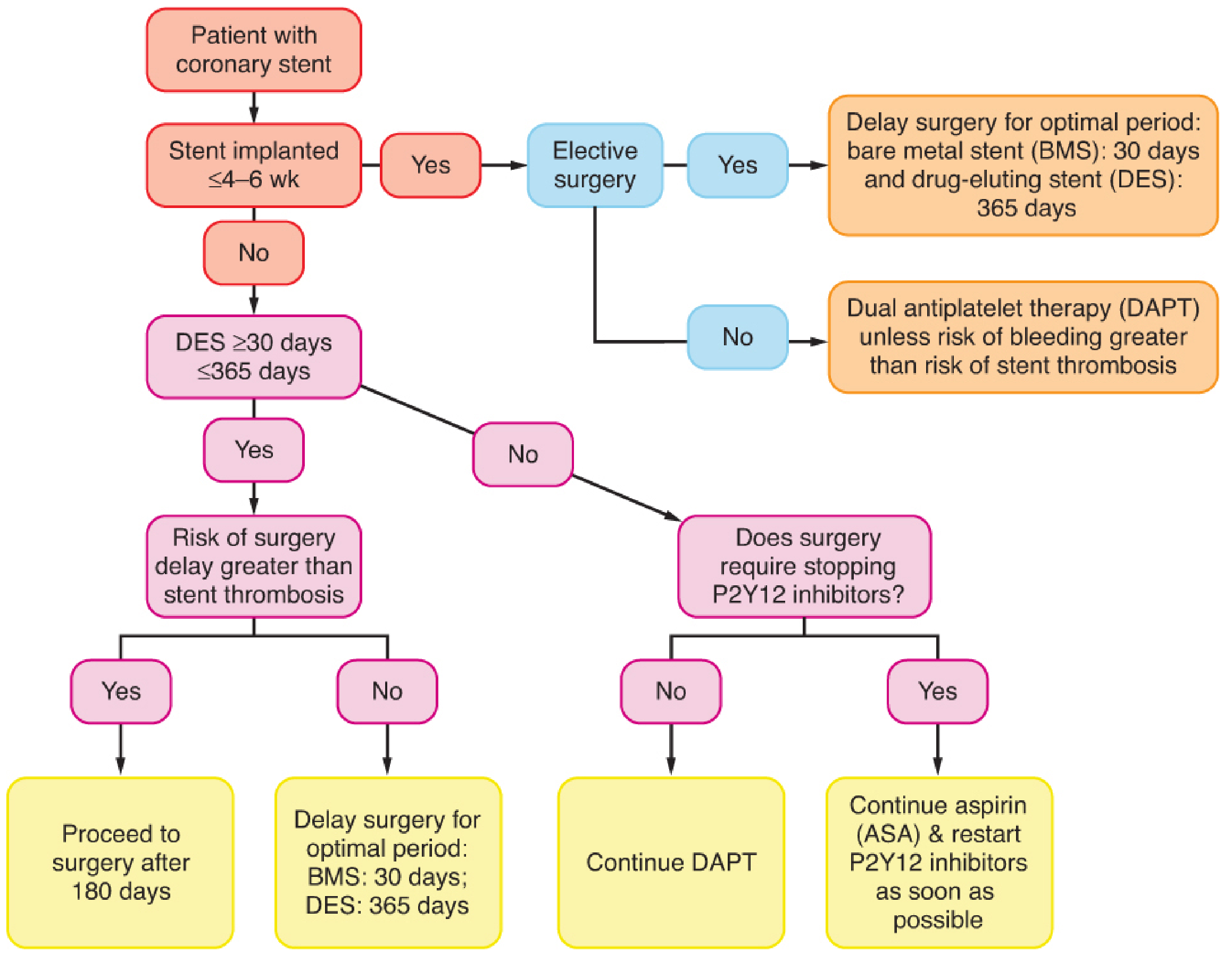
| Stent Type | Minimum delay for elective surgery |
|---|---|
| Bare Metal Stent (BMS) | 30 days (some say 4-6 weeks) |
| Drug Eluting Stent (DES) - old generation | 12 months (365 days) |
| New-generation DES | 6 months (per current evidence) |
Washout periods for P2Y12 inhibitors:
- Clopidogrel: 5 days
- Ticagrelor: 3-5 days
- Prasugrel: 7 days
If urgent surgery is required within these periods, continue aspirin (at minimum), proceed in a center with an available interventional cardiologist.
6. Anticoagulants (Bridging)
- Mechanical heart valves + warfarin: Bridging with UFH/LMWH is required
- AF + warfarin (stroke prophylaxis only): Bridging generally NOT necessary (BRIDGE trial)
- DOACs: Hold based on renal function and procedural bleeding risk; typically 24-48 hours for low-bleed, 48-72 hours for high-bleed procedures
7. Clonidine
- Early data suggested mortality benefit
- POISE-2 trial demonstrated clonidine increased nonfatal cardiac arrest and clinically important hypotension
- NOT recommended for perioperative cardiac risk mitigation
PART 8: ANESTHESIA CONSIDERATIONS - INTRAOPERATIVE
Choice of Anesthetic Technique
No convincing evidence that general vs. regional/neuraxial anesthesia is superior in terms of cardiac outcomes overall. The choice should be individualized.
Neuraxial (spinal/epidural) considerations:
- Provides excellent analgesia, reduces stress response, decreases DVT
- Sympathetic blockade can cause hypotension - requires careful titration in cardiac patients
- Contraindicated in patients on full anticoagulation (ASRA guidelines)
Monitoring:
- Standard ASA monitoring mandatory
- Invasive arterial line - for hemodynamically unstable patients or major vascular/thoracic surgery
- Central venous catheter - For vasopressor infusions, large-volume fluid shifts
- Pulmonary artery catheter (PA catheter) - Selective use in severe LV/RV dysfunction, pulmonary hypertension; not routine
- TEE (Transesophageal Echocardiography) - Excellent for real-time assessment of ventricular function, volume status, regional wall motion abnormalities
Hemodynamic Goals
- Maintain HR close to baseline (avoid tachycardia - increases O₂ demand, decreases diastolic filling time)
- Maintain adequate preload (especially in AS, HCM, RV dysfunction)
- Avoid hypotension (MAP goal: within 20% of baseline, or ≥65 mmHg)
- Optimize afterload according to underlying pathology
Specific Cardiac Conditions - Anesthetic Principles
Ischemic Heart Disease (CAD):
- Balance O₂ supply and demand
- Maintain coronary perfusion pressure (diastolic BP)
- Tachycardia is the most dangerous hemodynamic change
- Have vasopressors (phenylephrine, norepinephrine) and vasodilators (NTG) ready
Aortic Stenosis (AS):
- Maintain sinus rhythm and adequate HR (60-80 bpm)
- Avoid vasodilation (hypotension is catastrophic)
- Maintain preload (fixed stroke volume)
- Avoid sudden bradycardia or tachycardia
Aortic Regurgitation (AR):
- Favor slightly higher HR (60-90 bpm) to reduce regurgitant fraction and diastolic time
- Vasodilators are beneficial (reduce afterload)
- Avoid bradycardia
Mitral Stenosis (MS):
- Control HR strictly (avoid tachycardia - reduces filling time)
- Maintain sinus rhythm
- Avoid increase in pulmonary vascular resistance
Mitral Regurgitation (MR):
- Slightly elevated HR is acceptable
- Afterload reduction beneficial
- Avoid bradycardia and increased afterload
Hypertrophic Cardiomyopathy (HCM):
- Maintain intravascular volume (avoid hypovolemia)
- Avoid vasodilation and hypotension
- Avoid tachycardia
- Avoid inotropes
- Phenylephrine is vasopressor of choice (pure alpha, no increase in contractility)
Heart Failure with Reduced EF (HFrEF):
- Optimize volume status preoperatively (diuresis to euvolemia)
- Continue guideline-directed medical therapy
- Avoid negative inotropes
- Have inotropic support ready (dobutamine, milrinone)
- BNP/NT-proBNP helps guide timing
Pulmonary Hypertension:
- Very high-risk group
- Avoid hypoxia, hypercarbia, acidosis (all increase PVR)
- Maintain RV preload
- Consider inhaled NO or prostacyclins perioperatively
- Avoid vasodilators that drop systemic BP more than PVR
PART 9: CARDIOVASCULAR IMPLANTABLE ELECTRONIC DEVICES (CIEDs)
(Barash 9e, ASA 2020 Guidelines)
Pacemakers:
- Assess: type (pacemaker vs. ICD), programmed mode, underlying rhythm, pacemaker dependence
- Electrocautery EMI (electromagnetic interference) causes:
- Inhibition of pacing (worst in pacemaker-dependent patients)
- Inappropriate triggering of ICD shocks
- Bipolar cautery is safest
- Monopolar cautery above umbilicus = highest risk
- Pacemaker-dependent patient: reprogram to DOO or VOO mode (asynchronous) OR use magnet
ICDs:
- Magnet placement over ICD suspends tachytherapies (defibrillation/ATP)
- If tachytherapies disabled, attach external defibrillator
- Reprogram to original settings immediately postoperatively
PART 10: POSTOPERATIVE MANAGEMENT
Monitoring for MACE (Major Adverse Cardiac Events):
- Troponin surveillance (now recommended by 2024 ACC/AHA): Serial troponins at 24h and 48h postoperatively in high-risk patients
- Diagnose MINS (Myocardial Injury after Non-cardiac Surgery) - troponin elevation without classical MI criteria but still associated with 30-day mortality
Continue or restart medications:
- Restart beta-blockers and statins as soon as possible
- Restart antiplatelets per bleeding risk assessment
- Restart warfarin/DOACs once hemostasis is secure
Postoperative complications to anticipate:
- Perioperative MI (often silent in the OR due to anesthesia/analgesia)
- New-onset atrial fibrillation (common after major surgery)
- Acute decompensated heart failure
- Hemodynamic instability
PART 11: SPECIFIC HIGH-RISK SCENARIOS
Emergency Surgery in Cardiac Patient
- Proceed to OR immediately
- Risk-mitigation strategies:
- Invasive monitoring (arterial line, CVC)
- Perioperative beta-blockade if on chronically
- Vasopressors ready
- Cardiologist on standby
- Postoperative ICU/HDU care
Patient with Recent MI
- Within 30-60 days: Very high risk - delay elective surgery if possible
- After 60 days: Risk stabilizes but remains elevated
- Standard guidance: delay elective surgery 6 weeks after MI (some guidelines say 3 months for major surgery)
Patient with Recent PCI (see stent timing table above)
PART 12: VIVA QUESTIONS (MD ANAESTHESIA LEVEL)
Section A - Fundamental Concepts
Q1. What is the difference between "cardiac clearance" and perioperative cardiac evaluation?
"Cardiac clearance" implies a binary go/no-go decision. Perioperative cardiac evaluation is a nuanced risk stratification process that identifies active cardiac conditions, estimates procedural risk, determines if testing will change management, and optimizes medical therapy in the context of the planned surgery. No cardiologist can or should simply "clear" a patient for surgery.
Q2. Name the components of the Revised Cardiac Risk Index.
High-risk surgery, ischemic heart disease, congestive heart failure, cerebrovascular disease, insulin-dependent diabetes, chronic kidney disease (Cr >2 mg/dL). Each scores 1 point. RCRI 0 = 0.4%, RCRI 1 = 0.9%, RCRI 2 = 6.6%, RCRI ≥3 = 11% major cardiac complication risk.
Q3. What is the minimum MET threshold for adequate functional capacity? What is its significance?
4 METs - equivalent to climbing a flight of stairs or walking at 4 mph on level ground without symptoms. Patients with ≥4 MET capacity are considered to have adequate reserve for most non-cardiac surgeries. Poor functional capacity (<4 METs) is an indication for further cardiac evaluation before intermediate/high-risk surgery.
Q4. What are the active cardiac conditions that must be treated before elective non-cardiac surgery?
Unstable angina or recent MI, decompensated heart failure (NYHA IV), significant arrhythmias (high-degree AV block, sustained VT, SVT with rate >100 bpm), severe aortic stenosis, and symptomatic mitral stenosis.
Section B - POISE Trial & Beta-Blockers
Q5. Describe the POISE trial. What were its findings and implications?
POISE (PeriOperative ISchemic Evaluation) - 2008 RCT of ~8,000 patients. High-dose extended-release metoprolol (100 mg) started 2-4 hours before NCS and continued for 30 days. Results: Reduced non-fatal MI (4.2% vs 5.7%) but significantly increased total mortality (3.1% vs 2.3%), stroke (1.0% vs 0.5%), and clinically important hypotension (15% vs 9.7%). Net harm. Implication: Starting high-dose beta-blockers acutely in the perioperative period is harmful. Continue chronic beta-blocker therapy; if starting new, require weeks of titration.
Q6. If a patient on chronic beta-blockers comes for emergency surgery, what do you do?
Continue the beta-blocker. Abrupt discontinuation causes rebound catecholamine surge, reflex tachycardia, and precipitates MI/unstable angina. If NPO, convert to IV equivalent. Ensure HR is controlled.
Q7. What is the POISE-2 trial? What did it show about clonidine and aspirin?
POISE-2 - 2014 trial examining low-dose aspirin vs placebo and clonidine vs placebo perioperatively. Key findings: Aspirin did not reduce composite MACE endpoint vs placebo and increased major bleeding. Clonidine increased nonfatal cardiac arrest (0.8% vs 0.3%) and caused clinically important hypotension. Neither aspirin (unless secondary prevention) nor clonidine is recommended for perioperative cardiac risk reduction.
Section C - Stents, DAPT, and Anticoagulation
Q8. A patient with a drug-eluting stent placed 8 months ago requires appendicectomy. How do you manage antiplatelet therapy?
This is a time-sensitive (urgent) situation. At 8 months, DAPT has ideally been continued (standard 12 months for older-generation DES). For urgent/emergent surgery: continue aspirin perioperatively, stop clopidogrel 5 days before if time permits, restart P2Y12 inhibitor as soon as surgically safe. The anesthesiologist, surgeon, and cardiologist must jointly decide the risk of stent thrombosis vs. bleeding risk. A new-generation DES at 6+ months has lower thrombosis risk.
Q9. How is anticoagulation managed in a patient on warfarin for mechanical mitral valve who needs elective hernia repair?
Bridging anticoagulation is required. Stop warfarin 5 days before surgery. Start therapeutic LMWH (or UFH) when INR drops below 2.0. Hold last LMWH dose 24 hours before surgery (therapeutic dose). Resume warfarin and LMWH postoperatively until INR is therapeutic. For mechanical mitral valve, the risk of valve thrombosis without bridging is high; bridging is mandatory (unlike AF where bridging is generally not needed).
Q10. What is the BRIDGE trial? What does it tell us about bridging in AF patients?
BRIDGE trial (2015) - RCT of bridging LMWH vs no bridging in AF patients on warfarin undergoing surgery. Bridging did NOT reduce arterial thromboembolism but significantly increased major bleeding. Conclusion: Bridging anticoagulation is generally NOT necessary in AF patients with warfarin (where the indication is stroke prophylaxis). However, patients with mechanical valves, history of stroke/TIA, or very high CHA₂DS₂-VASc scores may still warrant bridging.
Section D - Specific Cardiac Conditions
Q11. What are the anesthetic goals in a patient with severe aortic stenosis posted for cholecystectomy?
Maintain: (1) Sinus rhythm - avoid AF or rapid ventricular rates; (2) HR 60-80 bpm - avoid tachycardia (reduces diastolic filling and subendocardial perfusion) and bradycardia; (3) Preload - adequate filling pressure as the LV is stiff and filling-dependent; (4) Systemic vascular resistance - any vasodilation can precipitate catastrophic hypotension; (5) Coronary perfusion pressure. Avoid spinal for major cases (sudden sympatholysis is dangerous). Careful, titrated epidural is preferable for regional. Intraoperative TEE is valuable.
Q12. What are the hemodynamic goals in hypertrophic obstructive cardiomyopathy (HOCM)?
The dynamic outflow obstruction worsens with: decreased preload, decreased afterload, increased contractility, and tachycardia. Goals: (1) Maintain/increase preload - avoid hypovolemia; (2) Increase afterload - vasopressors of choice is phenylephrine (pure alpha, no inotropic effect); (3) Slow HR - beta-blockers preferred; (4) Avoid inotropes (digoxin, dopamine, dobutamine); (5) Maintain sinus rhythm. Avoid spinal (acute preload reduction is catastrophic).
Q13. How does pulmonary hypertension affect perioperative management?
Pulmonary hypertension is among the highest-risk conditions for NCS (perioperative mortality 7-14% in severe cases). Key principles: (1) Avoid all triggers of increased PVR: hypoxia, hypercarbia, acidosis, hypothermia, pain, light anesthesia; (2) Maintain RV preload but avoid RV volume overload; (3) Vasopressors: norepinephrine for systemic hypotension, vasopressin useful (does not increase PVR); (4) Inhalational agents for pulmonary vasodilation if needed (inhaled NO, prostacyclins perioperatively); (5) Avoid high PEEP and high airway pressures; (6) Expert multidisciplinary consultation mandatory.
Section E - CIEDs and Monitoring
Q14. A pacemaker-dependent patient requires laparotomy. How do you manage the pacemaker?
Assess: type of device, pacemaker dependence, current programming. Plan: (1) Contact cardiologist/manufacturer for interrogation and reprogramming; (2) Reprogram to asynchronous mode (DOO or VOO) to prevent inhibition by electrocautery EMI; alternatively, magnet application converts to asynchronous mode; (3) Use bipolar cautery if possible; if monopolar, keep cautery pad distal to device and use short bursts; (4) Have external transcutaneous pacing ready; (5) Reprogram to original settings immediately postoperatively and re-interrogate device.
Q15. What is the significance of placing a magnet over an ICD during surgery?
A magnet placed over an ICD suspends tachytherapies (ATP and defibrillation), preventing inappropriate shocks triggered by EMI from electrocautery. The magnet does NOT affect pacing function of an ICD. If tachytherapies are suspended, an external defibrillator must be connected and ready. The magnet must be removed and the ICD must be re-interrogated postoperatively.
Section F - Advanced/Integrative Questions
Q16. What is MINS? How is it different from perioperative MI?
MINS (Myocardial Injury after Non-cardiac Surgery) - a newer concept from the VISION study. Defined as troponin elevation (>0.03 ng/mL for hs-troponin T) within 30 days of surgery, not necessarily meeting universal MI criteria (no required symptoms or ECG changes). MINS is independently associated with 30-day mortality (Hazard Ratio ~4). Approximately 8% of patients ≥45 years undergoing NCS develop MINS, mostly without ischemic symptoms. The 2024 ACC/AHA guidelines now recommend postoperative troponin surveillance in high-risk patients.
Q17. What role does BNP/NT-proBNP play in perioperative cardiac evaluation?
Natriuretic peptides are now formally incorporated into the 2024 ACC/AHA guidelines. Elevated preoperative BNP (>92 pg/mL) or NT-proBNP (>300 pg/mL) independently predicts perioperative MACE and mortality at 30 days. They are especially useful in: (1) Detecting undiagnosed heart failure; (2) Guiding timing of surgery in HF patients (diuresis to euvolemia); (3) Risk-stratifying patients with poor/unknown functional capacity. Postoperative natriuretic peptide elevation also predicts adverse events.
Q18. Should prophylactic coronary revascularization be done before high-risk non-cardiac surgery to reduce perioperative cardiac risk?
No. Multiple RCTs (CARP trial - Coronary Artery Revascularization Prophylaxis, 2004) and meta-analyses demonstrate that prophylactic PCI or CABG before NCS does NOT reduce perioperative or long-term MACE. Furthermore, PCI creates a new problem - mandatory DAPT and the attendant risk of stent thrombosis if DAPT is interrupted for surgery. Revascularization should only be considered if independently indicated (left main disease, severe triple-vessel disease with LV dysfunction, unstable ACS) regardless of the planned surgery.
Q19. A 65-year-old patient with EF 30% is scheduled for colectomy for cancer. What is your anesthetic plan?
Multidisciplinary approach (cardiologist, surgeon, anesthesiologist). Pre-op: Optimize HF therapy (ensure euvolemia, continue GDMT - ACEi/ARB, beta-blocker, MRA, SGLT2i if appropriate). Check BNP. ECG, echocardiogram. Hold ACEi 24-48 hours before surgery. Intraoperative: Invasive arterial line, CVP, consider TEE/PA catheter. Prefer combined general + epidural (reduces stress response; epidural analgesia reduces myocardial O₂ demand). Avoid negative inotropes; use volatile agents cautiously. Phenylephrine for hypotension initially, switch to norepinephrine if cardiac output compromised. Have inotropic support (dobutamine) ready. Careful fluid management. Post-op: ICU/HDU, serial troponins, restart medications, optimize pain control.
Q20. What is the significance of functional capacity assessment in the 2024 ACC/AHA guidelines? How has it changed?
The 2024 guidelines notably moved away from subjective self-reported functional capacity (DASI - Duke Activity Status Index) based on the METS study showing poor predictive value of subjective assessment. The new emphasis is on objective testing such as CPET (cardiopulmonary exercise testing) or natriuretic peptide measurement. However, the basic principle remains: patients with confirmed good functional capacity (≥4 METs objectively) can often proceed without further cardiac testing regardless of cardiac risk factors.
QUICK REFERENCE SUMMARY TABLE
| Key Topic | High-Yield Point |
|---|---|
| RCRI ≥3 | 11% cardiac complication risk |
| 4 METs | Threshold for adequate functional capacity |
| POISE Trial | Acute beta-blockers: reduce MI but increase mortality/stroke |
| Clonidine | POISE-2 - increases cardiac arrest; NOT recommended |
| BMS surgery delay | 30 days minimum |
| DES surgery delay | 6-12 months (new-gen: 6 months) |
| Clopidogrel washout | 5 days |
| Prasugrel washout | 7 days |
| Ticagrelor washout | 3-5 days |
| BRIDGE trial | No bridging needed for AF (not mechanical valve) |
| CARP trial | Prophylactic revascularization NOT beneficial before NCS |
| AS anesthesia | Maintain preload, SVR, sinus rhythm |
| HOCM | Phenylephrine is vasoconstrictor of choice |
| MINS | Troponin elevation post-op, even without MI symptoms; ~8% incidence |
| BNP cutoff | >92 pg/mL (BNP) or >300 pg/mL (NT-proBNP) = increased perioperative risk |
| Pacemaker-dependent + cautery | Reprogram to DOO/VOO or apply magnet |
| RAASi perioperatively | Hold 24-48 hours before surgery |
Sources:
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Chapter 23 (Preoperative Evaluation)
- Fuster and Hurst's The Heart, 15th Edition - Chapter 72 (Perioperative Management of CV Disease in NCS)
- Morgan and Mikhail's Clinical Anesthesiology, 7e - Chapter 21 (Anesthetic Management of Specific Conditions)
- Miller's Anesthesia, 10e
- 2024 AHA/ACC/ACS Guideline for Perioperative Cardiovascular Management for Noncardiac Surgery (Circulation 2024)
- 2022 ESC/ESA Guidelines on Cardiovascular Assessment for NCS (Eur Heart J 2022)
This is a shared conversation. Sign in to Orris to start your own chat.