I now have comprehensive data from Robbins Basic Pathology, Bradley & Daroff's Neurology, Henry's Clinical Diagnosis, Medical Microbiology, and PubMed. Let me now compose the full comprehensive teaching response.
MENINGITIS PATHOLOGY - COMPREHENSIVE EXAM-ORIENTED TEACHING MODULE
Based on Robbins & Kumar Basic Pathology (10e), Robbins & Cotran Pathologic Basis of Disease, Bradley and Daroff's Neurology in Clinical Practice, Henry's Clinical Diagnosis and Management, Medical Microbiology 9e, and recent PubMed evidence.
📌 PART 1: DEFINITION & CLASSIFICATION
Definition
Meningitis is an inflammatory process - typically infection-induced - involving the leptomeninges (pia + arachnoid) within the subarachnoid space.
- If inflammation extends into underlying brain parenchyma → meningoencephalitis
- Can also be non-infectious: chemical meningitis (ruptured epidermoid cyst), carcinomatous meningitis (metastatic cancer cells in subarachnoid space)
(Robbins Basic Pathology, p. 833)
Classification (Master Table)
| Type | Onset | Predominant Cell | Common Organisms | Glucose | Protein |
|---|
| Acute Pyogenic (Bacterial) | Hours - Days | Neutrophils (PMNs) | N. meningitidis, S. pneumoniae, E. coli, GBS | ↓↓ | ↑↑ |
| Aseptic (Viral) | Days | Lymphocytes | Enteroviruses (80%), HSV-2, HIV, mumps | Normal | Mildly ↑ |
| Chronic (TB/Fungal/Spirochetal) | Weeks - Months | Lymphocytes + plasma cells | M. tuberculosis, Cryptococcus, syphilis | ↓ (mod) | ↑↑ |
MEMORY TRICK - "BVT" for cell types:
- Bacterial → Busy neutrophils (PMNs)
- Viral → Virtuous lymphocytes
- TB/fungal → Tough lymphocytes (chronic)
📌 PART 2: ETIOLOGY BY AGE GROUP (HIGH-YIELD TABLE)
| Age Group | Most Common Organisms | Mnemonic |
|---|
| Neonates (0-3 months) | Group B Streptococci (S. agalactiae), E. coli (K1 strain), L. monocytogenes | "GEL" - Group B, E. coli, Listeria |
| Infants (3 mo - 5 yr) | N. meningitidis, S. pneumoniae, H. influenzae type b (pre-vaccine) | "NeSH" |
| Adolescents & Young Adults (15-24 yr) | N. meningitidis (most common) | "Neisseria hits teens" |
| Adults (20-60 yr) | S. pneumoniae (MC overall in adults), N. meningitidis | "Strep takes over with age" |
| Elderly (>60 yr) | S. pneumoniae, L. monocytogenes, gram-negative bacilli | "Listeria loves the elderly" |
| Immunocompromised | Cryptococcus neoformans, L. monocytogenes, gram-negatives | |
| Post-neurosurgery/Trauma | Staphylococci, gram-negative bacilli | |
| CSF Shunt | S. epidermidis, S. aureus | |
KEY EXAM POINT: S. pneumoniae is the #1 cause of bacterial meningitis in adults overall and has the highest mortality (20-30%). N. meningitidis is #1 in young adults/adolescents. After Hib vaccination, H. influenzae is now rare.
📌 PART 3: PATHOGENESIS & MOLECULAR MECHANISMS
Step-by-Step Pathogenesis Flowchart
Nasopharyngeal colonization (S. pneumoniae, N. meningitidis)
↓
Attachment to mucosal epithelium via pili/adhesins
↓
Invasion of mucosal barrier (IgA protease production by pathogens)
↓
Bacteremia / Hematogenous spread
↓
Crossing the Blood-Brain Barrier (BBB)
• Transcytosis through cerebral endothelial cells
• Trojan horse mechanism (inside phagocytes)
• Direct spread from sinusitis/otitis/mastoiditis
↓
Bacterial replication in CSF (low IgG, low complement, low PMNs normally)
↓
Release of bacterial components:
• LPS (gram-negatives) → TLR-4 activation
• Peptidoglycan/teichoic acid (gram-positives) → TLR-2 activation
↓
Pro-inflammatory cascade:
TNF-α, IL-1β, IL-6, IL-8, PAF, reactive oxygen species
↓
BBB disruption → Vasogenic edema
Neutrophil recruitment → Cytotoxic edema
CSF outflow obstruction → Interstitial/communicating hydrocephalus
↓
Raised ICP → Brain herniation
Vasculitis → Cerebral infarction
Cranial nerve compression
↓
Death / Neurological sequelae
Key Molecular Details for USMLE/NEET PG
| Mechanism | Detail |
|---|
| IgA protease | Cleaves secretory IgA → allows mucosal invasion by S. pneumoniae, N. meningitidis, H. influenzae |
| Polysaccharide capsule | Antiphagocytic; key virulence factor of S. pneumoniae, N. meningitidis |
| Lipopolysaccharide (LPS) | Triggers cytokine storm via TLR-4; drives most pathology in gram-negative meningitis |
| Pili (fimbriae) | Adhesion to nasopharyngeal epithelium in N. meningitidis |
| E. coli K1 antigen | Sialic acid capsule; mimics host tissue → evades complement in neonates |
| TNF-α & IL-1β | Increase BBB permeability; key mediators of cerebral edema |
| Matrix metalloproteinases (MMPs) | Degrade BBB tight junctions; contribute to vasogenic edema |
| Complement activation | C3a/C5a → neutrophil chemotaxis into CSF |
📌 PART 4: MORPHOLOGY (GROSS & MICROSCOPIC)
GROSS PATHOLOGY - ACUTE PYOGENIC MENINGITIS
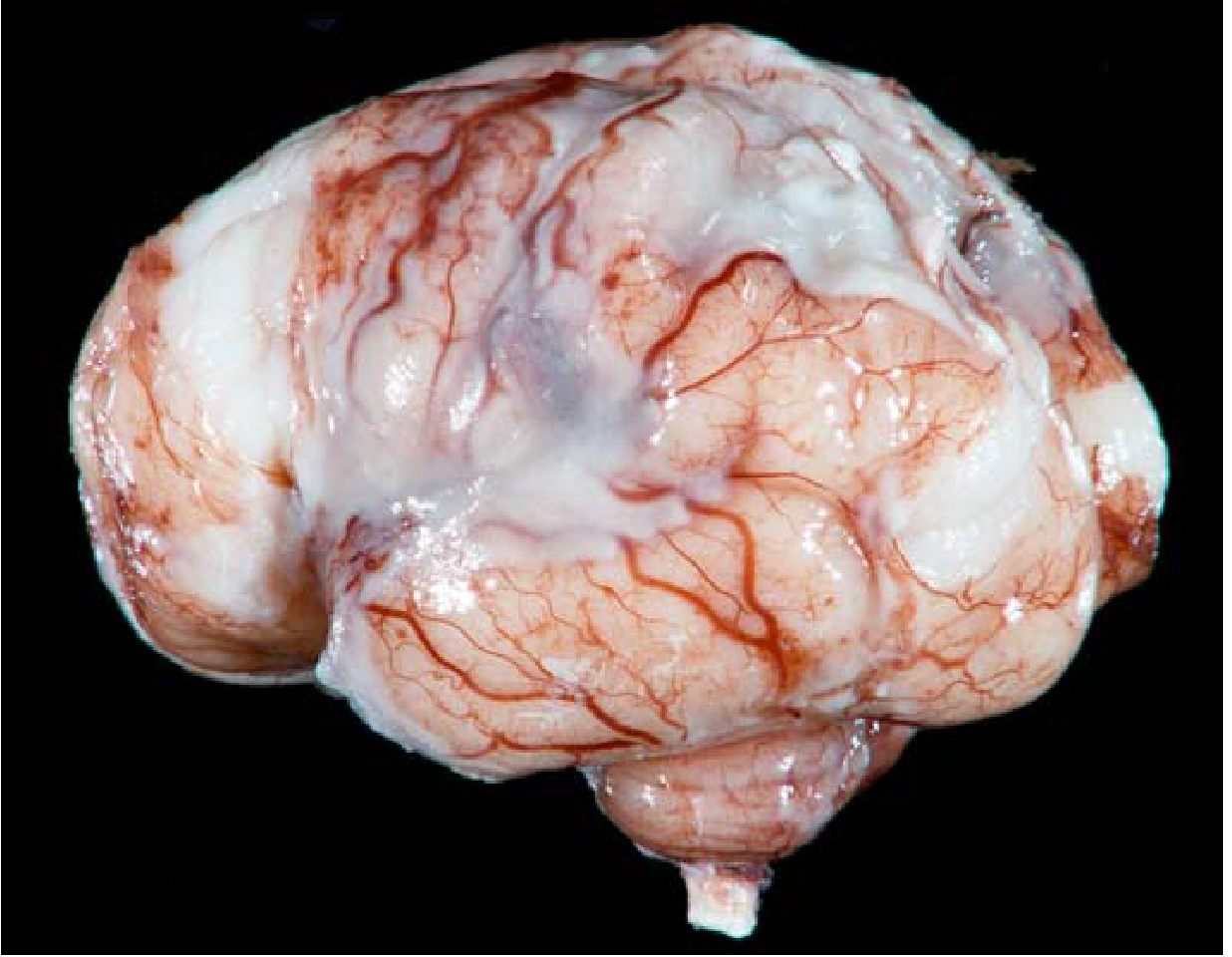
The classic image from Robbins Basic Pathology (Fig. 21.16):
FIG. 21.16 Pyogenic Meningitis (Robbins Basic Pathology): A thick layer of suppurative (yellowish-green, creamy) exudate covers the brain stem and cerebellum, thickening the leptomeninges. This is the hallmark gross finding.
What to look for on the gross specimen:
- Leptomeninges: opaque, thickened, yellow-gray-green purulent exudate filling the sulci
- Distribution: may be diffuse or focal (e.g., base of brain in TB, convexities in pneumococcal)
- Cerebral vessels: engorged, dilated (vascular congestion)
- Brain surface: edematous, gyri may be flattened due to raised ICP
- Subdural empyema: may coexist
- Hydrocephalus: in later stages
MICROSCOPIC PATHOLOGY
| Type | Microscopic Hallmark |
|---|
| Acute Bacterial | Subarachnoid space filled with neutrophils (PMNs) + fibrin + bacteria; meningeal vessels congested; meninges thickened |
| Viral (Aseptic) | Lymphocytic pleocytosis in subarachnoid space; perivascular lymphocytic cuffing; no bacteria |
| Tuberculous | Caseating granulomas with epithelioid cells + Langhans giant cells; basal exudate (predilection for base of brain); endarteritis obliterans |
| Cryptococcal | Mucoid encapsulated yeasts in subarachnoid/perivascular (Virchow-Robin) spaces; "soap bubble" appearance on gross section; minimal inflammation (due to immunosuppression); India ink preparation positive |
| Syphilitic (Meningovascular) | Chronic meningitis at base; obliterative endarteritis rich in plasma cells and lymphocytes |
EXAM PEARL: In cryptococcal meningitis - the CSF may show few cells but elevated protein. The fungal capsule inhibits phagocytosis AND suppresses host immune response.
📌 PART 5: RISK FACTORS
| Category | Specific Factors |
|---|
| Extremes of age | Neonates (immature immunity), elderly (waning immunity) |
| Immunocompromise | HIV/AIDS, transplant, steroids, chemotherapy → Listeria, Cryptococcus |
| Asplenia | Encapsulated organisms: S. pneumoniae, N. meningitidis, H. influenzae |
| CSF leaks/Skull fracture | Recurrent pneumococcal meningitis |
| Complement deficiency (C5-C9) | Recurrent N. meningitidis infections (MAC deficiency) |
| Crowded living | Military barracks, college dormitories → meningococcal outbreaks |
| Neurosurgery/Shunts | Nosocomial meningitis (S. epidermidis, gram-negatives) |
| Contiguous spread | Otitis media, sinusitis, mastoiditis |
| Unvaccinated status | H. influenzae, N. meningitidis, S. pneumoniae |
| Alcoholism, cirrhosis | S. pneumoniae, gram-negatives |
| Pregnancy | L. monocytogenes |
| Diabetes, malignancy, age >50 | L. monocytogenes |
MNEMONIC for Listeria risk factors - "DEAD LAD":
Diabetes, Elderly (>50), Alcohol, Depressed immunity, Liver disease, AIDS, Deficient cell-mediated immunity
📌 PART 6: CLINICAL FEATURES & CLINICOPATHOLOGICAL CORRELATIONS
Classic Triad (only in ~44% of cases - don't miss partial presentations!)
- Fever (bacterial toxin release + cytokine surge)
- Neck stiffness (nuchal rigidity) - meningeal irritation
- Altered consciousness/Headache - raised ICP
Meningeal Signs (Clinical-Pathological Correlation)
| Sign | How to Elicit | Positive Finding | Pathological Basis |
|---|
| Kernig's sign | Flex hip 90°, try to extend knee | Inability to extend knee beyond 135° (pain/resistance) | Inflamed nerve roots resist stretch |
| Brudzinski's sign | Passive neck flexion (supine) | Involuntary flexion of hips & knees | Inflamed meninges cause reflex hip/knee flexion |
| Jolt accentuation | Horizontal head rotation 2-3x/sec | Worsening headache | Increased CSF turbulence against inflamed meninges |
HIGH-YIELD: Kernig's and Brudzinski's are specific (~95%) but not sensitive (~50%) for bacterial meningitis. Don't rule out meningitis if signs are absent!
Other Clinical Features
- Photophobia (inflammation of meninges around optic nerves)
- Petechial/purpuric rash → N. meningitidis (meningococcemia with DIC - endotoxin effect)
- Papilledema (raised ICP - late sign; its presence may contraindicate immediate LP!)
- Cranial nerve palsies (CN III, IV, VI, VII) - from basal exudate especially in TB
- Seizures - cortical irritation
- Bulging fontanelle in infants (raised ICP)
- High-pitched cry in neonates
Waterhouse-Friderichsen Syndrome
- Fulminant meningococcemia with DIC
- Bilateral adrenal hemorrhage → acute adrenal insufficiency
- Petechiae → purpura → skin necrosis
- Shock, circulatory failure
- Pathology: fibrin thrombi in adrenal vessels + hemorrhagic infarction of both adrenals
- Mortality approaches 90% without treatment
📌 PART 7: CSF ANALYSIS - THE MOST IMPORTANT EXAM TABLE
| Parameter | Normal | Bacterial | Viral | TB/Fungal | Carcinomatous |
|---|
| Appearance | Clear | Turbid/Purulent | Clear/turbid | Clear/xanthochromic | Clear/xanthochromic |
| Opening pressure | 70-180 mmH₂O | ↑↑↑ (>300) | Normal to ↑ | ↑↑ | ↑ |
| WBC count | <5 cells/μL | ↑↑↑ (100-10,000) | ↑ (10-500) | ↑ (50-500) | Mildly ↑ or normal |
| Predominant cell | Lymphocytes | Neutrophils (PMN) | Lymphocytes | Lymphocytes | Malignant cells |
| Glucose (CSF/serum ratio) | >0.6 | ↓↓ (<0.4) | Normal (>0.6) | ↓ (<0.5) | ↓ |
| Protein | 15-45 mg/dL | ↑↑ (100-500) | Mildly ↑ (50-100) | ↑↑ (100-500) | ↑ |
| Gram stain yield | - | ~80% | Negative | 5-10% (AFB smear) | Cytology +ve |
| Culture yield | - | ~80-90% | Often negative | 45-90% | N/A |
| Special tests | - | Bacterial antigen, PCR | PCR (enterovirus, HSV) | ADA ↑, PCR | Cytology, flow cytometry |
MNEMONIC for Bacterial CSF - "PLNG":
Pressure ↑, Leucocytes (neutrophils) ↑↑, Normal glucose NO (glucose is ↓), Gram stain positive
Why is glucose low in bacterial meningitis?
- Bacteria consume glucose directly
- Impaired glucose transport across inflamed BBB
- Increased metabolic demand of inflammatory cells
ADA (Adenosine Deaminase) in CSF
- Elevated in TB meningitis (>10 IU/L is suggestive)
- Reflects lymphocyte/macrophage activation
- High-yield NEET PG/INICET exam point
📌 PART 8: LABORATORY DIAGNOSIS
Complete Workup
1. CSF Examination (Lumbar Puncture)
- Gold standard for diagnosis
- CAUTION: Perform CT scan first if papilledema, focal neurological deficits, or altered consciousness (risk of brain herniation)
- Classic LP finding in bacterial: "turbid, purulent, under high pressure"
2. Gram Stain of CSF
| Organism | Gram Stain Appearance |
|---|
| S. pneumoniae | Gram-positive diplococci (lancet-shaped) |
| N. meningitidis | Gram-negative diplococci (kidney-bean shaped, intracellular) |
| L. monocytogenes | Gram-positive short rods (may look like diphtheroids) |
| H. influenzae | Gram-negative coccobacilli |
| E. coli | Gram-negative rods |
| Group B Strep | Gram-positive cocci in chains |
3. Culture & Sensitivity - Blood culture + CSF culture (most sensitive)
4. Rapid Antigen Tests - Latex agglutination for polysaccharide antigens
5. PCR (most sensitive for viruses; increasingly used for bacteria)
- FilmArray Meningitis/Encephalitis Panel - detects 14 pathogens simultaneously
6. Special Stains
- India ink: Cryptococcus (capsule creates clear halo around yeast)
- AFB stain/Culture: TB meningitis
- VDRL in CSF: Neurosyphilis (high specificity; low sensitivity)
7. Serology
- Cryptococcal antigen (CrAg) in CSF/serum - very sensitive and specific
- HSV PCR in viral encephalitis
- Beta-glucan, galactomannan: fungal markers
8. Imaging
- CT scan (before LP if indicated): may show meningeal enhancement, hydrocephalus, cerebral edema, abscess, herniation
- MRI with gadolinium (superior): shows leptomeningeal enhancement ("tramtrack" pattern in TB at base of brain)
📌 PART 9: COMPLICATIONS
Acute Complications
| Complication | Mechanism |
|---|
| Brain herniation | Raised ICP → transtentorial herniation → death |
| Hydrocephalus | Exudate blocks CSF resorption at arachnoid granulations (communicating type) or CSF flow (obstructive type) |
| Cerebral infarction/stroke | Vasculitis of meningeal/cortical vessels (especially TB) |
| Subdural effusion/empyema | Bacterial invasion of subdural space |
| Ventriculitis | Spread to ependymal lining of ventricles |
| Septic shock, DIC | Especially meningococcal disease |
| SIADH | Hypothalamic irritation → hyponatremia |
| Waterhouse-Friderichsen | Meningococcemia → adrenal hemorrhage |
Chronic/Long-term Sequelae (MUST KNOW for exams)
- Deafness (sensorineural): MC long-term sequela of bacterial meningitis (S. pneumoniae #1, due to cochlear damage from inflammation + peri-labyrinthitis)
- Intellectual disability
- Epilepsy (cortical scarring)
- Focal neurological deficits
- Communicating hydrocephalus (chronic TB/post-bacterial)
- Visual impairment (optic nerve damage)
- Learning difficulties in children
EXAM PEARL: "Most common long-term sequel of meningitis = Sensorineural hearing loss"
- Answer for NEET PG, INICET, USMLE alike
📌 PART 10: DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Features |
|---|
| Viral meningitis | Lymphocytic CSF, normal glucose, self-limiting, no bacteria on gram stain |
| TB meningitis | Subacute onset, basal involvement, ADA ↑, AFB positive, lymphocytic CSF with very high protein |
| Encephalitis | Primarily parenchymal (altered consciousness, seizures, focal signs dominant; meningism may be mild) |
| Brain abscess | Focal symptoms, CT shows ring-enhancing lesion, CSF changes usually milder |
| Subarachnoid hemorrhage | "Thunderclap" headache, xanthochromic CSF, RBCs that don't clear |
| Cryptococcal meningitis | Immunocompromised host, india ink +ve, CrAg +ve, "soap bubble" lesions |
| Carcinomatous meningitis | Malignant cells in CSF, history of systemic cancer, multiple cranial nerve palsies |
| Mollaret meningitis | Recurrent aseptic meningitis, "Mollaret cells" (large epithelioid cells) in CSF, often HSV-2 related |
| Drug-induced meningitis | NSAIDs, TMP-SMX, IVIG exposure history; sterile CSF |
📌 PART 11: GENETIC/IMMUNOLOGICAL ASSOCIATIONS
| Genetic Defect | Associated Meningitis Risk |
|---|
| C5-C9 (MAC) deficiency | Recurrent Neisseria infections (meningococcal and gonococcal); most important complement-meningitis link |
| MBL (mannose-binding lectin) deficiency | Increased susceptibility to S. pneumoniae |
| IgA deficiency | Recurrent sinopulmonary infections → meningitis risk |
| Properdin deficiency | X-linked; severe N. meningitidis infections |
| Asplenia (functional or surgical) | Encapsulated organisms (OPSI - overwhelming post-splenectomy infection) |
| IL-12 / IFN-γ pathway defects | Susceptibility to mycobacterial infections including TB meningitis |
| IRAK4/MyD88 deficiency | Invasive pneumococcal disease |
📌 PART 12: TREATMENT OVERVIEW (Clinicopathological Framework)
Treatment is not the pathologist's domain, but you must understand it for clinicopathological integration.
Empirical Antibiotic Choices by Age (High-Yield)
| Age | Likely Organism | Empirical Treatment |
|---|
| 0-3 months | GBS, E. coli, Listeria | Ampicillin + Cefotaxime/Gentamicin |
| 3 months - 50 years | N. meningitidis, S. pneumoniae | 3rd gen Cephalosporin (Ceftriaxone/Cefotaxime) |
| >50 years / Immunocomp | S. pneumoniae, Listeria | Ceftriaxone + Ampicillin |
| TB meningitis | M. tuberculosis | HRZE + corticosteroids |
| Cryptococcal | Cryptococcus | Amphotericin B + Flucytosine → Fluconazole |
Adjunctive Dexamethasone
- Reduces neurological sequelae (especially hearing loss) in bacterial meningitis
- Recommended BEFORE or WITH first antibiotic dose
- Particularly beneficial for S. pneumoniae meningitis
- Mechanism: reduces TNF-α and IL-1β surge
📌 PART 13: RECENT ADVANCES (PubMed Evidence)
Based on recent systematic reviews:
-
Global Case Fatality Rate (van Ettekoven et al., JAMA Netw Open, 2024; PMID: 39093565): Over 80 years, global CFR of bacterial meningitis has decreased but remains 20-30% in high-income and >50% in low-income countries. S. pneumoniae has the highest CFR. This emphasizes the continued importance of vaccination.
-
Antibiotic Duration in Pediatric Meningitis (Sudo et al., Eur J Pediatr, 2024; PMID: 37870611): Shorter antibiotic courses may be comparable to longer ones for non-pneumococcal meningitis in children - an evolving area of practice.
-
FilmArray MEP Panel: Multiplex PCR detecting 14 pathogens simultaneously - now considered superior to culture for rapid diagnosis (result in ~1 hour vs 48-72 hours for culture).
-
Meningococcal serogroup B vaccine (MenB): Now part of routine vaccination in many universities; complementing ACWY vaccines.
-
Dexamethasone controversy: Recent meta-analyses continue to support adjunctive steroids for pneumococcal meningitis but show variable benefit for other pathogens.
📌 PART 14: IMAGE-BASED PATHOLOGY
Image 1 - GROSS PATHOLOGY: Pyogenic Meningitis
(Robbins Basic Pathology, Fig. 21.16)
What this image shows:
- Creamy/white-yellow suppurative exudate coating the brain surface, filling sulci
- Leptomeninges appear opaque and thickened
- Congested meningeal blood vessels visible
- Exudate concentrated on the convexities and brain stem
Exam question based on this image: "Which organism most likely caused the findings shown in this gross brain specimen, if the patient was a 20-year-old college student?" → Answer: Neisseria meningitidis
Image 2 - Brain Cross-Section with Dark Lesions (Cryptococcal/Perinatal)
(Robbins Fig. showing cross-section with dark irregular areas)
- The first image fetched (cross-section) showed dark irregular areas = areas of tissue destruction from Cryptococcal spread in perivascular spaces, creating the characteristic "soap bubble" lesions
📌 PART 15: MCQ BANK - EXAM-STYLE QUESTIONS
SET A: NEET PG / INICET / FMGE STYLE MCQs
Q1. A 19-year-old medical student develops sudden severe headache, fever, and non-blanching petechial rash. LP shows neutrophilic pleocytosis. The organism most likely responsible secretes:
- (A) Exotoxin A
- (B) Endotoxin (LPS)
- (C) Streptolysin O
- (D) Tetanospasmin
Answer: B - N. meningitidis (gram-negative diplococcus) releases LPS (endotoxin) which activates complement and TLR-4, causing cytokine storm, DIC, and petechiae.
Q2. A neonate presents with bulging fontanelle, fever, and high-pitched cry. CSF shows gram-positive cocci in chains. The most likely organism is:
- (A) S. pneumoniae
- (B) Group B Streptococcus (S. agalactiae)
- (C) N. meningitidis
- (D) L. monocytogenes
Answer: B - GBS is gram-positive cocci in chains and is #1 cause of neonatal meningitis along with E. coli.
Q3. The CSF in viral meningitis shows which pattern?
- (A) Neutrophils, low glucose, high protein
- (B) Lymphocytes, normal glucose, mildly elevated protein
- (C) Neutrophils, normal glucose, normal protein
- (D) RBCs, xanthochromia, high protein
Answer: B - Classic viral CSF pattern.
Q4. Recurrant Neisseria meningitidis infections should prompt investigation for deficiency of:
- (A) IgA
- (B) C1q
- (C) Membrane Attack Complex (C5-C9)
- (D) MBL
Answer: C - MAC deficiency is strongly associated with recurrent Neisseria infections.
Q5. A 55-year-old diabetic patient develops subacute meningitis. India ink preparation of CSF shows encapsulated yeast with clear halos. The findings are consistent with:
- (A) Histoplasma capsulatum
- (B) Cryptococcus neoformans
- (C) Candida albicans
- (D) Aspergillus fumigatus
Answer: B - India ink positive, encapsulated yeast = Cryptococcus. The capsule creates clear halo against black ink.
Q6. The most common long-term sequel of bacterial meningitis is:
- (A) Epilepsy
- (B) Hydrocephalus
- (C) Sensorineural hearing loss
- (D) Intellectual disability
Answer: C - Sensorineural hearing loss is the most common sequel, due to spread to cochlea/labyrinth via subarachnoid space.
Q7. Gross pathology of bacterial meningitis shows "exudate in the sulci." Microscopically, the subarachnoid space is filled with:
- (A) Lymphocytes and plasma cells
- (B) Eosinophils
- (C) Neutrophils (PMNs) and fibrin
- (D) Granulomas with caseous necrosis
Answer: C - Acute pyogenic meningitis = neutrophilic exudate in subarachnoid space.
Q8. Assertion: Dexamethasone is given before or with the first dose of antibiotics in bacterial meningitis.
Reason: Dexamethasone reduces cytokine release and decreases the risk of sensorineural hearing loss.
- (A) Both A and R true; R is correct explanation
- (B) Both true; R is not correct explanation
- (C) A true, R false
- (D) A false, R true
Answer: A - Both correct and R explains A. Dexamethasone (a glucocorticoid) given early reduces TNF-α/IL-1β surge and cochlear damage.
Q9. "Soap bubble" appearance on brain cross-section is seen in:
- (A) Pyogenic brain abscess
- (B) Glioblastoma multiforme
- (C) Cryptococcal meningoencephalitis
- (D) Cerebral toxoplasmosis
Answer: C - Mucoid Cryptococcus spreads in Virchow-Robin spaces → "soap bubble" lesions on gross cross-section.
Q10. Waterhouse-Friderichsen syndrome is characterized by all of the following EXCEPT:
- (A) Bilateral adrenal hemorrhage
- (B) DIC
- (C) Purpuric rash
- (D) Unilateral cranial nerve palsy
Answer: D - WF syndrome features: bilateral adrenal hemorrhage, DIC, shock, purpuric rash - it does NOT typically present with unilateral CN palsy (that is more characteristic of TB/fungal basilar meningitis).
SET B: USMLE STEP 1 STYLE QUESTIONS
Q11. A 22-year-old college freshman presents to the ER with 8-hour history of severe headache, photophobia, neck stiffness, and a petechial rash spreading over his legs. Temperature is 39.8°C. BP is 88/60 mmHg. Which of the following is the most appropriate NEXT step in management?
- (A) Lumbar puncture immediately
- (B) Blood cultures followed by LP
- (C) CT scan of head then LP
- (D) Blood cultures, then immediate empirical antibiotics and dexamethasone, followed by LP when feasible
- (E) MRI brain with gadolinium
Answer: D - This is classic meningococcal meningitis with early septic shock. Do NOT delay antibiotics for LP or imaging. In the presence of hemodynamic instability or signs of septicemia, blood cultures → immediate antibiotics. CT before LP is needed only if there are focal deficits/papilledema/immunocompromise. USMLE key: never delay antibiotics waiting for diagnostics.
Q12. Pathology of the brain shown below would most likely be from a patient with:
(Describing the gross image: creamy exudate in sulci, opaque leptomeninges)
- (A) Viral encephalitis
- (B) Bacterial meningitis
- (C) Glioblastoma multiforme
- (D) Multiple sclerosis
Answer: B - Purulent exudate in subarachnoid space is the hallmark of bacterial (pyogenic) meningitis.
Q13. A 65-year-old woman who recently completed chemotherapy develops meningitis. CSF gram stain shows gram-positive rods. She ate a salad from a deli. The most likely organism has which characteristic pathogenic mechanism?
- (A) Endotoxin releasing, gram-negative
- (B) Intracellular pathogen that crosses M cells; acquired via contaminated food
- (C) Polysaccharide capsule, transmitted via respiratory droplets
- (D) Transforms to filamentous form in tissue
Answer: B - L. monocytogenes - gram-positive rods, facultative intracellular, acquired via contaminated deli meats/soft cheese, infects the immunocompromised and elderly.
SET C: CASE-BASED DISCUSSION
CASE: A 2-day-old neonate born to a mother who had fever and UTI during the third trimester is brought in with poor feeding, temperature instability, and a bulging fontanelle. CSF: WBC 850/μL (80% neutrophils), protein 180 mg/dL, glucose 20 mg/dL (blood glucose 80 mg/dL). Gram stain shows gram-negative rods.
Discussion Points:
- Diagnosis: Neonatal bacterial meningitis due to E. coli (K1 strain) - gram-negative rods, neutrophilic CSF, low glucose
- Source: Maternal urogenital tract infection; vertical transmission during birth or transplacental
- Why is glucose low? Bacteria consume glucose + impaired transport
- K1 antigen significance: Sialic acid capsule resists complement-mediated killing in the neonate (low IgG, low complement levels normally in neonates)
- Treatment: Ampicillin + Cefotaxime (covers GBS and E. coli)
- Worst complication to fear: Cerebral vein thrombosis, hydrocephalus, ventriculitis, white matter injury → intellectual disability
- CSF/Blood glucose ratio: 20/80 = 0.25 (markedly low; normal >0.6) - confirms bacterial etiology
📌 PART 16: MNEMONICS MASTER LIST
| Topic | Mnemonic |
|---|
| Bacterial meningitis organisms by age | "GEL" (neonates: GBS, E.coli, Listeria); "NESH" (children: Neisseria, E.coli, Strep, H.flu); "SLG" (elderly: Strep pneumo, Listeria, Gram-negatives) |
| CSF bacterial meningitis | "PLNG" - Pressure ↑, Leukocytes (PMN) ↑, No glucose (↓), Gram stain + |
| Listeria risk factors | "DEAD LAD" - Diabetes, Elderly, Alcohol, Depressed immunity, Liver disease, AIDS, Deficient CMI |
| Meningeal signs | "KB Jolt" - Kernig's, Brudzinski's, Jolt accentuation |
| Waterhouse-Friderichsen | "BAD SHock" - Bilateral Adrenal, DIC, Septic/Hemorrhagic shock |
| Encapsulated organisms (asplenia) | "SHiN" - S. pneumoniae, H. influenzae, N. meningitidis |
| Recurrent Neisseria | "MAC attack" - MAC (C5-C9) deficiency |
| CSF cell types | "BVT" - Bacterial=Busy (PMN), Viral=Virtuous (lymph), TB=Tough (lymph/mono) |
| Complications | "DEAFNESS" - Deafness, Epilepsy, Abscess/arteritis, Focal deficits, N/hypo-natremia (SIADH), Empyema, Stupor/coma, Shock (WF syndrome) |
📌 RAPID REVISION SHEET - TOPPER LEVEL
╔════════════════════════════════════════════════════════════════════╗
║ MENINGITIS RAPID REVISION - ONE PAGE SUMMARY ║
╠════════════════════════════════════════════════════════════════════╣
║ DEFINITION: Inflammation of leptomeninges (pia+arachnoid) ║
║ in subarachnoid space ║
╠════════════════════════════════════════════════════════════════════╣
║ ORGANISMS BY AGE: ║
║ • Neonates: GBS, E.coli K1, Listeria ║
║ • <5yr: N.meningitidis, S.pneumo, H.flu (pre-vaccine) ║
║ • Teens/Young adults: N.MENINGITIDIS (#1) ║
║ • Adults: S.PNEUMONIAE (#1 overall) ║
║ • Elderly/Immuno: S.pneumo + LISTERIA ║
║ • Immunocompromised: CRYPTOCOCCUS ║
╠════════════════════════════════════════════════════════════════════╣
║ CSF FINDINGS (★ Most repeated exam topic): ║
║ BACTERIAL: ↑↑PMN | ↓↓Glucose | ↑↑Protein | Turbid | ↑↑Pressure ║
║ VIRAL: ↑Lymph | Normal Glucose | Mildly↑Prot | Clear ║
║ TB: ↑Lymph | ↓Glucose | ↑↑Protein | ADA↑ | AFB stain ║
║ CRYPTO: ↑Lymph | ↓Glucose | ↑Protein | India ink + ║
╠════════════════════════════════════════════════════════════════════╣
║ GROSS PATH: Creamy purulent exudate in sulci; opaque meninges ║
║ MICRO PATH: Subarachnoid space filled with NEUTROPHILS (PMN) ║
║ + fibrin (acute bacterial) ║
║ LYMPHOCYTES (viral/TB) ║
║ GRANULOMAS + caseation (TB) ║
║ ENCAPSULATED YEAST in Virchow-Robin spaces (Crypto) ║
╠════════════════════════════════════════════════════════════════════╣
║ COMPLICATIONS: ║
║ • MC sequel = SENSORINEURAL HEARING LOSS ║
║ • Hydrocephalus (communicating) ║
║ • WF syndrome (meningococcal) ║
║ • Herniation (raised ICP) ║
║ • SIADH (hyponatremia) ║
╠════════════════════════════════════════════════════════════════════╣
║ GENETIC LINKS: ║
║ • C5-C9 (MAC) deficiency → Recurrent Neisseria ║
║ • Asplenia → SHiN organisms ║
║ • Properdin deficiency → severe meningococcal disease ║
╠════════════════════════════════════════════════════════════════════╣
║ KEY STAINS: ║
║ • India ink: Cryptococcus ║
║ • AFB stain (ZN): M.tuberculosis ║
║ • Gram stain: bacteria (80% yield in bacterial meningitis) ║
║ • VDRL (CSF): Neurosyphilis ║
╠════════════════════════════════════════════════════════════════════╣
║ TREATMENT PEARLS: ║
║ • DEXAMETHASONE before/with antibiotics (reduces hearing loss) ║
║ • Do NOT delay antibiotics waiting for CT/LP ║
║ • Neonates: Ampicillin + Cefotaxime ║
║ • Adults: Ceftriaxone ± Ampicillin (if >50yr/immunocomp) ║
║ • TB: HRZE + steroids ║
║ • Crypto: Ampho B + Flucytosine → Fluconazole ║
╠════════════════════════════════════════════════════════════════════╣
║ EXAM PEARLS (FREQUENTLY REPEATED): ║
║ ★ "Petechial rash + meningitis" = N.meningitidis ║
║ ★ "Recurrent Neisseria" = MAC (C5-C9) deficiency ║
║ ★ "Soap bubble brain" = Cryptococcal meningitis ║
║ ★ "WF syndrome" = bilateral adrenal hemorrhage from meningococcus ║
║ ★ "ADA elevated in CSF" = TB meningitis ║
║ ★ "Base of brain predilection" = TB and syphilitic meningitis ║
║ ★ "CSF: few cells but high protein" = Cryptococcal meningitis ║
║ ★ "Mollaret cells (large epithelioid cells) in CSF" = HSV-2 ║
║ ★ "#1 long-term sequel" = Sensorineural hearing loss ║
║ ★ "Dexamethasone" given BEFORE first antibiotic dose ║
╚════════════════════════════════════════════════════════════════════╝
📌 EXAMINER MUST-KNOW HIGH-YIELD FACTS
-
Robbins definition: Meningitis = inflammatory process involving leptomeninges within the subarachnoid space. If it spreads to brain parenchyma = meningoencephalitis.
-
Grossly: Pyogenic meningitis shows thick creamy suppurative exudate covering brain surface, especially basilar cisterns and cerebral convexities (Robbins Fig. 21.16).
-
Microscopically: Subarachnoid space packed with neutrophils (PMNs) + fibrin in acute bacterial; lymphocytes in viral; caseating granulomas in TB; encapsulated yeast in Cryptococcal meningitis.
-
TB meningitis: Predilection for base of brain (basilar meningitis); causes cranial nerve palsies, endarteritis obliterans, hydrocephalus. CSF shows lymphocytes, high protein, low glucose, elevated ADA.
-
Cryptococcal meningitis: "Soap bubble" lesion on cross-section; India ink positive; CSF may show minimal cells but high protein; C. gattii can affect immunocompetent; C. neoformans mainly immunocompromised.
-
WF syndrome: Meningococcemia → DIC → bilateral adrenal hemorrhage → acute adrenal insufficiency + shock + purpura fulminans.
-
Complement MAC deficiency (C5-C9): Classical association with recurrent Neisseria infections.
-
Why blood glucose ↓ in bacterial meningitis: Bacterial utilization + impaired BBB glucose transport.
-
Sensorineural hearing loss = MC long-term sequela of bacterial meningitis; worst with S. pneumoniae.
-
Dexamethasone before first antibiotic reduces TNF-α/IL-1β and prevents cochlear damage and neurological sequelae.
-
Listeria monocytogenes: Gram-positive rods (may resemble diphtheroids on gram stain); RESISTANT to cephalosporins (use ampicillin); affects elderly, pregnant, immunocompromised, neonates.
-
E. coli K1 antigen: Sialic acid capsule mimics host tissue; resists complement; major neonatal meningitis pathogen.
-
Viral meningitis (Aseptic): Enteroviruses account for 80% of cases; self-limiting; CSF = lymphocytosis, normal glucose, mildly elevated protein.
-
VDRL in CSF: For neurosyphilis diagnosis - high specificity, low sensitivity (false negatives occur).
-
ADA in CSF >10 IU/L: Strongly suggests TB meningitis - key NEET PG point.
Sources: Robbins & Kumar Basic Pathology 10e (p.833-836), Bradley and Daroff's Neurology in Clinical Practice, Henry's Clinical Diagnosis and Management by Laboratory Methods, Medical Microbiology 9e; supported by van Ettekoven et al. JAMA Netw Open 2024 (PMID: 39093565) and Sudo et al. Eur J Pediatr 2024 (PMID: 37870611).