Pain
Reading File
Asking for Preferences
Finding Sources
Searching the Web
pain physiology mechanisms nociception 2025
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Here is a thorough overview of the physiology and mechanisms of pain, drawn primarily from Harrison's Principles of Internal Medicine (22nd ed.) and supplemented by Rheumatology (Elsevier, 2022) and Sabiston Textbook of Surgery.
Pain: Physiology and Mechanisms
Definition
The International Association for the Study of Pain (IASP) defines pain as "an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage." This definition captures the key duality of pain: it is both a sensory experience and an emotional one. Acutely, pain is accompanied by behavioral arousal and a stress response - increased heart rate, blood pressure, pupil diameter, and plasma cortisol.
The Four Steps of Nociception
Tissue injury initiates a process called nociception, which proceeds through four stages:
| Step | Description |
|---|---|
| 1. Transduction | Noxious stimuli (thermal, mechanical, chemical) are converted into electrical signals at free nerve endings (nociceptors) |
| 2. Transmission | Electrical signals travel via peripheral nerve fibers (Aδ and C fibers) to the spinal cord, then ascend to the brain |
| 3. Modulation | The pain signal is enhanced or suppressed, primarily at the dorsal horn of the spinal cord |
| 4. Perception | The signal reaches the cerebral cortex; pain becomes a conscious, subjective experience |
Step 1 - Transduction: Peripheral Nociceptors
Nociceptors are free nerve endings distributed throughout somatic and visceral tissues (skin, joints, muscle, bone, viscera - but notably not the CNS itself, which is why awake craniotomy is possible).
They respond to multiple noxious stimuli:
- Intense heat or cold
- Intense mechanical distortion (pinch, pressure)
- Acidic pH changes
- Chemical irritants: ATP, serotonin, bradykinin (BK), histamine
A key molecular receptor is TRPV1 (transient receptor potential vanilloid 1, aka the vanilloid receptor), which is activated by heat, acidic pH, endogenous lipid mediators, and capsaicin.
Silent nociceptors are a special class of Aδ/C afferents that are normally unresponsive to mechanical or thermal stimuli, but become sensitized and activated during inflammation - explaining why inflamed tissue becomes disproportionately painful.
Step 2 - Transmission: Nerve Fibers and Pathways
The peripheral nerve contains three fiber types relevant to pain:
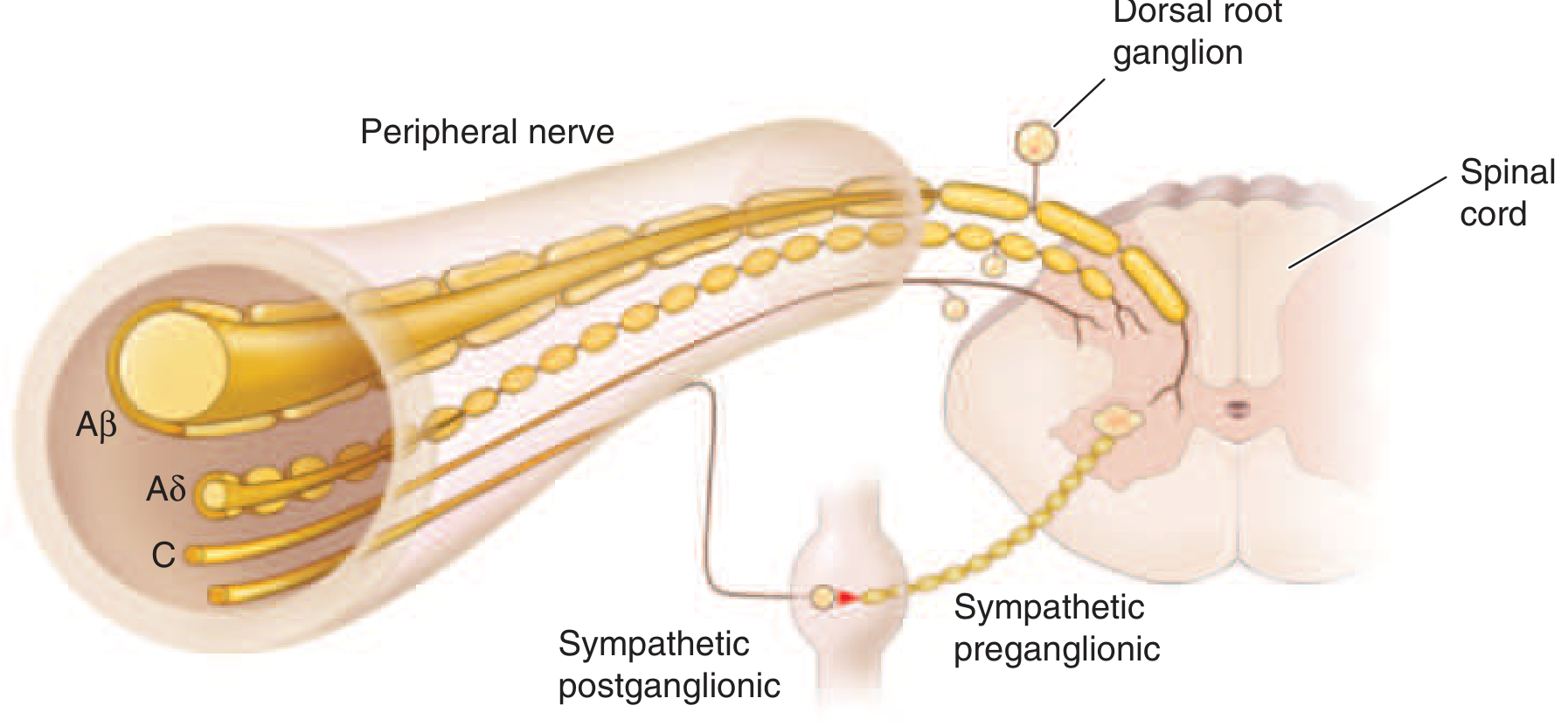
| Fiber | Diameter | Myelination | Function |
|---|---|---|---|
| Aβ | Large | Heavily myelinated | Light touch, moving stimuli - NOT pain under normal conditions |
| Aδ | Small | Thinly myelinated | Sharp, fast, well-localized "first pain" (thermal + mechanical) |
| C | Smallest | Unmyelinated | Dull, burning, aching "second pain"; polymodal |
The pathway from periphery to brain:
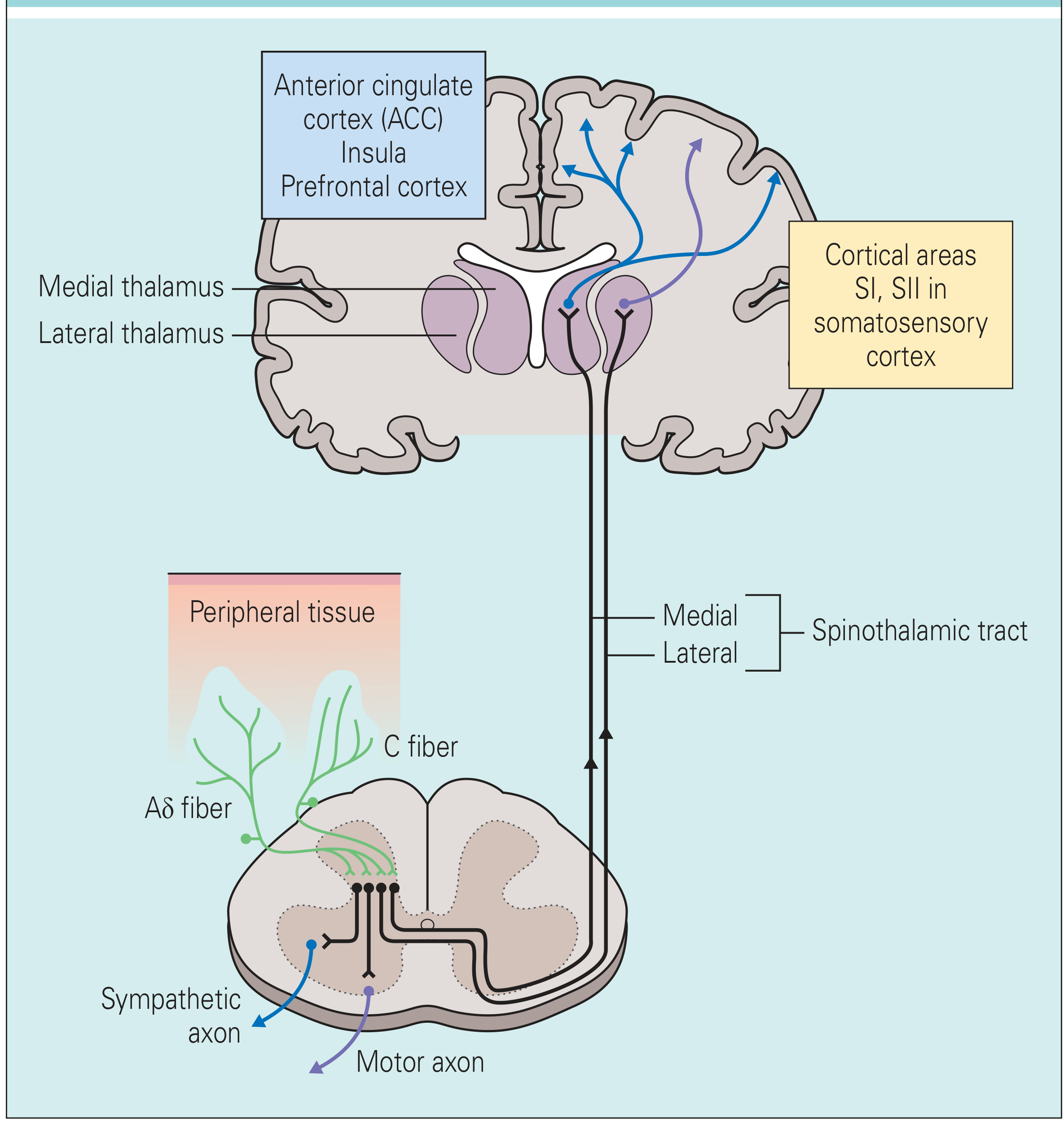
- Aδ and C fibers enter the spinal cord via the dorsal root and synapse in the dorsal horn (substantia gelatinosa)
- Second-order neurons cross to the contralateral side and ascend via the spinothalamic tract (anterolateral white matter)
- Fibers reach the thalamus (medial and lateral divisions)
- Thalamocortical projections diverge to:
- Somatosensory cortex (SI, SII) - localizes pain, encodes intensity and quality
- Anterior cingulate cortex (ACC) and insular cortex - the affective/emotional dimension of pain (suffering, fear, urge to escape)
Neurotransmitters at the dorsal horn:
- Glutamate - fast excitation of second-order neurons
- Substance P and CGRP - slower, longer-lasting excitation
Referred Pain
Each spinal pain-transmission neuron receives convergent inputs from both visceral afferents and skin afferents of the same spinal segment. Because the brain "assumes" the input is from the skin, pain from deep structures is mislocalized to the corresponding skin area. Example: diaphragmatic inflammation → shoulder pain (C3-C4 dermatome). This is the convergence-projection hypothesis of referred pain.
Step 3 - Modulation: Sensitization and Descending Control
Peripheral Sensitization
When tissues are damaged or inflamed, inflammatory mediators (bradykinin, prostaglandins, nerve growth factor, leukotrienes, low pH) lower the threshold and increase the firing frequency of nociceptors. Mechanistically, intracellular signaling increases the production and membrane insertion of ion channels, making the terminal hyperexcitable.
Result: allodynia (normally innocuous stimuli cause pain) and hyperalgesia (exaggerated pain response to a noxious stimulus). The classic example is sunburned skin - a gentle slap becomes intensely painful.
Central Sensitization
Persistent nociceptive input from inflamed tissue enhances the excitability of dorsal horn neurons in the spinal cord. This amplifies both:
- Primary hyperalgesia - pain at the injury site (shared with peripheral sensitization)
- Secondary hyperalgesia - enhanced pain sensitivity in healthy tissue surrounding the inflamed area
Nociceptor-Induced Neurogenic Inflammation
Primary afferents are not passive - when activated, they release substance P and CGRP from peripheral terminals, causing:
- Vasodilation
- Neurogenic edema
- Mast cell degranulation (histamine release)
- Platelet serotonin release
- Further recruitment of BK
This creates a self-amplifying loop of inflammation and pain.
Descending Modulation
A dedicated brain circuit modulates pain transmission at the dorsal horn:
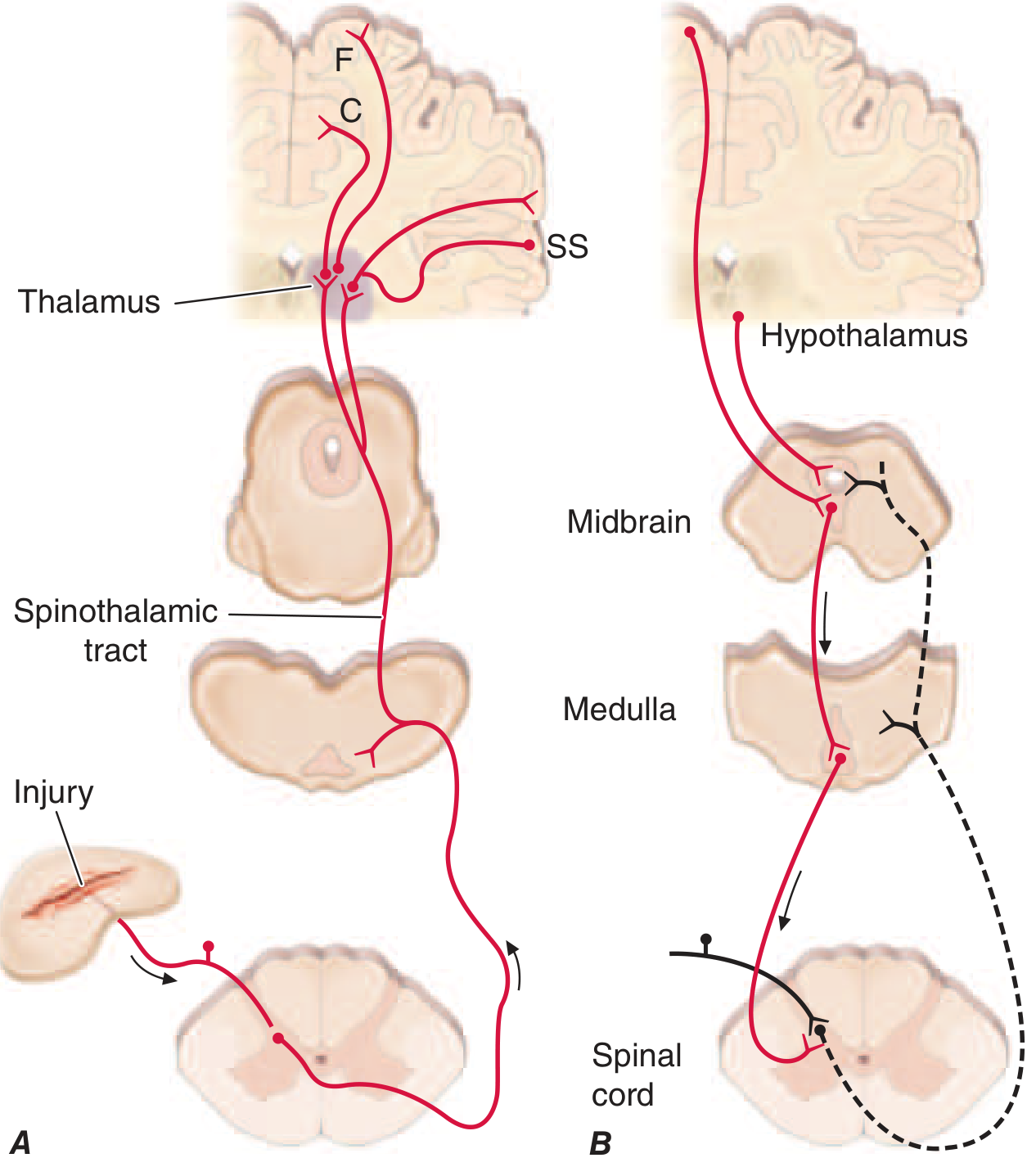
- Descending inhibitory pathway: Hypothalamus → periaqueductal gray (PAG, midbrain) → rostral ventromedial medulla (RVM) → dorsal horn. This circuit is rich in opioid receptors and endogenous opioid peptides (enkephalins, β-endorphin).
- Activated by: intense emotion, suggestion, distraction from the injury, opioid drugs, placebo analgesia
- The medulla also contains pain-facilitating neurons, which can enhance pain transmission - this circuit may underlie migraine, nocebo effects, and psychologically-mediated chronic pain.
Step 4 - Perception
Perception is the final, subjective experience when signals reach the cortex. It is modulated by attention, expectation, emotion, culture, and prior experience - explaining why identical injuries produce wildly different pain responses across individuals and situations (e.g., soldiers in battle vs. civilians). This is not "fake" pain; the affective and cognitive layers are neurologically real.
Neuropathic Pain
Damage to peripheral nerves or central pathways can paradoxically generate pain rather than loss of sensation. Mechanisms include:
- Ectopic discharge from damaged nerve fibers
- Ephaptic cross-talk between injured fibers
- Loss of central inhibitory interneurons
- Inappropriate sprouting of Aβ fibers into pain-specific laminae of the dorsal horn (so that light touch triggers pain)
Examples: diabetic neuropathy, post-herpetic neuralgia, phantom limb pain.
Sources:
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Chapter 14, "Pain: Pathophysiology and Management"
- Sabiston Textbook of Surgery - "Mechanisms of Acute Pain"
- Fischer's Mastery of Surgery, 8th ed. - "Etiology and Pathophysiology"
- Rheumatology, 2-Volume Set (Elsevier, 2022) - "Sensitization of Nociceptors"
This is a shared conversation. Sign in to Orris to start your own chat.