I want to learn all about electrolytes how its absorbed frim blood and then from tubules to where
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content and all the key diagrams. Let me compose the full answer.
Electrolytes: Absorption from the Gut and Reabsorption Along the Nephron
This guide covers two journeys: (1) how electrolytes enter the blood from the gut, and (2) once filtered at the glomerulus, how each nephron segment handles them before what remains exits as urine.
Part 1 - Intestinal Absorption (Gut → Blood)
(Source: Yamada's Textbook of Gastroenterology, 7e)
The small intestine receives about 8-9 liters of fluid daily (diet + secretions). The vast majority is reabsorbed; only 100-200 mL is lost to stool. This mass movement depends on active electrolyte transport that osmotically pulls water along.
Key Principles
Two routes across the intestinal epithelium:
- Transcellular - ions cross the apical membrane (lumen-facing), travel through the cytosol, and exit at the basolateral membrane (blood-facing). Requires at least one active step.
- Paracellular - passive movement through tight junctions, driven by gradients established by the active transcellular route.
The master driver is always Na⁺-K⁺-ATPase on the basolateral membrane. It pumps 3 Na⁺ out of the cell for every 2 K⁺ in, keeping intracellular Na⁺ very low. That low intracellular Na⁺ then becomes the driving force for all secondary active transporters on the apical side.
Electrolyte by Electrolyte
| Electrolyte | Mechanism of Absorption | Segment |
|---|---|---|
| Na⁺ | 1. Na⁺-glucose cotransporter (SGLT1) - nutrient-coupled; 2. Na⁺/H⁺ exchanger (NHE3) - electroneutral; 3. ENaC channels (electrogenic, aldosterone-regulated) | Small intestine + colon |
| Cl⁻ | Cl⁻/HCO₃⁻ exchanger (DRA/SLC26A3) - often in parallel with NHE3 making the process electroneutral; also through tight junctions following Na⁺ | Small intestine + colon |
| K⁺ | Mostly passive, following electrochemical gradient; actively secreted by KCNQ1 channels in small intestine; actively absorbed by H⁺-K⁺-ATPase in colon | Throughout |
| Ca²⁺ | Active transcellular via TRPV6 channels on apical membrane → calbindin carries through cytosol → PMCA1b pump/NCX1 exchanger exits basolaterally. Requires calcitriol (1,25-vitamin D) | Duodenum mainly |
| Mg²⁺ | TRPM6/TRPM7 channels on apical membrane; passive paracellular in small intestine | Jejunum/ileum |
| Phosphate | Na⁺-phosphate cotransporters (NaPi-IIb) on apical side, driven by Na⁺ gradient | Jejunum |
In the colon, the dominant process is electrogenic Na⁺ absorption via ENaC channels (controlled by aldosterone) with Cl⁻ following passively through tight junctions. The colon also actively secretes Cl⁻ via CFTR (the cystic fibrosis channel) - this is the pump that malfunctions in secretory diarrheas.
Part 2 - Renal Handling: From Glomerular Filtrate → Urine
Once electrolytes are in the blood, they are freely filtered at the glomerulus (except Ca²⁺ which is ~50% protein-bound). The filtered load then travels through four distinct tubular segments, each with specialized transport machinery. The master engine in every segment is the same: Na⁺-K⁺-ATPase on the basolateral membrane.
Segment 1 - Proximal Tubule (PT)
Reabsorbs ~65% of filtered Na⁺, Cl⁻, HCO₃⁻, K⁺, and essentially 100% of glucose and amino acids.
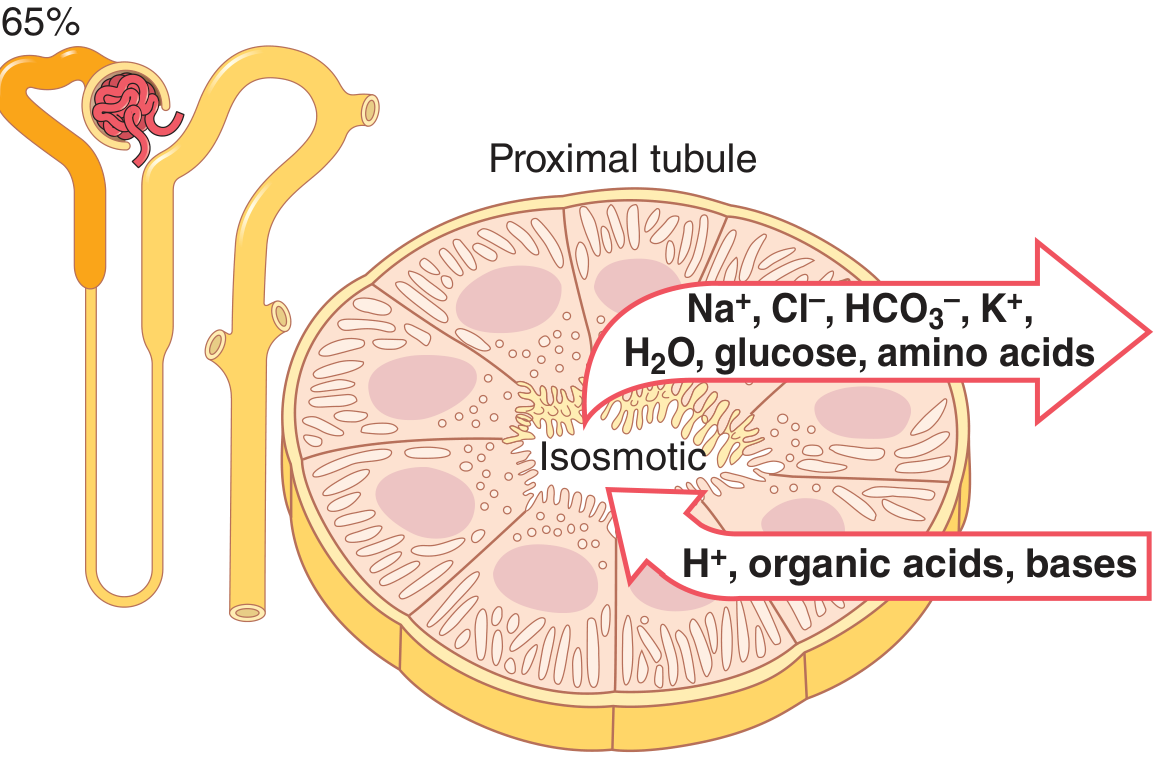
The cells have an extensive apical brush border (massive surface area) and are packed with mitochondria. Transport here is isosmotic - water follows every solute absorbed, so osmolarity doesn't change.
Early PT (Na⁺ coupled with organics):
- Na⁺-glucose cotransporter (SGLT2 → 90%, SGLT1 → 10%)
- Na⁺-amino acid cotransporters
- Na⁺/H⁺ exchanger (NHE3) → reabsorbs Na⁺, secretes H⁺ → HCO₃⁻ reclaimed
Late PT (Na⁺ coupled with Cl⁻):
- By this point glucose/amino acids are gone; Cl⁻ concentration is relatively high (~140 mEq/L)
- Cl⁻ diffuses passively through tight junctions (paracellular) and via chloride channels
- Na⁺ follows chloride (or is driven by ongoing NHE3 activity)
Ca²⁺ in the PT is reabsorbed passively in parallel with Na⁺/water (paracellular, ~60-70% of filtered load). PTH has no effect here - it is volume-dependent.
Phosphate in the PT is reabsorbed (75-80%) via Na⁺-phosphate cotransporters (NaPi-IIa, NaPi-IIc) on the apical membrane - secondary active transport driven by the Na⁺ gradient. PTH reduces these cotransporters → more phosphate lost in urine.
Source: Guyton and Hall Textbook of Medical Physiology
Segment 2 - Loop of Henle
Thin Descending Limb
- Highly permeable to water (aquaporins), poorly permeable to solutes
- As filtrate descends into the hypertonic medulla, water is pulled out osmotically → filtrate becomes concentrated
- No significant active ion transport
Thick Ascending Limb (TAL) - "the diluting segment"
Reabsorbs ~25% of filtered Na⁺, Cl⁻, K⁺, and large amounts of Ca²⁺ and Mg²⁺. IMPERMEABLE to water.
This is the segment where the key co-transporter NKCC2 (Na⁺-K⁺-2Cl⁻) operates. Loop diuretics (furosemide, bumetanide, ethacrynic acid) block NKCC2.
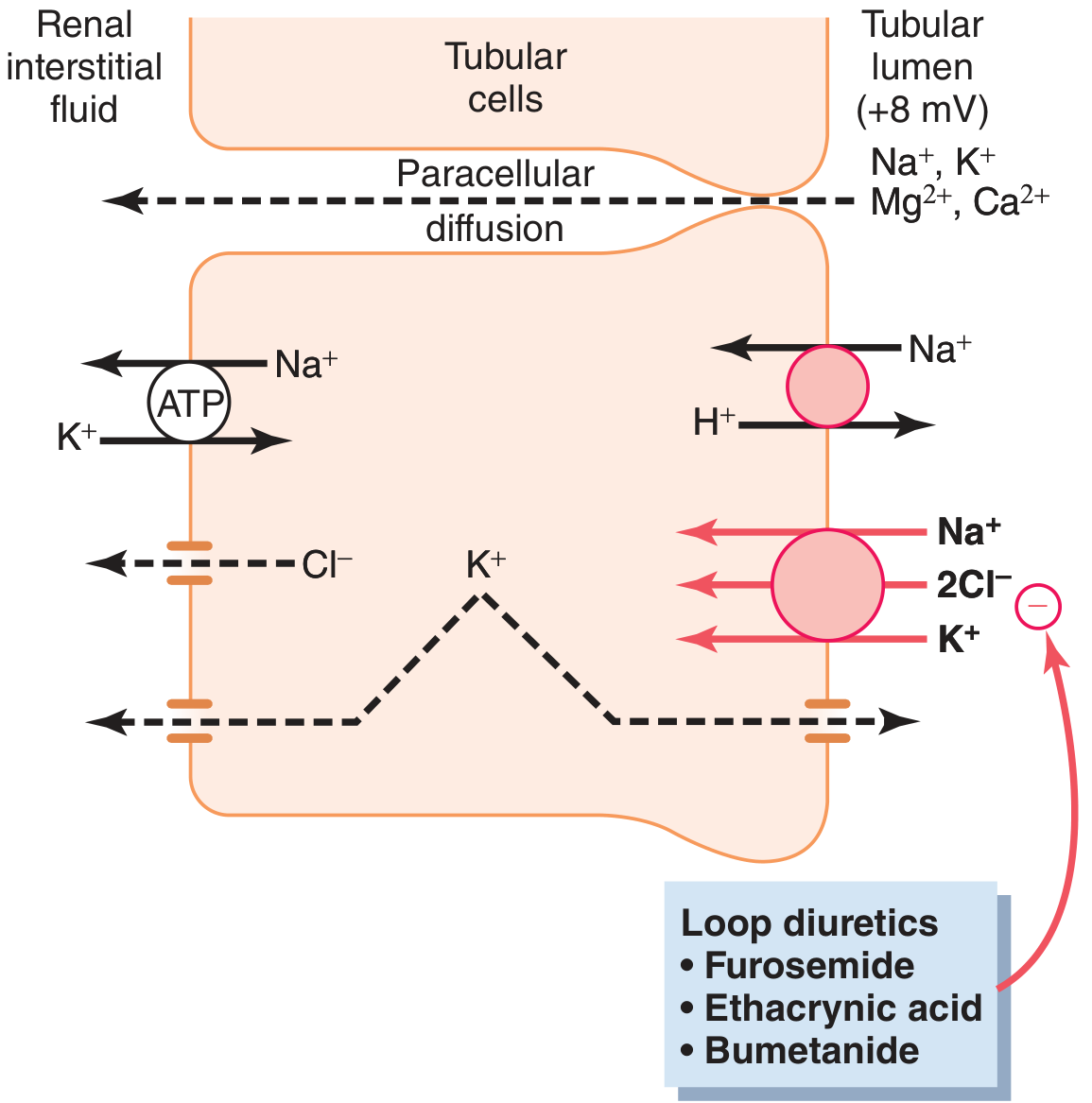
Mechanism:
- NKCC2 co-transports 1 Na⁺ + 2 Cl⁻ + 1 K⁺ into the cell (apical side) - secondary active, driven by Na⁺ gradient
- Na⁺-K⁺-ATPase pumps Na⁺ out basolaterally
- K⁺ recycles back into the lumen through ROMK channels → creates a +8 mV lumen-positive charge
- This positive lumen charge drives paracellular reabsorption of cations: Ca²⁺, Mg²⁺, Na⁺, K⁺
Because this segment is impermeable to water but actively removes solutes, the filtrate becomes hypotonic ("dilute") as it exits the loop - this is called the diluting segment.
Source: Guyton and Hall Textbook of Medical Physiology
Segment 3 - Distal Tubule
Early distal tubule (DCT): Reabsorbs Na⁺, Cl⁻, Ca²⁺, Mg²⁺. Also impermeable to water.
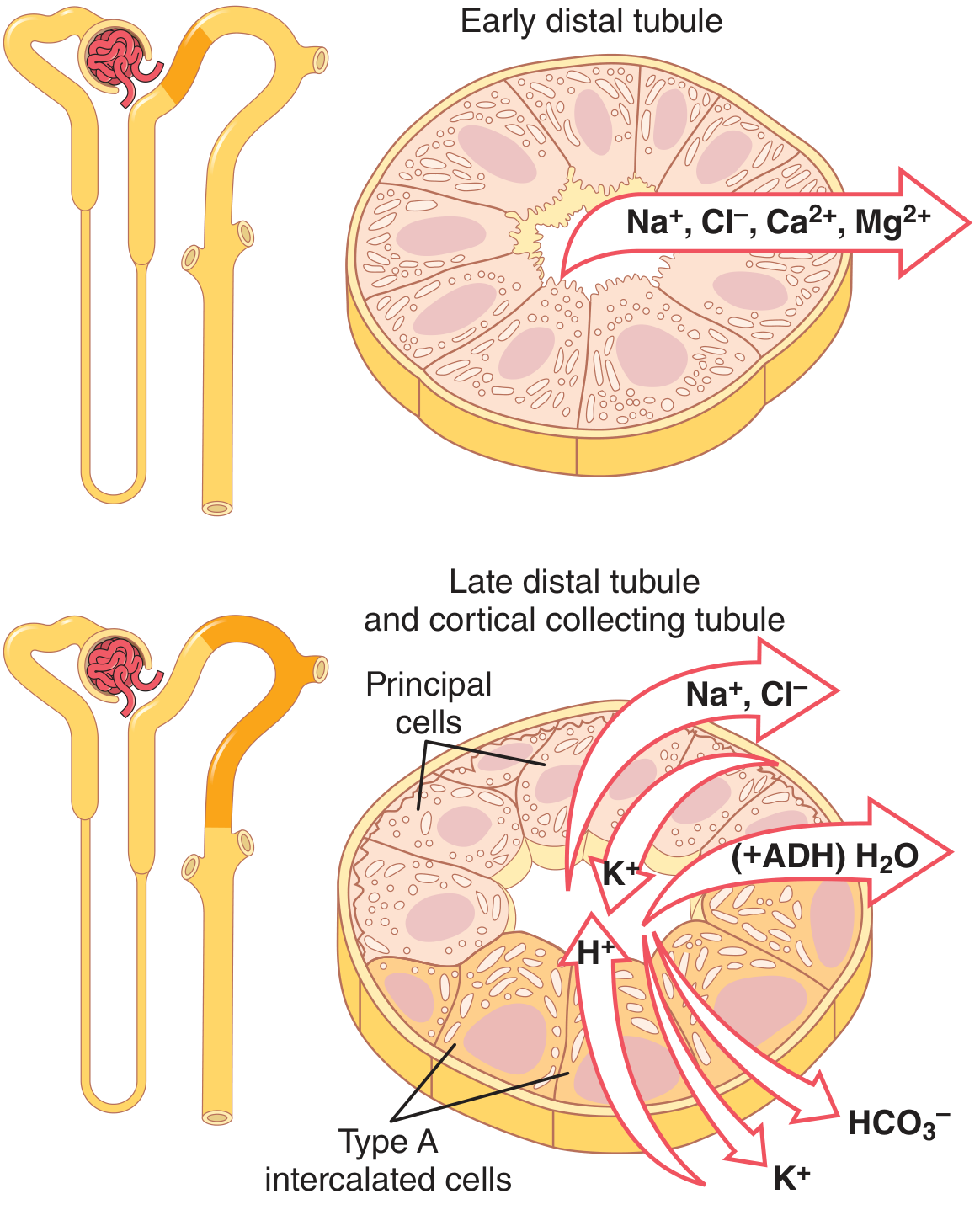
- NCC co-transporter (Na⁺-Cl⁻ cotransporter) on the apical membrane - blocked by thiazide diuretics
- Ca²⁺ is reabsorbed here entirely by transcellular active transport: enters via TRPV5 channels on the apical side → binds calbindin-D28k → exits via PMCA1b ATPase and NCX1 exchanger on the basolateral side. This is the main site regulated by PTH and calcitriol.
Late distal tubule and cortical collecting tubule contain two cell types:
Principal cells (regulated by aldosterone):
- Apical ENaC channels: Na⁺ enters passively down gradient
- K⁺ exits into lumen through ROMK channels (K⁺ secretion)
- Basolateral Na⁺-K⁺-ATPase drives it all
- Aldosterone increases ENaC and Na⁺-K⁺-ATPase expression → more Na⁺ in, more K⁺ out
- Spironolactone/eplerenone block aldosterone receptors; amiloride/triamterene block ENaC directly
Type A intercalated cells:
- Secrete H⁺ into lumen (H⁺-ATPase)
- Reabsorb K⁺ (H⁺-K⁺-ATPase) and HCO₃⁻ (via Cl⁻/HCO₃⁻ exchanger on basolateral side)
Source: Guyton and Hall Textbook of Medical Physiology
Segment 4 - Medullary Collecting Duct
- Continues Na⁺ reabsorption (principal cells, same ENaC mechanism)
- ADH (vasopressin) inserts aquaporin-2 (AQP2) channels → water reabsorption
- Permeable to urea (unlike cortical collecting duct) → urea transporters allow urea into the medullary interstitium, maintaining the high osmolality gradient that drives water reabsorption
- Capable of secreting H⁺ against steep gradients → key role in final urine acidification
Summary Table: Where Each Electrolyte Is Handled
| Electrolyte | PT | TAL | Early DCT | Late DCT / CCD | MCD | Final Urine |
|---|---|---|---|---|---|---|
| Na⁺ | 65% reabsorbed | 25% reabsorbed | ~5% | ~3% (aldosterone) | last trace | <1% filtered |
| K⁺ | 65% reabsorbed | 25-30% reabsorbed | variable | secreted (normally) | - | ~12% filtered |
| Cl⁻ | passive with Na⁺ | NKCC2 | NCC | with Na⁺ | - | small amount |
| HCO₃⁻ | ~85% (NHE3) | some | - | reabsorbed (intercalated) | secreted (intercalated) | variable |
| Ca²⁺ | 60-70% (passive) | 20% (paracellular) | 10% (active, PTH) | regulated by PTH/VitD | - | <2% filtered |
| Mg²⁺ | 10-15% | 60-70% (paracellular) | 5-10% | - | - | ~3-5% filtered |
| Phosphate | 75-80% (NaPi) | minimal | 10% | - | - | ~10% filtered |
Hormonal Control Summary
| Hormone | Site of Action | Effect |
|---|---|---|
| Aldosterone | Late DCT, CCD, MCD | ↑Na⁺ reabsorption, ↑K⁺ secretion, ↑H⁺ secretion |
| ADH (vasopressin) | DCT, CD | ↑Water reabsorption (AQP2) |
| Angiotensin II | PT, TAL, DCT, CD | ↑Na⁺, Cl⁻, HCO₃⁻ reabsorption |
| PTH | PT, TAL, DCT | ↓PO₄³⁻ reabsorption; ↑Ca²⁺ reabsorption |
| Atrial natriuretic peptide (ANP) | DCT, CD | ↓NaCl reabsorption (↑excretion) |
| Calcitriol (1,25-VitD) | TAL, DCT, gut | ↑Ca²⁺ and Mg²⁺ absorption/reabsorption |
Source: Guyton and Hall Textbook of Medical Physiology, Table 28.3
The Calcium Transport Machinery in Detail
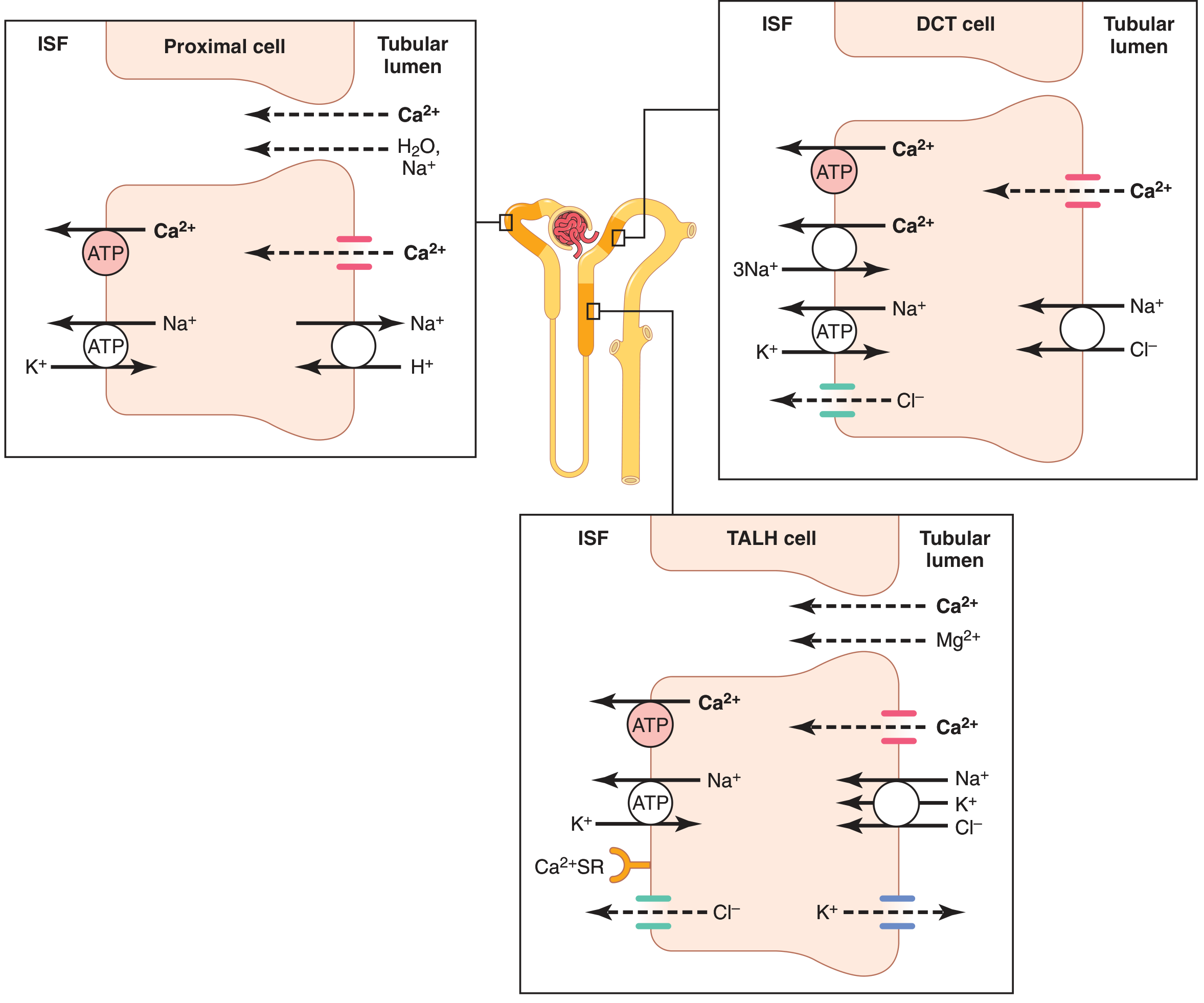
This diagram from Guyton nicely shows how different segments use different routes for Ca²⁺ - paracellular in the PT and TALH, active transcellular in the DCT - and how the calcium-sensing receptor (CaSR) on TALH cells directly senses plasma Ca²⁺ and regulates claudin-based paracellular permeability.
Potassium's Unique Journey
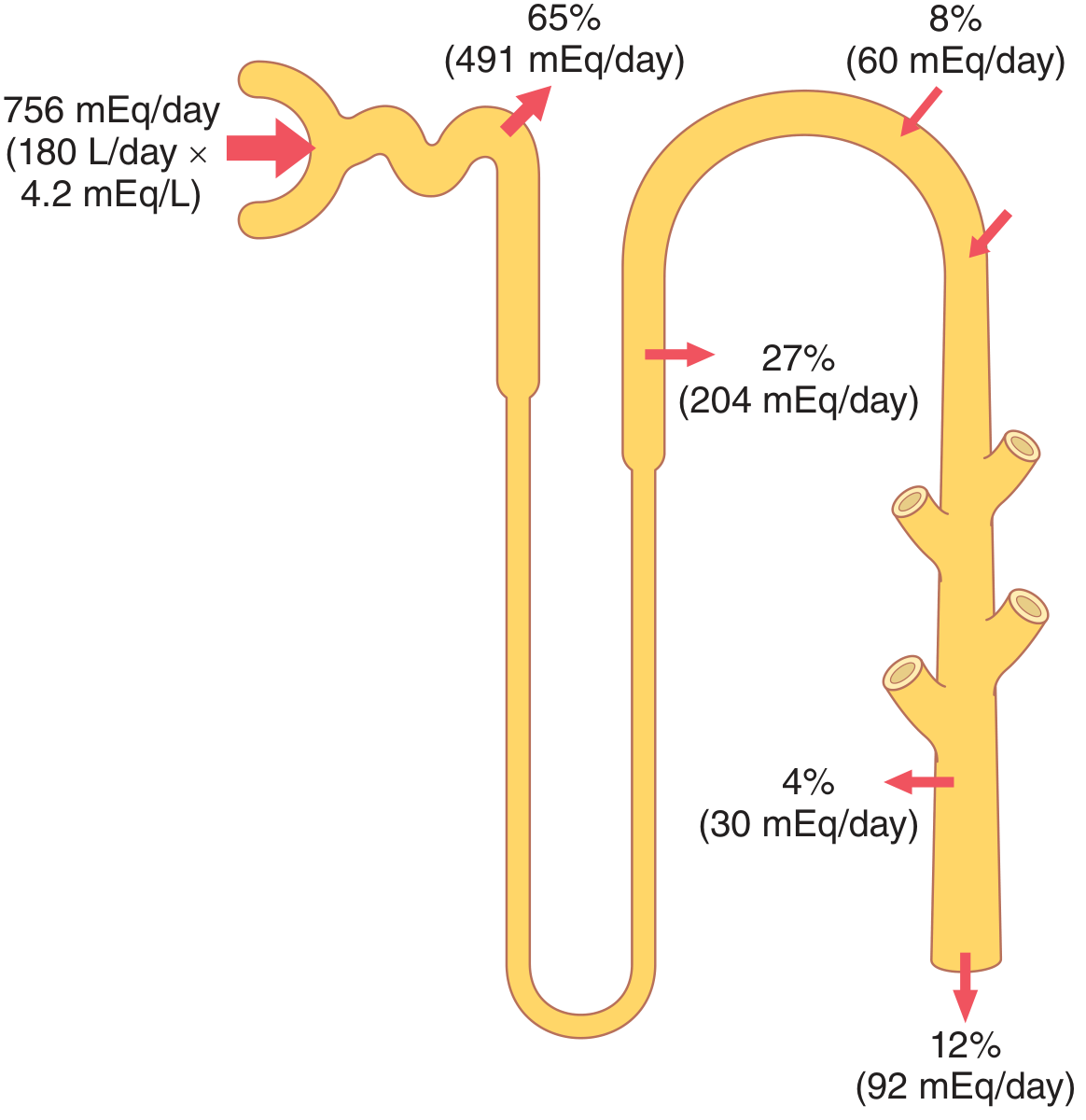
K⁺ is unique because it can be either secreted or reabsorbed in the distal nephron depending on body needs. On a high-K⁺ diet, aldosterone and direct K⁺ stimulation of principal cells increase secretion dramatically. On a very low-K⁺ diet, intercalated cells switch to active K⁺ reabsorption via H⁺-K⁺-ATPase. This flexibility means K⁺ excretion can range from <10 mEq/day to >400 mEq/day.
Source: Guyton and Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.