Plantar fasicitis etiology pathology signs and symptoms clinical tests investigation and treatment explain in detail with appropriate images illustrations and rehabilitation
Reading File
Finding Sources
Searching the Web
plantar fasciitis etiology pathology signs symptoms clinical tests treatment rehabilitation
Searching PubMed
"plantar fasciitis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Searching PubMed
"plantar fasciitis"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Searching the Web
plantar fasciitis windlass test clinical examination anatomy diagram
Loading Image
Loading Image
Reading File
Loading Image
Searching the Web
plantar fasciitis rehabilitation exercises stretching night splint orthotic images
Now I have all the material needed. Let me compile the comprehensive response.
Plantar Fasciitis: A Comprehensive Clinical Guide
1. Definition & Overview
Plantar fasciitis is the most common cause of plantar heel pain in adults, affecting millions annually. It is a degenerative irritation of the plantar fascia origin at the medial calcaneal tuberosity, with surrounding perifascial involvement. Despite its name, the condition is characterized by an absence of inflammatory cells in biopsy specimens - it is more accurately a degenerative fasciopathy (fasciosis) than a true inflammatory process.
Peak incidence is 40-60 years of age in the general population, with a younger peak in runners and athletes. It affects both sedentary and active individuals.
- Harrison's Principles of Internal Medicine 22E; Miller's Review of Orthopaedics 9th Ed.
2. Anatomy of the Plantar Fascia
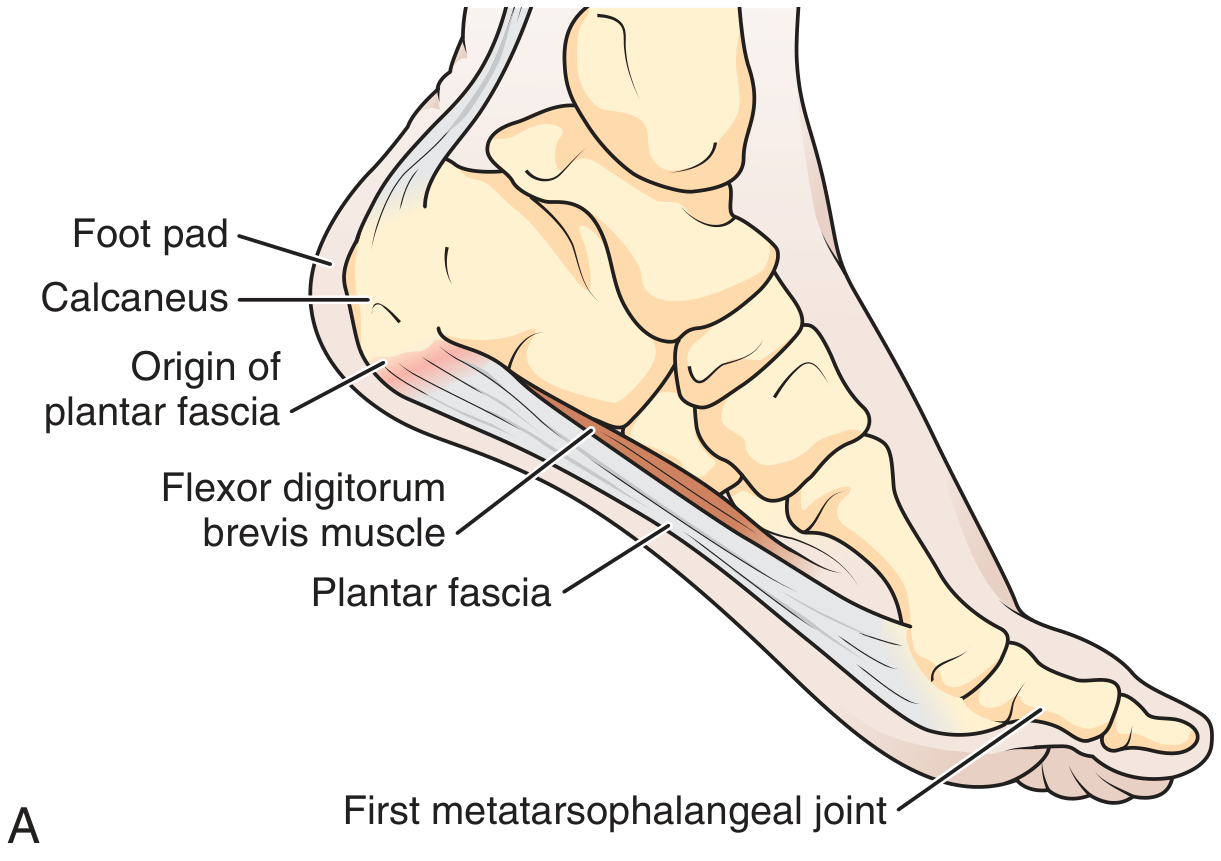
The plantar fascia is a thick fibrous aponeurosis comprising 3 segments (medial, central, lateral):
- Origin: Medial calcaneal tuberosity
- Course: Fans out across the entire plantar aspect of the foot
- Insertion: Splits and inserts into the plantar aspects of the proximal phalanges of all 5 toes
Functions:
- Supports the medial longitudinal arch
- Acts as a shock absorber during gait
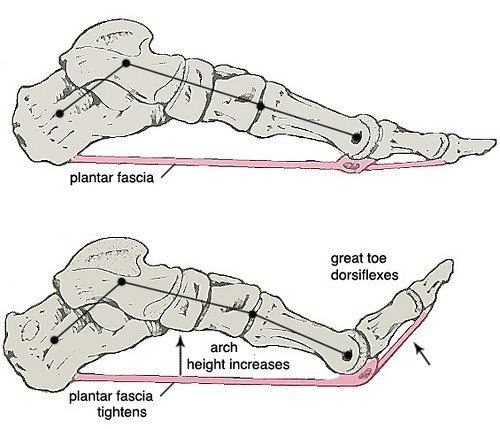
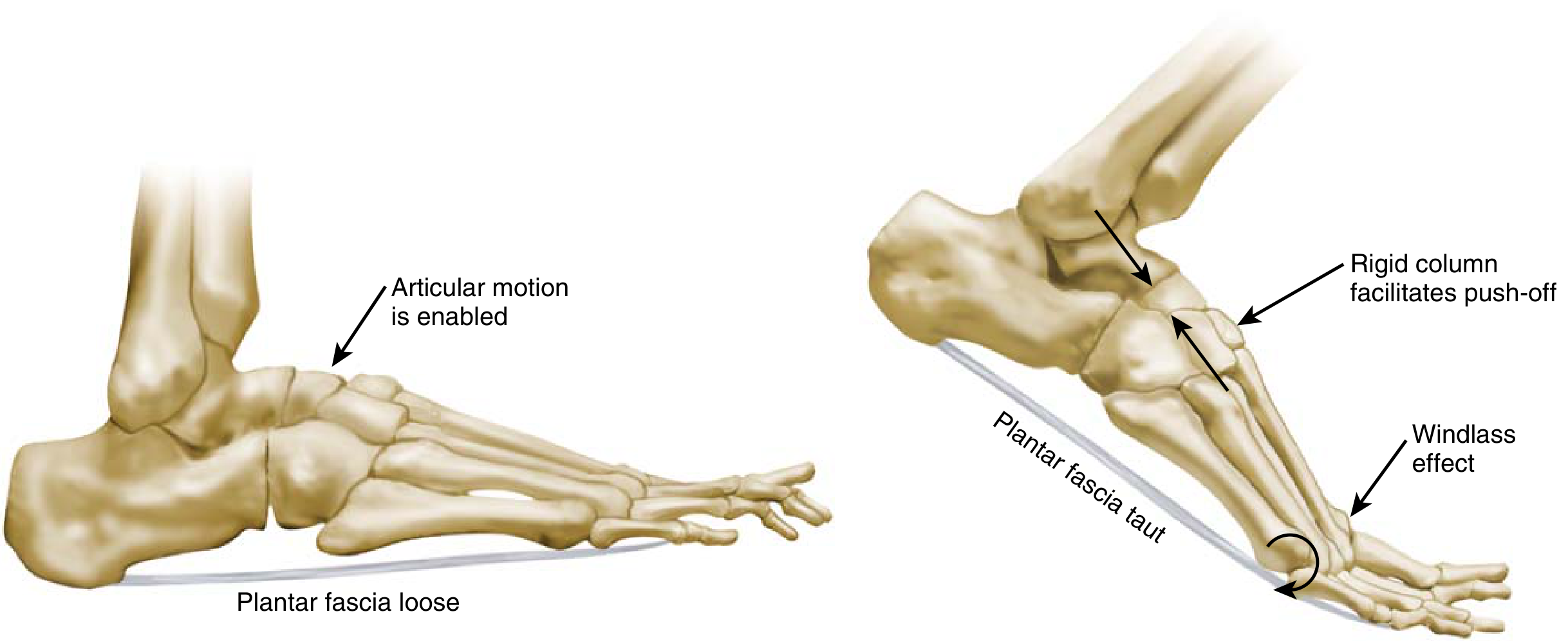
- Enables the windlass mechanism during push-off phase
The Windlass Mechanism
3. Etiology & Risk Factors
Plantar fasciitis is multifactorial in origin. It is best understood as an overuse injury from repetitive microtrauma, though it can also arise from a single traumatic event.
Intrinsic Risk Factors
| Factor | Mechanism |
|---|---|
| BMI >30 kg/m² | Biggest single risk factor - increases load on fascia |
| Pes planus (flat foot) | Increased strain at fascial origin due to arch collapse |
| Pes cavus (high arch) | Excessive heel strain; foot fails to absorb shock |
| Limited ankle dorsiflexion | Increases tension on plantar fascia during gait |
| Tight gastrocnemius-soleus complex | Alters biomechanics; contracture strongly associated |
| Excessive pronation or supination | Abnormal load distribution |
| Age 40-60 | Degenerative changes in collagen |
| Leg length discrepancy | Asymmetric loading |
Extrinsic Risk Factors
| Factor | Mechanism |
|---|---|
| Prolonged standing or walking | Repetitive cyclic loading |
| Sudden increase in activity/mileage | Classic overuse pattern in runners |
| Hard running surfaces | Reduced shock absorption |
| Improper or worn footwear | Inadequate arch support and cushioning |
| High heels | Chronic shortening of Achilles/plantar fascia |
| Occupation | Healthcare workers, teachers, factory workers |
Associated Systemic Conditions
- Spondyloarthritis (ankylosing spondylitis, psoriatic arthritis) - plantar fasciitis as an enthesopathy is a recognized feature
- Rheumatoid arthritis
- Diabetes mellitus
- Harrison's 22E; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Miller's Orthopaedics
4. Pathology & Pathophysiology
Mechanism of Injury
- Repetitive microtrauma at the calcaneal-fascial interface from cyclic loading
- Microtears at the origin of the plantar fascia on the medial calcaneal tuberosity
- Inadequate healing response initiates a degenerative injury-repair cycle
- Collagen fiber disorganization, mucoid degeneration, fibroblast proliferation (without true inflammatory infiltrate)
- Chronic degeneration of fascia fibers leads to thickening and hypoechogenicity of the fascia
- Loading of this degenerative tissue causes the characteristic plantar pain
- A traction osteophyte (calcaneal spur) may form as periostitis extends from the medial calcaneal tuberosity
Key Histological Finding
On biopsy: no inflammatory cells are present. Instead there is angiofibroblastic hyperplasia - hence the preferred modern term "plantar fasciosis" or "fasciopathy."
MRI Findings in Plantar Fasciitis
- Miller's Review of Orthopaedics 9th Ed.; Gray's Anatomy for Students; Family Medicine 9e
5. Signs & Symptoms
Classic Presentation
"First-step pain" is the pathognomonic symptom:
- Severe, sharp, stabbing pain on the plantar surface of the heel on taking the first few steps in the morning
- Pain is worst after prolonged inactivity (after sleep, after prolonged sitting)
- Pain characteristically improves with initial ambulation (as the fascia warms up and stretches)
- Pain returns and worsens later in the day after prolonged standing or walking
Pain Character
- Burning, aching, occasionally lancinating
- Located at the antero-medial heel (medial calcaneal tuberosity)
- May radiate proximally in severe cases
- Dull ache at end of day after extensive activity
Additional Features
- Stiffness in the foot and localized heel swelling
- Bilateral in a significant proportion of cases
- May coexist with posterior tibial tendon dysfunction (PTTD)
- A small subset has pain at the origin of abductor hallucis (ABH), suggesting involvement of the first branch of the lateral plantar nerve (Baxter's nerve)
What Plantar Fasciitis Does NOT Typically Cause
- Bruising, overt swelling
- Weakness or neurological signs
- Numbness or tingling (these suggest tarsal tunnel or nerve entrapment)
- Goldman-Cecil Medicine; Tintinalli's; Harrison's 22E; Miller's Orthopaedics
6. Clinical Examination & Tests
Inspection
- Foot posture: pes planus or pes cavus
- Gait assessment: antalgic gait, excessive pronation
- Calf bulk and symmetry
Palpation
The primary finding is exquisite, point tenderness over the antero-medial calcaneal tuberosity at the proximal insertion of the plantar fascia.
Pain is reproduced or worsened by:
- Passive dorsiflexion of the toes (stretches the fascia)
- Toe walking (loads the fascia)
- Passive dorsiflexion of the ankle
Special Clinical Tests
1. Windlass Test (Jack's Test)
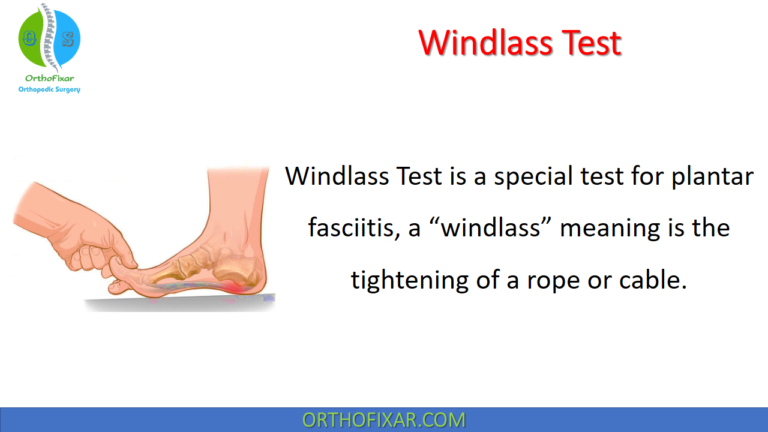
- Technique: With the patient non-weight-bearing (or weight-bearing for higher sensitivity), the examiner passively dorsiflexes the first metatarsophalangeal (MTP) joint
- Positive: Reproduction of pain at the medial calcaneal tuberosity
- Sensitivity: 13.6% (non-weight-bearing) to 31.8% (weight-bearing)
- Interpretation: A positive windlass test is highly specific for plantar fasciitis
2. Silfverskiöld Test
- Assesses for gastrocnemius contracture (a key associated finding)
- Ankle dorsiflexion assessed with knee extended vs. knee flexed
- Dorsiflexion improves significantly with knee flexion = isolated gastrocnemius tightness
- Important because gastrocnemius contracture strongly predicts plantar fasciitis and guides treatment (gastrocnemius recession)
3. First-Step Test
- Ask patient to take first steps after prolonged sitting or in the morning
- Classical "post-static dyskinesia" pattern is characteristic
4. Palpation along the Fascia
- Tenderness along the entire course suggests fascial tear or rupture
- Tenderness at the ABH origin suggests Baxter neuritis component
Differential Diagnosis Checklist
- Heel pad syndrome (diffuse tenderness, central not antero-medial)
- Stress fracture of the calcaneus
- Tarsal tunnel syndrome (burning/tingling, Tinel's sign positive)
- Baxter's neuritis (first branch lateral plantar nerve)
- Spondyloarthropathy-related enthesopathy
- Calcaneal tumors (rare)
- Miller's Orthopaedics; Roberts & Hedges'; Tintinalli's
7. Investigations
Plain Radiography (Weight-Bearing X-Ray)
- First-line investigation in all patients
- Goals: Rule out calcaneal stress fracture, subtalar arthritis, tumor, foreign body
- May show a plantar calcaneal heel spur (enthesophyte extending from medial calcaneal tuberosity)
- Important caveat: Heel spurs are found in ~15% of the general population; only 30% of those have heel pain. 75% of patients with heel pain have spurs. Spurs are therefore not diagnostic of plantar fasciitis
- The absence of a spur does not exclude the diagnosis
Ultrasound (US)
- Can demonstrate:
- Thickening of the plantar fascia at the calcaneal attachment (normal <4 mm; >4-5 mm is abnormal)
- Hypoechogenicity indicating edema at the fascial attachment
- Calcifications within the fascia
- Useful for guided injection therapy
- Accessible, dynamic, cost-effective
MRI
- Most sensitive method for detecting plantar fasciitis
- Shows: thickening of the plantar aponeurosis, perifascial edema/inflammation, associated calcaneal bone marrow edema
- Not required for routine diagnosis - reserved for atypical presentations or refractory cases
- Rules out occult fracture, nerve entrapment, soft tissue tumors
Nerve Conduction Studies / EMG
- Indicated when nerve entrapment (tarsal tunnel, Baxter neuritis) is suspected clinically
Blood Tests
- ESR, CRP, HLA-B27, uric acid if spondyloarthropathy or gout suspected
- Harrison's 22E; Goldman-Cecil; Roberts & Hedges'
8. Treatment
Treatment follows a stepwise, conservative-first approach. 90-95% of cases resolve within 12 months regardless of treatment modality.
Phase 1: First-Line Conservative Treatment (Weeks 1-6)
Activity Modification
- Reduce or eliminate the provocating activity (running, prolonged standing)
- Avoid barefoot walking, especially on hard floors in the morning
- Avoid flat shoes with no arch support
Stretching (Most Important Treatment)
Plantar fascia-specific stretching is the single most evidence-based conservative treatment:
1. Plantar Fascia-Specific Stretch
- Sit and cross the affected foot over the opposite knee
- Grasp the toes and pull them back toward the shin
- Hold 10 seconds, repeat 10 times, 3 times per day (especially before first steps in the morning)
2. Achilles/Gastrocnemius Stretch
- Stand facing a wall, step back with affected foot
- Keep heel on floor, lean forward until calf stretch is felt
- Hold 30 seconds, repeat 3x
3. Eccentric Calf Raises
- Rise onto toes (concentric), lower slowly past neutral (eccentric)
- Progressively load the fascia and tendon complex
Heel and Arch Support
- Cushioned heel inserts or heel cups
- Contoured full-length insoles for medial arch support
- Custom orthotics (from podiatry) for persistent cases
Ice/Cryotherapy
- Ice massage over the plantar heel 15-20 minutes, 2-3x daily
- Rolling foot over a frozen water bottle - stretches and ices simultaneously
NSAIDs
- Provide analgesia (not true anti-inflammatory effect, given the histology)
- Short course recommended
- Caution with GI, renal, cardiovascular risk factors
Taping
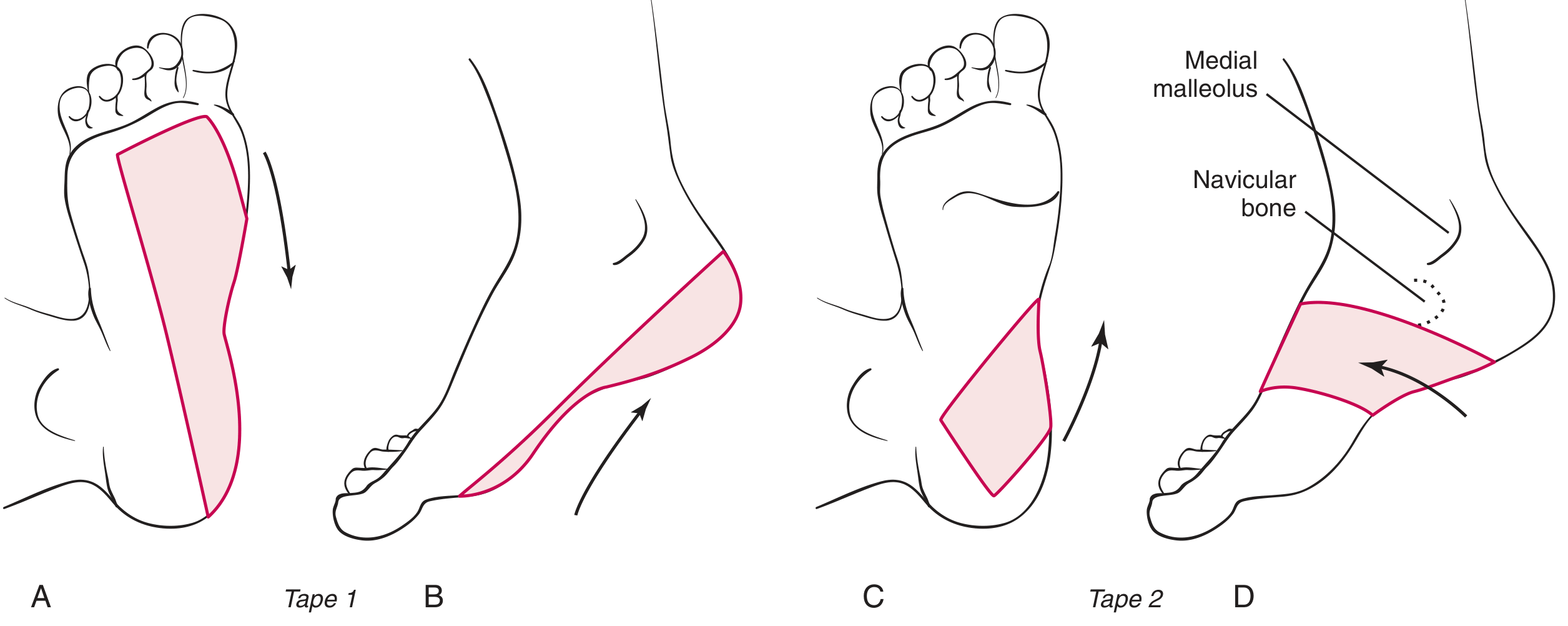
- Low-Dye strapping/taping provides immediate pain relief
- Applied with slight inversion and plantar flexion to offload the fascia
- Changed daily for 4-6 weeks
Phase 2: Intermediate Conservative Treatment (Weeks 6-12)
Night Splints
- Maintain ankle in neutral dorsiflexion (0°) during sleep
- Prevents nocturnal plantar flexion which causes re-tightening of fascia overnight
- Eliminates the "first-step" pain by pre-stretching the fascia
- A posterior lower-leg splint can be fabricated in the emergency department
- Custom dorsiflexion night splints from podiatry are more comfortable
Walking Boot/Cast
- Short-leg walking boot for severe or refractory cases
- Unloads and rests the plantar fascia
- Used for 4-6 weeks
Corticosteroid Injection
- Provides short-term pain relief (~1 month)
- Technique: 0.5-1 mL of methylprednisolone 40 mg/mL with local anaesthetic, injected at the medial calcaneal tuberosity (medial approach to avoid fat pad atrophy)
- Risks: Plantar fascia rupture (risk increases after 2-3 injections), plantar fat pad atrophy, chronic pressure pain
- Average number of injections leading to rupture: 2.67
- Should NOT be repeated more than 1-2 times; best reserved for resistant cases
Physical Therapy
- Manual therapy, soft tissue mobilization
- Therapeutic ultrasound
- Iontophoresis
- Gait retraining and biomechanical correction
Phase 3: Advanced Interventions (After 3-6 Months of Failed Conservative Therapy)
Extracorporeal Shock Wave Therapy (ESWT)
- Low-intensity ESWT has demonstrated success in limited studies
- Non-invasive; promotes tissue regeneration
- Mixed evidence but considered before surgery
Platelet-Rich Plasma (PRP) Injection
- Autologous PRP injected at fascial origin
- Growing evidence, particularly for chronic plantar fasciitis
- Some studies show superiority to corticosteroid at 3-6 months (more durable effect)
Prolotherapy / Autologous Blood Injection
- Injection of autologous blood or dextrose solution
- Investigational; limited consistent evidence
Botulinum Toxin Type A
- 50 units injected into plantar fascia reduced pain vs. placebo in one study
- Does not cure the disease
Phase 4: Surgical Treatment (After 6-12 Months of Failed Conservative Therapy, <5% of cases)
Indications: Failure of at least 6-12 months of comprehensive conservative management
Options:
-
Plantar fascia release (limited/partial - medial half): Most common; endoscopic or open
- Complete release risks: overloading the lateral column, dorsolateral foot pain, metatarsal stress fractures
- Limited release (medial half only) is preferred
-
Gastrocnemius recession: Strongly indicated in patients with a documented gastrocnemius contracture without evidence of Baxter neuritis; may be done in isolation
-
Baxter nerve decompression (release of deep fascia of ABH): For concurrent first branch lateral plantar nerve entrapment
- Miller's Review of Orthopaedics 9th Ed.; Goldman-Cecil Medicine; Harrison's 22E; Tintinalli's; Family Medicine 9e; Roberts & Hedges'
9. Rehabilitation Protocol
Rehabilitation is the cornerstone of management and should be structured in phases:
Phase 1: Acute Phase (Weeks 1-4) - Pain Control & Load Management
Goals: Reduce pain, protect the fascia, maintain fitness
| Intervention | Detail |
|---|---|
| Activity modification | Reduce running/standing; switch to swimming or cycling |
| Ice massage | 15-20 min, 2-3x daily |
| NSAID (short course) | Analgesia |
| Plantar fascia stretching | 3x10 reps before first steps, morning and evening |
| Achilles stretching | Gastrocnemius and soleus stretches |
| Taping | Low-Dye or kinesio taping during the day |
| Night splint | Worn during sleep to prevent nocturnal tightening |
| Heel cushion/insole | Immediate shock absorption |
Phase 2: Subacute Phase (Weeks 4-8) - Restore Tissue Tolerance
Goals: Progressively load the fascia, address biomechanical deficits
| Intervention | Detail |
|---|---|
| Eccentric calf raises | Start bilateral, progress to single-leg; 3 sets x 15 reps |
| Intrinsic foot muscle strengthening | Towel scrunches, marble pickups, short foot exercise |
| Ankle dorsiflexion mobilization | Joint mobilisation if range is restricted |
| Progressive weight-bearing activity | Begin walking on soft surfaces |
| Orthotic assessment | Custom orthotics if foot malalignment is present |
| Manual therapy | Soft tissue massage, joint mobilisation |
Phase 3: Strengthening & Functional Phase (Weeks 8-16)
Goals: Build strength, correct movement patterns, return to sport/work
| Intervention | Detail |
|---|---|
| Single-leg calf raises (eccentric focus) | 3 sets x 15, progress to weighted |
| Pronator/supinator strengthening | Theraband exercises in all planes |
| Hip and knee strengthening | Glute med, hip abductors (compensatory loading) |
| Balance and proprioception | Single-leg stance, BOSU board |
| Gait retraining | Address overpronation, stride length, cadence |
| Step-down exercise | Addresses shock absorption in the kinetic chain |
Phase 4: Return to Sport/Activity (Weeks 12-20+)
Goals: Full return to previous activity level
| Intervention | Detail |
|---|---|
| Progressive running program | Walk-run intervals on soft surface; 10% weekly mileage increase max |
| Plyometric loading | Jump and landing mechanics |
| Sport-specific drills | Gradually reintroduce sport-specific movements |
| Footwear advice | Replace worn running shoes; avoid barefoot on hard floors |
| Maintenance stretching | Continue plantar fascia and Achilles stretching indefinitely |
Key Stretching Exercises (Summary)
- Plantar fascia self-stretch - most evidence-based single exercise
- Gastrocnemius wall stretch - knee straight, 30s holds
- Soleus stretch - knee bent, 30s holds
- Frozen bottle rolling - simultaneous stretching and cryotherapy
- Towel/belt toe stretch - seated, towel looped around toes pulled toward shin
- Short foot exercise - intrinsic muscle activation
Physiotherapy Modalities
| Modality | Evidence |
|---|---|
| Stretching (fascia + Achilles) | Strong - cornerstone of management |
| Night splints | Moderate - reduces first-step pain significantly |
| Orthotics (custom or prefabricated) | Moderate - especially with pes planus/cavus |
| ESWT (shock wave) | Moderate - for chronic refractory cases |
| Ultrasound therapy | Limited - adjunct only |
| Iontophoresis (dexamethasone) | Limited evidence |
| Kinesio taping | Limited - short-term pain relief |
10. Prognosis
- 80-95% of cases resolve within 12 months with conservative management, regardless of the specific treatment offered
- Resolution can take 6-18 months in some cases - patients must be counseled about the prolonged natural history
- Recurrence is common if underlying biomechanical factors are not corrected
- <5% require surgical intervention
- Early intervention with appropriate rehabilitation breaks the pain-deconditioning cycle
Summary Table
| Domain | Key Points |
|---|---|
| Pathology | Degenerative fasciopathy (not true inflammation); microtears at medial calcaneal tuberosity; collagen disorganization |
| Biggest risk factor | BMI >30; also tight gastrocnemius, pes planus/cavus, prolonged standing |
| Classic symptom | First-step pain in morning; improves with walking; worsens with prolonged activity |
| Key sign | Point tenderness at antero-medial calcaneal tuberosity |
| Clinical test | Windlass test (passive 1st MTP dorsiflexion) |
| Investigations | Weight-bearing X-ray (first line); US (thickened fascia); MRI (if atypical) |
| First-line treatment | Fascia-specific stretching + Achilles stretching + heel cushion + NSAIDs |
| Injection | Corticosteroid (short-term benefit, rupture risk); PRP (more durable) |
| Surgery | Limited plantar fascial release (medial half); gastrocnemius recession; <5% need it |
| Prognosis | 90-95% resolve within 12 months |
Sources: Miller's Review of Orthopaedics 9th Ed. | Harrison's Principles of Internal Medicine 22E | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine | Textbook of Family Medicine 9e | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Gray's Anatomy for Students | Pfenninger & Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.