Approach to occult GI bleed
Reading File
Finding Sources
Finding Sources
Searching PubMed
"occult gastrointestinal bleeding"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Approach to Occult GI Bleeding
Definitions - Clarifying the Terminology
Understanding the terminology avoids confusion in clinical practice:
-
Occult GI bleeding - subacute bleeding that is not clinically visible. It presents as either a positive fecal occult blood test (FOBT) or iron deficiency anemia (IDA), with no hematemesis, melena, or hematochezia. - Sleisenger & Fordtran's Gastrointestinal and Liver Disease
-
Obscure GI bleeding - bleeding from a site that is not apparent after routine endoscopic evaluation (EGD + colonoscopy +/- push enteroscopy). Obscure bleeding can itself be either overt (visible blood) or occult (positive FOBT/IDA). - Goldman-Cecil Medicine
-
Prevalence context: ~10% of all GI bleeding hospitalizations are from the small bowel (obscure). Of these, 75% originate beyond the reach of a standard endoscope. Iron deficiency has a prevalence of 2-5% among adult men and postmenopausal women, and GI loss is a leading cause.
Common Causes
Within reach of standard endoscopy (missed initially)
- Cameron ulcers (large hiatal hernia)
- Dieulafoy lesion (aberrant submucosal vessel without ulcer)
- Internal hemorrhoids
- Gastric antral vascular ectasia (GAVE)
- Peptic ulcer disease / H. pylori
Small bowel causes (most common when standard endoscopy is negative)
| Lesion | Frequency |
|---|---|
| No lesion found | ~40% |
| Angiectasias (angiodysplasia) | ~31% (most common identifiable lesion) |
| Ulcerations | ~13% |
| Malignancy | ~8% |
| Other | ~6% |
Source: Double-balloon enteroscopy data in 488 patients - Goldman-Cecil Medicine, Table 121-5
- Other small bowel causes: NSAID enteropathy, Crohn's disease, celiac disease, radiation enteritis, Meckel's diverticulum, hereditary hemorrhagic telangiectasia (HHT/Osler-Weber-Rendu)
Causes of iron deficiency anemia without GI blood loss
- Celiac disease (malabsorption)
- Atrophic gastritis (decreased absorption)
- Hemolysis
- Menorrhagia (premenopausal women)
Step-by-Step Diagnostic Approach
Step 1 - Initial Assessment
History clues:
- Medication history: NSAIDs, aspirin, anticoagulants, steroids
- Prior GI surgeries
- Family history of GI cancer or polyposis
- Skin/mucosal telangiectasias (HHT)
- Symptoms of malabsorption (celiac)
- Menstrual history in premenopausal women
Labs:
- CBC (microcytic anemia, low Hb)
- Iron studies: serum ferritin (low), transferrin saturation (low), TIBC (elevated)
- CRP/ESR (if inflammatory cause suspected)
- Celiac serology (anti-tTG IgA)
- Reticulocyte count
Who warrants GI evaluation for IDA?
- All adult men, regardless of age
- All postmenopausal women
- Premenopausal women only after excluding menorrhagia and other non-GI causes
Step 2 - FOBT-Positive vs. IDA: Different Starting Points
FOBT-positive patient:
- Colonoscopy is the first step, because FOBT was designed to screen for colorectal cancer (begin at age 45 in average-risk adults per Harrison's)
- If colonoscopy is negative and no IDA/symptoms: no further workup needed per Harrison's
- If IDA or GI symptoms present: proceed to upper endoscopy
IDA patient:
- Colonoscopy first (most common source is colorectal lesion)
- Then upper endoscopy + push enteroscopy if colonoscopy is negative
- Take duodenal biopsies during upper endoscopy to exclude celiac disease
- Treat H. pylori if detected (reduces iron absorption and causes microerosions)
Step 3 - When Standard Endoscopy is Negative (Obscure-Occult)
This is the challenging clinical scenario. The algorithm below (from Goldman-Cecil Medicine) guides management:
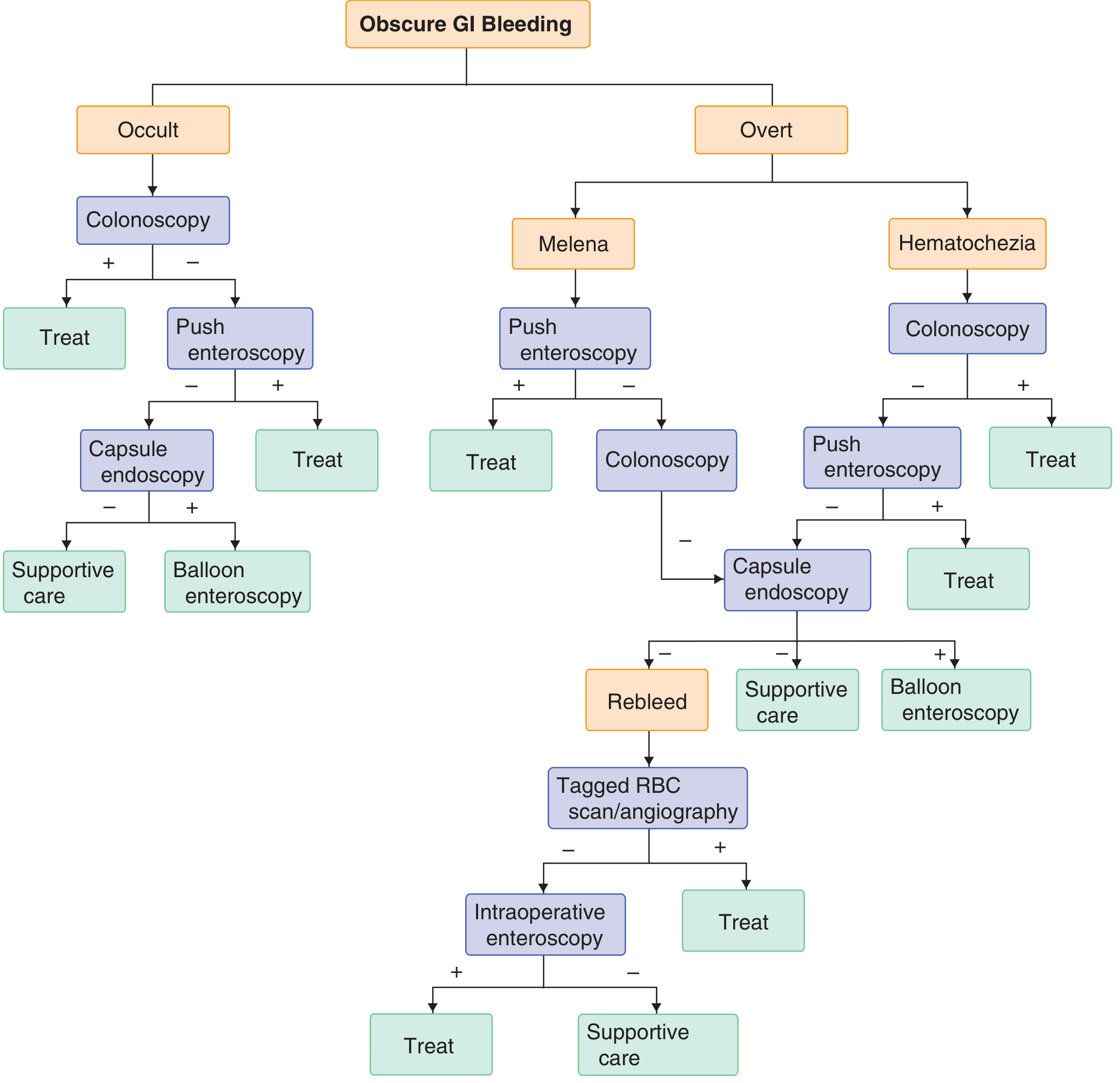
Occult bleeding pathway (left side of algorithm):
- Colonoscopy - if positive: treat. If negative:
- Push enteroscopy - examines proximal small bowel to ~70 cm past ligament of Treitz. If positive: treat. If negative:
- Capsule endoscopy (CE) - the key diagnostic tool for small bowel visualization. If positive: proceed to balloon enteroscopy. If negative: supportive care (no aggressive further workup)
Step 4 - Capsule Endoscopy
- The pivotal investigation once standard endoscopy is unrevealing
- Visualizes the entire small bowel mucosa non-invasively
- Most useful for angiodysplasia, mucosal inflammation, and small tumors
- Yield higher when performed within 2 weeks of acute bleed (while lesion is still active)
- Contraindications: known or suspected bowel obstruction, strictures, swallowing disorder
- After positive capsule: proceed to device-assisted (double-balloon/single-balloon/spiral) enteroscopy for therapeutic intervention
Step 5 - Deep Enteroscopy (Device-Assisted)
- Double-balloon enteroscopy (DBE) is most common - uses balloon overtube to advance deep into small bowel (>300 cm)
- Can be performed antegrade (per os) or retrograde (per anum)
- Allows both diagnosis and therapy (hemostasis, polypectomy, tattooing)
- Intraoperative enteroscopy reserved for cases where all other modalities fail
Step 6 - Imaging Modalities
CT Enterography (CTE):
- Multiphasic contrast-enhanced protocol with neutral oral contrast
- One study showed CTE sensitivity 88% vs. capsule endoscopy 38% for identifying small bowel lesions - particularly superior for focal small intestinal tumors (Grainger & Allison)
- Complementary to capsule endoscopy for benign causes (angiodysplasia, inflammation)
- Best combined with CE in clinical practice
CT Angiography (CTA):
- More useful in overt/active bleeding (detects extravasation ≥0.3-0.5 mL/min)
- Less useful in occult/low-grade bleeding (may miss intermittent bleeders)
Tagged RBC Scintigraphy:
- Detects bleeding rates as low as 0.1 mL/min
- Used mainly in overt obscure bleeding with rebleed after negative capsule
- Poor anatomic localization - usually followed by angiography
Step 7 - Angiography and Surgery
- Selective mesenteric angiography: therapeutic (embolization) and diagnostic; requires active bleeding at time of study
- Intraoperative enteroscopy: last resort when all other modalities fail; combined surgical and endoscopic approach
Special Considerations
When to re-scope before going to capsule endoscopy
- Before labeling bleeding as "obscure," repeat upper endoscopy and colonoscopy, as studies show a lesion is found in up to 25% of cases on repeat examination (missed Dieulafoy, Cameron ulcers, hemorrhoids, GAVE)
H. pylori and iron deficiency
- H. pylori decreases iron absorption and can cause microerosions
- Treat if positive even without obvious ulcer - this alone may resolve IDA in some patients
Celiac disease
- Always biopsy duodenum during upper endoscopy in IDA workup - celiac is a common, easily missed cause of IDA
HHT (Hereditary Hemorrhagic Telangiectasia)
- Autosomal dominant
- Look for telangiectasias on lips, buccal mucosa, tongue, fingernails
- Small bowel AVMs are a major source of recurrent occult bleeding
Medications causing occult blood loss
- NSAIDs: #1 cause of small bowel ulcers/erosions
- Aspirin: gastric erosions
- Anticoagulants/antiplatelets: unmask underlying lesions
Summary Algorithm - Occult GI Bleed
Positive FOBT or IDA
|
Initial labs (iron studies, celiac serology)
|
+----|----+
| |
FOBT+ IDA
| |
Colonoscopy Colonoscopy first
| |
Negative Negative
| |
If IDA/Sx → EGD + push enteroscopy
|
Negative
|
Duodenal biopsy (celiac), treat H. pylori if +
|
Still negative
|
Capsule endoscopy
/ \
Positive Negative
| |
Balloon Supportive
enteroscopy care
(diagnose + (reassess)
treat)
Sources:
- Goldman-Cecil Medicine International Edition - Chapter 121: Obscure and Occult GI Bleeding
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease - Chapter 20: GI Bleeding
- Grainger & Allison's Diagnostic Radiology - Chapter 21: Occult GI Bleeding
- Harrison's Principles of Internal Medicine (22E, 2025) - Positive FOBT
ECT in psychiatry
Reading File
Finding Sources
Searching PubMed
"electroconvulsive therapy"[MeSH Terms] AND depression
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content across the key domains. I have enough to write a thorough, well-structured answer. Let me compile it now.
Electroconvulsive Therapy (ECT) in Psychiatry
1. Historical Background
ECT has the longest pedigree of any modern psychiatric treatment. Key milestones:
| Year | Milestone |
|---|---|
| 1500s | Paracelsus induces seizures with camphor to treat psychiatric illness |
| 1934 | Ladislas von Meduna successfully treats a catatonic patient with chemically induced seizures (camphor/pentylenetrazol), based on his hypothesis of biologic antagonism between epilepsy and schizophrenia |
| 1938 | Ugo Cerletti and Lucio Bini (Italy) administer the first electrical ECT to a delusional incoherent patient - he remitted after 11 treatments |
| 1940s | ECT introduced to the United States; curare used as muscle relaxant |
| 1951 | Succinylcholine introduced, enabling modified (paralytic) ECT |
| 1960s | Randomized controlled trials confirm ECT superior to medications for depression |
| 1987 | Sackeim et al. demonstrate dose-response relationship; seizure threshold matters, not just seizure duration |
| 2000 | High-dose right unilateral ECT = bilateral ECT in efficacy, with fewer cognitive side effects |
| 2001 | Largest trial of post-ECT relapse prevention shows nortriptyline + lithium superior to either alone |
Source: Kaplan & Sadock's Synopsis of Psychiatry, Table 22-1
An estimated ~100,000 patients/year receive ECT in the United States. Despite declining use since mid-20th century, ECT remains the most effective acute treatment for major depression and is irreplaceable for life-threatening psychiatric emergencies.
2. Mechanism of Action
The mechanism of ECT is not fully established, but several neurobiological effects are understood:
Seizure physiology
- A bilateral generalized seizure is necessary for both therapeutic and adverse effects of ECT
- Subconvulsive stimulation is ineffective; the seizure is necessary but not sufficient - its dose relative to seizure threshold also matters
- ECT acts as an anticonvulsant - seizure threshold rises progressively across a treatment course
Neurophysiology
- During seizure: cerebral blood flow, O2 and glucose utilization, and blood-brain barrier permeability increase
- Post-ictally: blood flow and glucose metabolism decrease (most markedly in frontal lobes); the degree of decrease correlates with therapeutic response
- After a successful course: EEG shows massive increase in slow-wave activity over prefrontal cortex in responders; high-intensity bilateral stimulation produces the strongest effect
- EEG typically returns to pretreatment baseline 1 month to 1 year after course completion
Neurotransmitter/receptor changes
- Downregulation of postsynaptic beta-adrenergic receptors (similar to chronic antidepressants, but ECT achieves this faster)
- Enhanced serotonergic transmission (5-HT1A receptor sensitization)
- Increased dopaminergic activity in mesolimbic pathways
- Elevated GABA and endogenous opioid levels
- Increased BDNF (brain-derived neurotrophic factor) - possible contribution to neuroplasticity and antidepressant effect
- Neuroendocrine changes: affects HPA axis, prolactin, thyroid-stimulating hormone
3. Indications
Primary (First-line) Indications
ECT is the first-line treatment (not reserved for treatment failure) when speed of response is critical:
- Severe depression with high suicidal risk - ECT works in days vs. weeks for antidepressants
- Depression with refusal of food/fluid (nutritional emergency - "life-threatening inanition")
- Catatonia - most dramatic and rapid response; can take as few as 1-4 treatments
- Severe depression in pregnancy - safe in all trimesters when medications are hazardous
- Neuroleptic Malignant Syndrome (NMS) - when pharmacotherapy fails
Secondary (After Medication Failure) Indications
- Major depressive disorder (MDD) - treatment-resistant (failed 2+ adequate antidepressant trials)
- Bipolar depression - treatment-resistant
- Mania - severe/refractory; comparable to lithium in RCTs (equal response rates in 1988 trials); requires 8-20 treatments
- Schizophrenia - as adjunct in treatment-resistant cases or acute exacerbations; 15+ treatments often needed
- Schizoaffective disorder - particularly when affective component is prominent
- Parkinson's disease with depression or "on-off" motor fluctuations - ECT has direct dopaminergic effects
Predictors of Good Response to ECT
- Severe melancholic depression
- Psychotic depression (delusional depression responds exceptionally well)
- Catatonic features
- Prior positive response to ECT
- Shorter duration of current episode
Predictors of Poor Response
- Concurrent personality disorder
- Atypical depression
- Long duration of illness
- High levels of anxiety/somatization
4. Contraindications
There are no absolute contraindications to ECT. Risk-benefit assessment guides decision-making. However, the following are relative contraindications (require special precautions):
| Condition | Reason/Risk |
|---|---|
| Recent MI (<3 months) | ECT causes transient hypertension and tachycardia; cardiac stress |
| Raised intracranial pressure / space-occupying lesion | Risk of cerebral herniation due to seizure-induced ICP rise |
| Recent intracranial surgery / stroke | Unstable cerebrovascular status |
| Aortic/cerebral aneurysm | Risk of rupture with hypertensive surge |
| Retinal detachment | Increase in IOP during seizure |
| Pheochromocytoma | Uncontrolled catecholamine release |
| Anesthesia risk (ASA Class 4-5) | General anesthesia required |
Pregnancy is NOT a contraindication - ECT is often safer than medications in pregnancy.
5. Pre-ECT Evaluation
Workup
- CBC, serum electrolytes, urinalysis, LFTs
- ECG (to assess cardiac risk from stimulation-induced autonomic surges)
- Thorough medical history and physical examination
- Anesthesia evaluation
Note: Spinal X-rays are no longer routinely indicated (succinylcholine-modified ECT has very low spinal injury risk).
Medications to consider before ECT
- Stop or reduce: benzodiazepines (raise seizure threshold), anticonvulsants (raise seizure threshold, reduce efficacy), lithium (increases risk of post-ECT confusion and prolonged seizures)
- Continue: antihypertensives, cardiac medications, antireflux medications
- Anticholinergics (atropine/glycopyrrolate): may be given pre-procedure to reduce secretions and prevent bradycardia
6. Technique and Administration
Anesthesia Protocol
ECT is performed under general anesthesia with 3 components:
- Anticholinergic premedication - atropine or glycopyrrolate (reduces secretions, prevents bradycardia)
- Short-acting general anesthetic - methohexital (preferred) or propofol - for rapid induction and short duration
- Succinylcholine (depolarizing neuromuscular blocker) - to minimize motor convulsions and prevent musculoskeletal injury. A blood pressure cuff can be inflated on one arm prior to succinylcholine to observe the motor seizure in that limb.
The patient is oxygenated before and after the seizure. Vital signs and pulse oximetry are monitored throughout.
Electrode Placement
Three configurations are used:
| Placement | Description | Efficacy | Cognitive SE |
|---|---|---|---|
| Bilateral (bitemporal) | One electrode over each temporal area | Highest | Most |
| Right unilateral (RUL) | Both electrodes on right side (d'Elia position) | High at high dose | Least |
| Bifrontal | Both electrodes over frontal areas | Similar to bilateral | Intermediate |
- High-dose right unilateral ECT (≥6x seizure threshold) achieves equivalent response to bilateral ECT with significantly less cognitive impairment
- Bilateral ECT is preferred in urgent/severe presentations requiring fastest response
- Ultra-brief pulse width bilateral ECT is likely ineffective
Stimulus Parameters
- Modern ECT machines deliver brief pulse (not sine wave) current
- Stimulus measured in millicoulombs (mC) or joules
- Key principle: dose-response relationship - stimulus must be substantially above seizure threshold for right unilateral ECT; for bilateral, even moderately suprathreshold doses are effective
- ~20% of applied charge actually enters the skull to excite neurons (skull impedance is high)
Monitoring the Seizure
- Minimum effective seizure duration: 25 seconds (EEG-monitored)
- EEG monitoring is mandatory; at minimum, electrodes over contralateral hemisphere for unilateral ECT
- Seizure phases: tonic (10-20 sec, plantar extension) → clonic (rhythmic contractions) → postictal suppression (60-90 sec)
- If seizure duration < 25 sec or no seizure: increase stimulus by 25-100%, check electrode contact, consider caffeine sodium benzoate (500-2000 mg IV) to lower seizure threshold
Number and Frequency of Treatments
| Condition | Number of Treatments | Frequency |
|---|---|---|
| Major depression | 6-12 (up to 20) | 2-3x/week |
| Mania | 8-20 | 2-3x/week |
| Schizophrenia | 15+ | 2-3x/week |
| Catatonia/Delirium | 1-4 | Daily possible |
- Twice-weekly is associated with less memory impairment than three-times-weekly
- Treatment continues until maximal therapeutic response is reached (defined as failure to improve after 2 consecutive sessions)
- If no improvement after 6-10 sessions: switch to bilateral placement and high-density stimulation before abandoning ECT
7. Adverse Effects
Cognitive Effects (Most Clinically Significant)
- Acute confusion/disorientation - common immediately post-ictal; resolves within 30-60 minutes
- Anterograde amnesia - difficulty forming new memories during the treatment course; typically transient
- Retrograde amnesia - loss of memories from weeks to months surrounding the ECT course; the most persistent side effect
- Autobiographical memory most affected
- Usually resolves within weeks-months but can occasionally persist
- Right unilateral ECT causes significantly less retrograde amnesia than bilateral
- A 2024 meta-analysis (PMID 38101070) found that while ECT causes short-term cognitive impairment, most domains recover at follow-up; autobiographical memory most persistently affected
Cardiovascular Effects
- Immediate bradycardia/asystole (parasympathetic surge with stimulus application) - prevented by anticholinergic premedication
- Followed by tachycardia and hypertension (sympathetic surge from seizure) - typically brief and self-limiting
- ECG changes (ST changes, ectopy) can occur; monitor closely in cardiac patients
- Deaths from ECT are extremely rare: ~1/10,000 treatments (comparable to anesthesia mortality)
Other Adverse Effects
- Headache - most common post-procedure complaint; treat with analgesics
- Muscle aches - from succinylcholine (fasciculations)
- Nausea/vomiting - anesthesia-related; treat with antiemetics
- Prolonged seizure / Status epilepticus (seizure >180 sec) - terminate with IV diazepam 5-10 mg or additional barbiturate anesthetic; requires intubation
- Tardive seizures - spontaneous seizures appearing after ECT, especially in those with pre-existing epilepsy
- Hypomania/mania switch - can occur during ECT for depression, especially in bipolar patients
- Dental/jaw injury - bite block is used to protect teeth
8. Continuation and Maintenance ECT
After a successful acute course, relapse rates without treatment are high (50-80% within 6 months).
Strategies
- Continuation pharmacotherapy - the 2001 CORE trial demonstrated that nortriptyline + lithium is significantly superior to nortriptyline alone or placebo for 6-month relapse prevention post-ECT
- Continuation ECT (C-ECT) - weekly then biweekly treatments for 6 months
- Maintenance ECT (M-ECT) - monthly treatments for patients who relapse despite medications, cannot tolerate medications, or prefer ECT
9. ECT vs. Ketamine (Recent Evidence)
Two landmark meta-analyses in JAMA Psychiatry directly compared ECT and ketamine for major depressive episodes:
- Rhee et al. (2022) [PMID 36260324] and Menon et al. (2023) [PMID 37043224] - both concluded ECT demonstrated superior or comparable antidepressant efficacy to ketamine overall, but ketamine had faster onset of action and fewer cognitive side effects. ECT remains the more definitively evidence-based option for severe/treatment-resistant depression.
10. Special Populations
| Population | Consideration |
|---|---|
| Pregnancy | ECT is safe in all trimesters; often preferred over medications for severe depression/mania |
| Elderly | Higher response rate than younger adults; need careful anesthesia titration; more cognitive vulnerability |
| Children/adolescents | Rare; reserved for severe, refractory, life-threatening cases |
| With implanted VNS | Turn off VNS generator during ECT (its anticonvulsant effect will reduce efficacy) |
| Parkinson's disease | Direct dopaminergic benefit beyond antidepressant effect |
| Dementia | Use cautiously; increased risk of prolonged confusion, but catatonia and severe depression in dementia can be treated |
11. Summary Table
| Feature | Details |
|---|---|
| Mechanism | Generalized tonic-clonic seizure + neurohumoral changes |
| Minimum seizure duration | 25 seconds |
| Frequency | 2-3x/week |
| Course length (depression) | 6-12 sessions |
| Response rate (depression) | 60-80%; higher in psychotic depression |
| Fastest response for | Catatonia (1-4 sessions) |
| Most cognitive SE | Bilateral bitemporal placement |
| Least cognitive SE | Right unilateral high-dose |
| Anesthetic | Methohexital + succinylcholine |
| Relapse prevention | Nortriptyline + lithium (best evidence) |
| Only absolute CI | None |
Sources:
- Kaplan & Sadock's Synopsis of Psychiatry - Chapter 22: ECT and Other Brain Stimulation Therapies (primary source)
- Rhee TG et al., JAMA Psychiatry 2022 [PMID 36260324] - Ketamine vs ECT meta-analysis
- Menon V et al., JAMA Psychiatry 2023 [PMID 37043224] - Ketamine vs ECT meta-analysis
- Guo Q et al., Psychiatry Res 2024 [PMID 38101070] - Long-term cognitive effects of ECT
This is a shared conversation. Sign in to Orris to start your own chat.