Parkinson disease mbbs 1st year student
Reading File
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND pathophysiology
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple textbooks. Let me compile a thorough, well-structured MBBS 1st year guide on Parkinson's disease.
Parkinson's Disease - MBBS 1st Year Guide
Sources: Lippincott Illustrated Reviews: Pharmacology, Neuroanatomy through Clinical Cases 3e, Costanzo Physiology 7e, Bradley & Daroff's Neurology in Clinical Practice
1. Definition & Overview
Parkinson's disease (PD) is a progressive neurodegenerative disorder caused by the loss of dopaminergic neurons in the substantia nigra pars compacta, leading to dopamine depletion in the striatum. It was first described by James Parkinson in 1817 in his "Essay on the Shaking Palsy."
- Onset typically between 55-65 years of age
- It is the second most common neurodegenerative disorder after Alzheimer's disease
2. Anatomy & Neurotransmitter Basis
The Nigrostriatal Pathway
The substantia nigra is part of the extrapyramidal system (basal ganglia). It has two key parts:
- Pars compacta - contains pigmented dopaminergic neurons (site of degeneration in PD)
- Pars reticulata - inhibitory output nucleus
Normal circuit:
- Substantia nigra pars compacta sends dopaminergic (inhibitory) projections to the neostriatum
- Neostriatum sends GABAergic (inhibitory) neurons back to the substantia nigra
- This mutual inhibitory circuit normally maintains balanced motor control
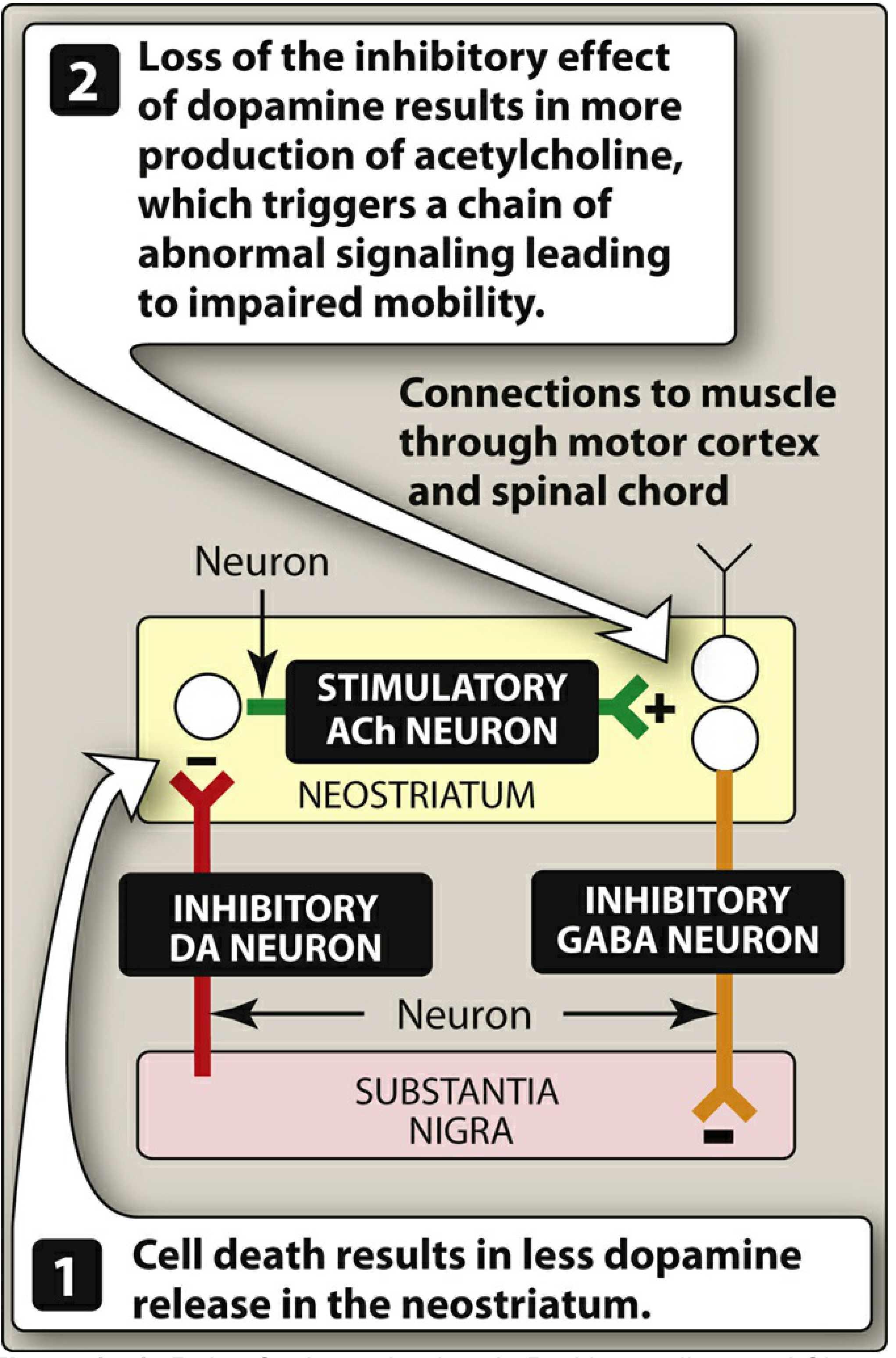
In PD:
- Dopaminergic neurons in the substantia nigra degenerate and die
- Dopamine levels in the neostriatum fall
- The normal inhibitory effect of dopamine on cholinergic (ACh) neurons is lost
- Cholinergic neurons become relatively overactive (ACh > DA imbalance)
- This abnormal signaling disrupts the motor control circuit → motor symptoms
Key concept: PD = DA deficiency + relative ACh excess in the neostriatum.
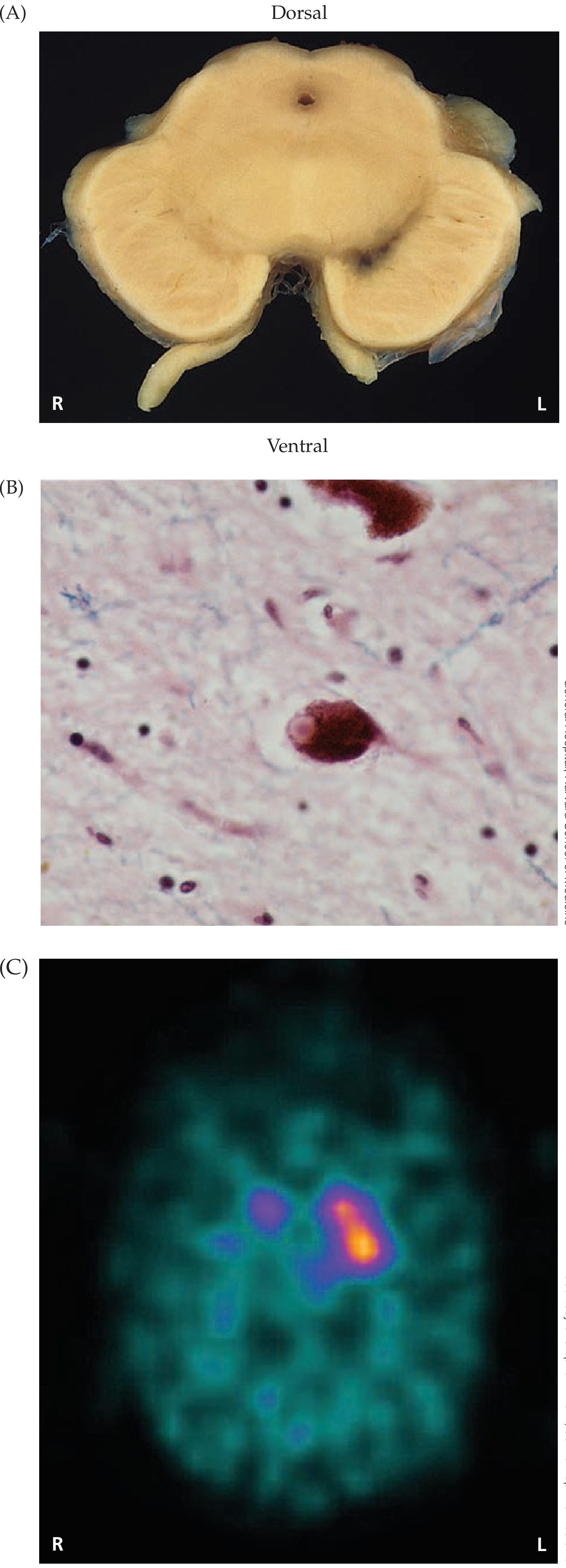
3. Pathology (What You See Under the Microscope)
Gross Pathology
- Pallor/depigmentation of the substantia nigra (normal black pigment from neuromelanin is lost due to neuronal death)
Microscopic Pathology - Lewy Bodies (PATHOGNOMONIC)
- Lewy bodies are intracytoplasmic, eosinophilic (pink) inclusions with a dense center and a lighter surrounding halo, found in remaining dopaminergic neurons
- Composed mainly of alpha-synuclein protein
- This is the hallmark lesion of Parkinson's disease
4. Etiology
- Idiopathic in most cases (cause unknown)
- Genetic factors: Mutations in LRRK2, SNCA (alpha-synuclein), PARK genes
- Environmental: MPTP (a neurotoxin), pesticides (rotenone, paraquat)
- Secondary (Drug-induced) Parkinsonism: Antipsychotics (haloperidol, phenothiazines) - block dopamine receptors; called pseudoparkinsonism
5. Clinical Features - "TRAP"
The classic motor tetrad is remembered as TRAP:
| Feature | Description |
|---|---|
| T - Tremor | Resting "pill-rolling" tremor (4-6 Hz); worse at rest, improves with movement |
| R - Rigidity | Cogwheel rigidity (intermittent) or lead-pipe rigidity; present throughout range of motion |
| A - Akinesia/Bradykinesia | Slowness of movement; difficulty initiating movement |
| P - Postural instability | Impaired balance reflexes; shuffling gait; falls |
Additional Motor Signs
- Masked facies (hypomimia) - reduced facial expression, decreased blink rate
- Micrographia - small handwriting
- Festinating gait - short, shuffling steps, appears to be "chasing their center of gravity"
- Freezing - difficulty initiating gait
- Hypophonia - soft, monotonous voice
- Myerson's sign - inability to suppress blinking when the glabella is tapped repeatedly
- Stooped posture with flexion of neck and trunk
- En bloc turning - turns without normal torso rotation
Non-Motor Symptoms (equally important!)
- Depression - most common psychiatric disturbance in PD; may predate motor symptoms
- Dementia (late feature; 15-40% of patients)
- Visual hallucinations (up to 40% of patients, often medication-induced)
- Autonomic dysfunction: constipation, orthostatic hypotension, bladder dysfunction
- Sleep disturbances: REM sleep behavior disorder (early marker)
- Anosmia (loss of smell - often a very early symptom)
- Dysphagia (swallowing difficulty, increases aspiration risk)
6. Basal Ganglia Pathways - Direct vs. Indirect
Costanzo Physiology explains the two pathways:
| Pathway | Effect on Movement | In PD |
|---|---|---|
| Direct pathway (Cortex → Striatum → GPi → Thalamus → Cortex) | Facilitates (excites) movement | Reduced (less DA to activate it) |
| Indirect pathway (Cortex → Striatum → GPe → STN → GPi → Thalamus) | Inhibits movement | Increased activity |
Net result in PD: More inhibition from the globus pallidus interna → thalamus is overly suppressed → motor cortex is not adequately excited → hypokinesia (reduced movement).
7. Diagnosis
PD is a clinical diagnosis based on:
- Cardinal features (TRAP)
- Asymmetrical onset (usually one side first)
- Response to levodopa
Investigations:
- No definitive blood test
- DaT SPECT scan (dopamine transporter imaging) - shows reduced dopamine uptake in the striatum
- MRI brain - usually normal in idiopathic PD (used to rule out other causes)
Red flags that suggest it is NOT idiopathic PD:
- Early postural instability
- Symmetrical onset
- Rapid progression
- No response to levodopa
8. Treatment - Pharmacology
Goal: Restore the DA/ACh balance in the neostriatum. Drugs are symptomatic; none reverse neurodegeneration.
A. Levodopa + Carbidopa (First-line, Gold Standard)
- Levodopa = metabolic precursor of dopamine; crosses the blood-brain barrier (dopamine itself cannot cross)
- Carbidopa = peripheral DOPA decarboxylase inhibitor; prevents conversion of levodopa to dopamine in the periphery
- Together: more levodopa reaches the brain, dose of levodopa is reduced 4-5 fold, peripheral side effects (nausea, vomiting, arrhythmias) are greatly reduced
Adverse effects of levodopa-carbidopa:
- On-off phenomenon - unpredictable motor fluctuations
- Wearing off - effects diminish before next dose
- Dyskinesias (involuntary writhing movements)
- Nausea, vomiting, orthostatic hypotension
- Visual hallucinations, confusion (especially in elderly)
B. Dopamine Receptor Agonists
Bromocriptine (ergot), Ropinirole, Pramipexole, Rotigotine, Apomorphine
- Directly stimulate dopamine receptors in the striatum
- Longer acting than levodopa
- Used as monotherapy in early PD or adjunct to levodopa
- Useful when levodopa response fluctuates
C. MAO-B Inhibitors (Selegiline, Rasagiline)
- Inhibit monoamine oxidase type B - the enzyme that breaks down dopamine in the brain
- Reduce dopamine degradation → more dopamine available
- Selegiline may have mild neuroprotective effects
D. COMT Inhibitors (Entacapone, Tolcapone, Opicapone)
- Inhibit catechol-O-methyltransferase - enzyme that metabolizes levodopa in the periphery
- Used to address "wearing-off" phenomena with levodopa-carbidopa
- Tolcapone can cause hepatic necrosis (liver monitoring required); largely replaced by entacapone
E. Anticholinergics (Benztropine, Trihexyphenidyl)
- Block excess ACh activity in the striatum (restoring DA/ACh balance)
- Especially useful for tremor and rigidity
- Side effects: dry mouth, blurred vision, urinary retention, constipation, confusion (avoid in elderly)
F. Amantadine
- Antiviral drug found to have antiparkinsonian effects
- Increases dopamine release, blocks reuptake, and has NMDA receptor antagonism
- Reduces dyskinesias; useful in early mild PD
G. Surgical Treatment
- Deep Brain Stimulation (DBS) of the subthalamic nucleus or globus pallidus interna
- For patients with advanced PD who do not respond adequately to medications
9. Quick Comparison: PD vs. Drug-Induced Parkinsonism
| Feature | Idiopathic PD | Drug-Induced (Pseudoparkinsonism) |
|---|---|---|
| Cause | Neurodegeneration | DA receptor blockers (antipsychotics) |
| Lewy bodies | Present | Absent |
| Response to levodopa | Yes | No (receptors blocked) |
| Reversibility | No | Yes (on stopping drug) |
10. Key Points to Remember for Exams
- Site of lesion: Substantia nigra pars compacta
- Neurotransmitter: Dopamine deficiency (relative acetylcholine excess)
- Pathological hallmark: Lewy bodies (alpha-synuclein inclusions)
- Classic triad (or tetrad - TRAP): Tremor, Rigidity, Akinesia, Postural instability
- Tremor type: Resting, "pill-rolling", 4-6 Hz
- Rigidity type: Cogwheel
- Gait: Festinating (shuffling, short steps)
- Facial appearance: Masked facies (hypomimia)
- Writing: Micrographia
- Drug of choice: Levodopa + Carbidopa
- Why carbidopa? To prevent peripheral conversion of levodopa; reduces dose and side effects
- Drug-induced parkinsonism: Antipsychotics (haloperidol, phenothiazines) - block D2 receptors
- Surgical option: Deep Brain Stimulation (DBS)
Recent reviews to be aware of: Xiao et al. (2025, PMID 40185518) reviewed updated pathogenesis mechanisms of PD in Neurologic Clinics - consistent with the above, with additional emphasis on mitochondrial dysfunction and neuroinflammation as contributing pathways.
This is a shared conversation. Sign in to Orris to start your own chat.