Can you explain hrct chest from basics
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have everything needed to write a comprehensive, well-structured guide on HRCT chest from basics. Here it is:
HRCT Chest - From Basics
1. What is HRCT?
High-Resolution Computed Tomography (HRCT) of the chest is a specialized CT technique designed to maximize spatial resolution of lung parenchyma. It differs from a standard chest CT in the following key ways:
| Feature | Standard CT | HRCT |
|---|---|---|
| Slice thickness | 5-10 mm | ≤1.5 mm (typically ~1 mm) |
| Reconstruction algorithm | Standard/smooth | High-spatial-frequency (sharp/bone algorithm) |
| Purpose | General survey | Detail of lung parenchyma & interstitium |
| Contrast | Often used | Usually non-contrast |
The thin slices + sharp reconstruction algorithm work together to maximize sharpness in the final image, letting you resolve fine structures like interlobular septa, bronchiole walls, and small vessels that are invisible on standard CT.
Additional sequences routinely added in ILD protocols:
-
Prone images - distinguish dependent atelectasis from true ILD at the bases
-
Expiratory images - detect air trapping (mosaic perfusion, small airway disease)
-
Murray & Nadel's Textbook of Respiratory Medicine, p. 469
2. Why is HRCT More Useful Than a Chest X-Ray?
Multiple studies comparing CT (especially HRCT) to chest radiography have consistently shown HRCT is more sensitive for detecting lung disease. Key advantages:
-
Up to 10% of IPF patients have a normal-appearing chest X-ray, especially early in disease
-
HRCT detects early emphysema, pneumoconiosis, and subtle ILD that is invisible on CXR
-
Reduces interobserver variability and increases diagnostic specificity
-
Allows assessment of disease reversibility and prognosis
-
Can direct biopsy or bronchoalveolar lavage to the most active area
-
Fishman's Pulmonary Diseases and Disorders, p. 949-950
3. The Foundation: Secondary Pulmonary Lobule
Understanding HRCT requires knowing the secondary pulmonary lobule (SPL) - the smallest unit of lung function surrounded by connective tissue septa. Everything you see on HRCT maps to structures within or around this lobule.
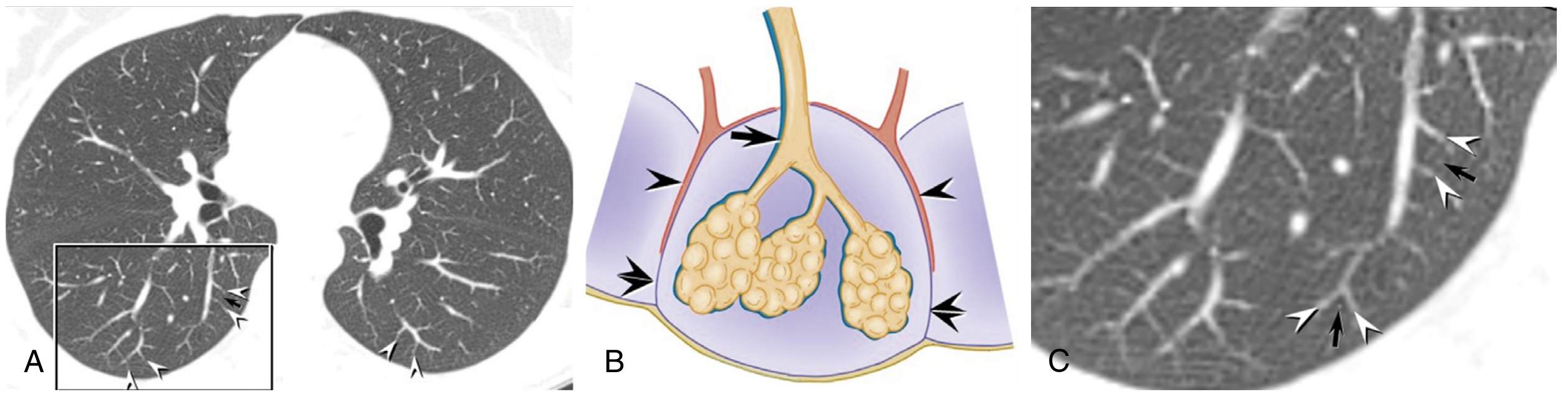
The SPL has three compartments:
- Centrilobular region - contains the terminal bronchiole and centrilobular artery (center of lobule)
- Perilobular/septal region - interlobular septa containing pulmonary veins and lymphatics
- Parenchyma - alveoli filling the lobule
Disease location within the SPL (centrilobular vs. perilymphatic vs. random) is the key to differential diagnosis of nodular patterns.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 469-470
4. The Four Core HRCT Patterns
HRCT abnormalities are broadly classified into 4 patterns. Most diseases show overlap between them.
A. Reticular Pattern
A net-like or mesh-like increase in lung opacity. Almost always represents significant ILD.
Sub-types:
-
Interlobular septal thickening (visible as lines outlining lobules):
- Smooth thickening → pulmonary oedema, alveolar proteinosis
- Irregular/beaded thickening → lymphangitic carcinomatosis, sarcoidosis
-
Intralobular septal thickening → appears as fine ground-glass opacity (below HRCT resolution for discrete lines); seen in most fibrosing ILDs
-
Honeycombing → end-stage fibrosis; clustered cystic air spaces (3-10 mm) with thick walls in a subpleural distribution. The hallmark of UIP/IPF. Must be distinguished from traction bronchiectasis.
-
Traction bronchiectasis/bronchiolectasis → irregular dilation of airways due to surrounding fibrosis; peripheral form can mimic honeycombing
-
Grainger & Allison's Diagnostic Radiology, p. 223-224
B. Nodular Pattern
Nodules in the lung can be interstitial or airspace. Distribution is the key diagnostic clue:
| Distribution | Location within lobule | Key diseases |
|---|---|---|
| Perilymphatic | Interlobular septa, subpleural, peribronchovascular | Sarcoidosis, lymphangitic carcinomatosis |
| Centrilobular | Center of lobule; spares pleura | Hypersensitivity pneumonitis, RB-ILD, endobronchial TB, diffuse panbronchiolitis |
| Random | No lobular predilection | Haematogenous metastases, miliary TB, fungal infections |
Tree-in-bud pattern: Centrilobular nodules with branching appearance → indicates small airway disease (infection, endobronchial spread of TB/bacterial pneumonia).
- Grainger & Allison's Diagnostic Radiology, p. 224
C. Ground-Glass Opacity (GGO) and Consolidation
- Ground-Glass Opacity (GGO): Hazy increased opacity but underlying vessels and bronchi are still visible through it. Implies partial filling of alveoli or interstitial thickening below the resolution of HRCT. Can be reversible (inflammation, oedema) or irreversible (fibrosis - when combined with traction bronchiectasis).
- Consolidation: Opacification that obscures underlying vessels completely. Implies complete filling of airspaces (fluid, pus, blood, tumour cells). Always significant.
GGO + traction bronchiectasis → active fibrosis (not just pure inflammation)
GGO alone → more likely reversible (hypersensitivity pneumonitis, NSIP, DAD)
- Murray & Nadel's Textbook of Respiratory Medicine, p. 471
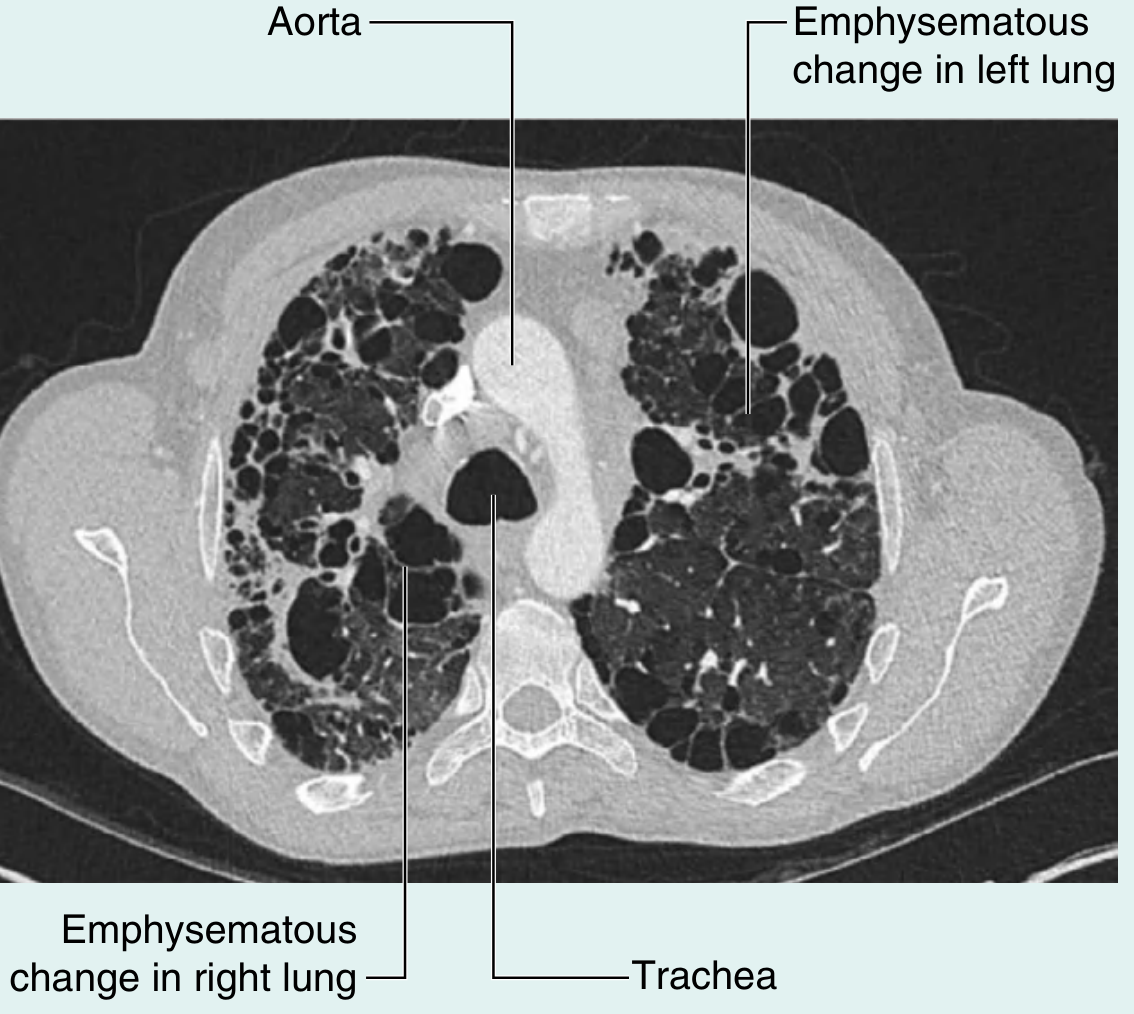
D. Cystic Pattern and Decreased Lung Opacity
- Cysts: Rounded air-containing spaces with a definable wall (unlike emphysema which lacks walls). Key diseases: LAM, LIP, Birt-Hogg-Dubé
- Emphysema: Areas of low attenuation WITHOUT a perceptible wall. Bullae are emphysematous spaces >1 cm
- Cavities: Thick-walled lucencies within consolidation (infection, malignancy, vasculitis)
- Mosaic attenuation pattern: Patchwork of areas with differing density
- Pathological "black" component (increased air) → air trapping (small airway disease) OR reduced vascularity (chronic thromboembolic disease)
- Pathological "grey" component (increased density) → ground-glass from ILD
- Expiratory CT helps: air trapping worsens on expiration, vascular disease stays the same, ILD stays the same
- Grainger & Allison's Diagnostic Radiology, p. 224-226
5. Distribution of Disease: The Other Half of the Diagnosis
After identifying the pattern, distribution is equally important:
| Distribution axis | Examples |
|---|---|
| Upper vs. lower zone predominance | Upper: sarcoidosis, hypersensitivity pneumonitis (chronic), silicosis / Lower: IPF/UIP, NSIP, asbestosis |
| Subpleural vs. central | Subpleural: UIP/IPF, COP / Central (peribronchovascular): sarcoidosis, lymphangitic carcinomatosis |
| Unilateral vs. bilateral | Bilateral symmetric: UIP, NSIP / Unilateral/asymmetric: infection, organising pneumonia |
| Anterior vs. posterior | Prone imaging distinguishes dependent atelectasis (disappears prone) from true ILD (persists prone) |
6. Key Disease Patterns at a Glance
| Disease | Characteristic HRCT Pattern |
|---|---|
| IPF (UIP pattern) | Subpleural basal reticular pattern + honeycombing ± traction bronchiectasis |
| NSIP | Bilateral ground-glass opacity + fine reticulation; subpleural sparing; lower lobe |
| Sarcoidosis | Perilymphatic nodules along bronchovascular bundles + fissures; upper/mid lobe |
| Hypersensitivity pneumonitis | Centrilobular GGO nodules + mosaic attenuation; upper/mid lobe; poorly defined |
| COP | Peripheral/subpleural consolidation; peribronchovascular; migratory |
| Lymphangitic carcinomatosis | Irregular beaded interlobular septal thickening; preserves lung architecture |
| Pulmonary oedema | Smooth interlobular septal thickening (Kerley B lines on CXR); GGO; pleural effusions |
| Miliary TB | Random nodules 1-3 mm throughout both lungs |
| Emphysema | Low attenuation areas without walls; upper lobe centrilobular (smoking) or lower lobe panlobular (AAT) |
- Grainger & Allison's Diagnostic Radiology, pp. 224-226; Murray & Nadel's, p. 470-471
7. UIP Pattern - The Most Tested/Clinically Important
The Fleischner Society 2018 criteria classify UIP on HRCT into four categories (clinically critical for IPF diagnosis):
| Category | Features |
|---|---|
| Typical UIP | Subpleural + basal predominant reticulation + honeycombing ± traction bronchiectasis; no alternate features |
| Probable UIP | Same as above but WITHOUT honeycombing |
| Indeterminate for UIP | Variable/diffuse distribution; fibrosis but inconspicuous features |
| Alternative diagnosis | Upper/mid lung predominant; predominant consolidation; extensive pure GGO; diffuse nodules; mosaic air trapping |
A typical UIP on HRCT has >90% positive predictive value for a histological UIP pattern on biopsy - meaning surgical lung biopsy can be avoided when the pattern is classic.
- Fishman's Pulmonary Diseases and Disorders, p. 950
8. Indications for HRCT Chest
- Suspected interstitial lung disease (ILD)
- Unexplained dyspnoea with normal or non-specific CXR
- Monitoring disease progression in known ILD
- Staging and characterisation of IPF (avoiding biopsy if typical UIP)
- Suspected emphysema or bronchiectasis evaluation
- Evaluation of hemoptysis (alongside bronchoscopy)
- Suspected small airway disease (obliterative bronchiolitis, diffuse panbronchiolitis)
- Occupational lung disease (asbestosis, silicosis, coal worker's pneumoconiosis)
- Pre-transplant lung evaluation
Quick Summary
HRCT = 1 mm slices + high-frequency reconstruction algorithm
↓
Maximizes spatial resolution of lung parenchyma
↓
Identify PATTERN: Reticular | Nodular | GGO/Consolidation | Cystic/Decreased opacity
↓
Add DISTRIBUTION: Upper vs. lower | Subpleural vs. central | Bilateral vs. unilateral
↓
= Narrowed differential diagnosis
The foundation of all HRCT interpretation is the secondary pulmonary lobule - always ask: where within the lobule is the disease? Centrilobular (small airways) vs. perilymphatic (interstitium/lymphatics) vs. random (haematogenous) is the most powerful diagnostic framework for nodular disease, and subpleural/basal vs. upper/central distribution is the key separator for fibrotic and non-fibrotic ILD.
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Grainger & Allison's Diagnostic Radiology; Fishman's Pulmonary Diseases and Disorders; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.