Hypoxix pulmonary vasoconstriction
Reading File
Finding Sources
Searching PubMed
"hypoxic pulmonary vasoconstriction" mechanism
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from three major textbooks. Here is the full, detailed answer:
Hypoxic Pulmonary Vasoconstriction (HPV)
Definition and Key Concept
HPV is a locally mediated reflex unique to the pulmonary circulation in which a fall in alveolar oxygen tension causes constriction of nearby pulmonary arterioles, redirecting blood from poorly ventilated regions to better-ventilated ones. This optimizes ventilation-perfusion (V/Q) matching and arterial oxygenation. Critically, this is the opposite of the systemic response - in other vascular beds (coronary, cerebral, skeletal muscle), hypoxia causes vasodilation.
Stimulus
- HPV is triggered when alveolar PO2 falls below ~60 mmHg
- The response is maximal at an alveolar O2 tension of ~30 mmHg
- It is alveolar PO2 - not pulmonary arterial blood PO2 - that is the principal driver. This has been confirmed by perfusing lungs with oxygenated blood while ventilating with hypoxic gas: vasoconstriction still occurs, proving the oxygen sensor is in the alveolar wall/adjacent vessels, not in the blood
- Mixed venous hypoxia (low perfusate PO2) does contribute, but it is a weaker stimulus
- Both alveolar and perfusate oxygen tensions together determine the full magnitude of HPV
Site of Action
- HPV occurs predominantly in small pulmonary arteries and arterioles (precapillary vessels)
- The oxygen sensor is at a precapillary site: retrograde perfusion experiments in isolated rat lungs showed no HPV when perfusion was reversed, confirming this
- Distribution is uneven in the normal lung (due to sparse, heterogeneous smooth muscle in small pulmonary arteries), which explains why global hypoxia (e.g., at high altitude) produces uneven vasoconstriction - relevant to high-altitude pulmonary edema
Mechanism
HPV does not require central nervous system input (it persists in excised isolated lungs) or autonomic innervation (it persists in transplanted lungs). It is an intrinsic property of pulmonary vascular smooth muscle cells (VSMCs).
Two competing but overlapping hypotheses exist, both placing the oxygen sensor in the mitochondrial electron transport chain:
1. Redox Hypothesis
- Hypoxia → decreased ROS generation by mitochondria → more reduced intracellular redox state
- Sulfhydryl groups on voltage-gated K+ channels (Kv1.5) are reduced → K+ channels close
- Membrane potential depolarizes → voltage-dependent Ca2+ channels open
- Intracellular Ca2+ rises → smooth muscle contraction
2. ROS Hypothesis
- Hypoxia → complex III of mitochondrial ETC generates ROS → released into cytosol
- ROS stimulate Ca2+ influx via nonselective cation channels AND Ca2+ release from sarcoplasmic reticulum via ryanodine receptors
- ROS also activate Rho-kinase (ROCK) → Ca2+ sensitization of myofilaments → augmented contractile response
Both mechanisms converge on increased intracellular Ca2+ and smooth muscle contraction. The final common step also involves connexin 40-mediated retrograde endothelial O2 signaling and Ca2+ influx via TRP1-V4 channels on pulmonary arterioles.
Humoral Modulation
| Factor | Effect on HPV |
|---|---|
| Nitric oxide (NO) | Inhibits HPV (vasodilator via cGMP); NO synthesis inhibitors augment HPV; inhaled NO (≈20 ppm) reduces HPV |
| Endothelins | Pro-constrictive; may augment HPV; endothelin antagonists are now key therapies for pulmonary arterial hypertension |
| Prostacyclin (PGI2) | Inhibits HPV |
| Metabolic acidosis | Augments HPV |
| Metabolic/respiratory alkalosis | Attenuates HPV |
| Hypercapnia/acidosis | Augments HPV (CO2 reduces NO levels) |
| Sympathetic activity | Enhanced HPV (Zucker obese rats, humans with obesity) |
Physiological Roles
-
Local V/Q matching - the most clinically relevant role under normal conditions. Patchy pneumonia, segmental atelectasis, or lobar consolidation triggers local HPV, diverting blood to ventilated areas and limiting arterial hypoxemia.
-
Fetal circulation - arguably the most important physiological role. During fetal life, the lungs do not participate in gas exchange; HPV keeps pulmonary vascular resistance high, limiting pulmonary blood flow to ~15% of cardiac output. At birth, with the first breath and rising alveolar PO2, HPV reverses and pulmonary blood flow surges.
-
One-lung ventilation (OLV) - during thoracic surgery, HPV reduces the shunt fraction through the collapsed (non-ventilated) lung from a potential 20-30% to a lesser degree, protecting arterial oxygenation.
Radiographic Demonstration
The image below, from Miller's Anesthesia, shows HPV in action during one-lung ventilation:
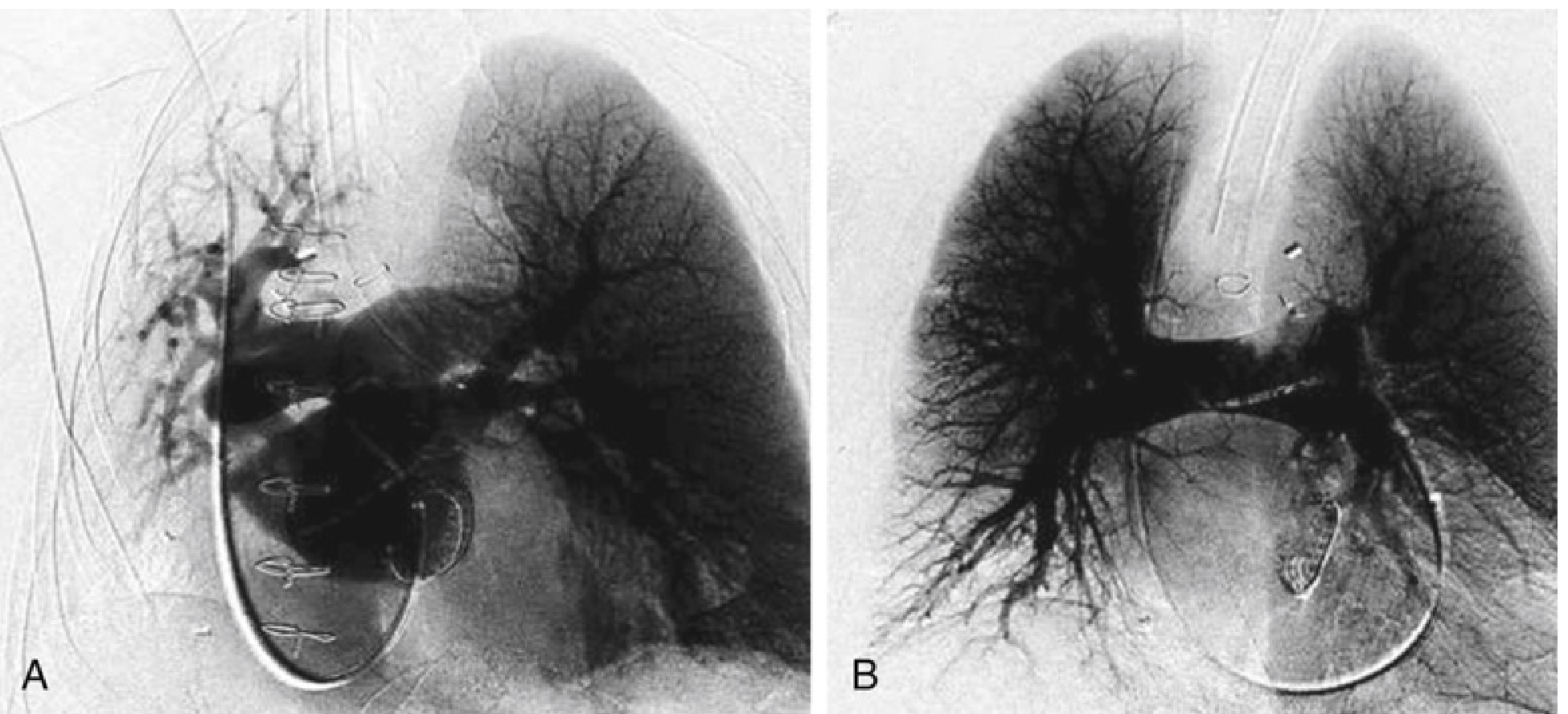
(A) During isolated left-lung ventilation, pulmonary angiogram shows perfusion only to the ventilated (left) lung - the right lung is not receiving microvascular perfusion because HPV has shut down its blood supply. (B) During two-lung ventilation, symmetric microvascular perfusion is restored to both lungs.
Clinical Consequences and Inhibition of HPV
Factors that inhibit HPV (worsen venous admixture and V/Q mismatch):
- Inhalational anesthetics (halothane, isoflurane, sevoflurane, desflurane): all attenuate HPV; ED50 is approximately twice MAC. This is a critical consideration during OLV for thoracic surgery. In contrast, most IV anesthetics (propofol, ketamine, opioids) do not inhibit HPV; propofol may actually potentiate HPV via K(ATP)-channel inhibition.
- Vasodilators: nitroglycerin, nitroprusside, inhaled NO, prostacyclin
- Phosphodiesterase inhibitors: milrinone, enoximone, inamrinone
- Beta-adrenergic agonists (some bronchodilators in asthma - this is the mechanism by which certain bronchodilators paradoxically worsen PaO2 in asthmatics)
- Calcium channel blockers
- Pulmonary hypertension (elevated PA pressure causes passive distension of constricted vessels)
- Hypocapnia/alkalosis
- Elevated cardiac output and high mixed venous PO2
- Hypothermia
- ARDS mediators (secondary inflammatory mediators increase capillary permeability and inhibit HPV)
Supplemental O2 in COPD also inhibits HPV (by raising alveolar PO2), redistributing flow to previously hypoxic, poorly ventilated areas and worsening V/Q mismatch - contributing to hypercapnia in O2-treated COPD exacerbations.
Global vs. Local Hypoxia
| Condition | Type of Hypoxia | Effect |
|---|---|---|
| Lobar pneumonia, atelectasis | Local (focal) | Beneficial HPV: blood diverted away, V/Q improved |
| High altitude | Global | Generalized HPV → pulmonary hypertension; uneven vasoconstriction → high-altitude pulmonary edema |
| Prolonged global hypoxia | Sustained global | HPV suppressed over time; structural remodeling takes over |
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Miller's Anesthesia, 10e; Morgan & Mikhail's Clinical Anesthesiology, 7e
This is a shared conversation. Sign in to Orris to start your own chat.