Coronary anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Coronary Anatomy
Overview
The two coronary arteries - left and right - are the first branches of the aorta and are the sole arterial supply to the myocardium. They originate from the sinuses of Valsalva just above the aortic valve cusps and run in the epicardial fat before penetrating into the myocardium.
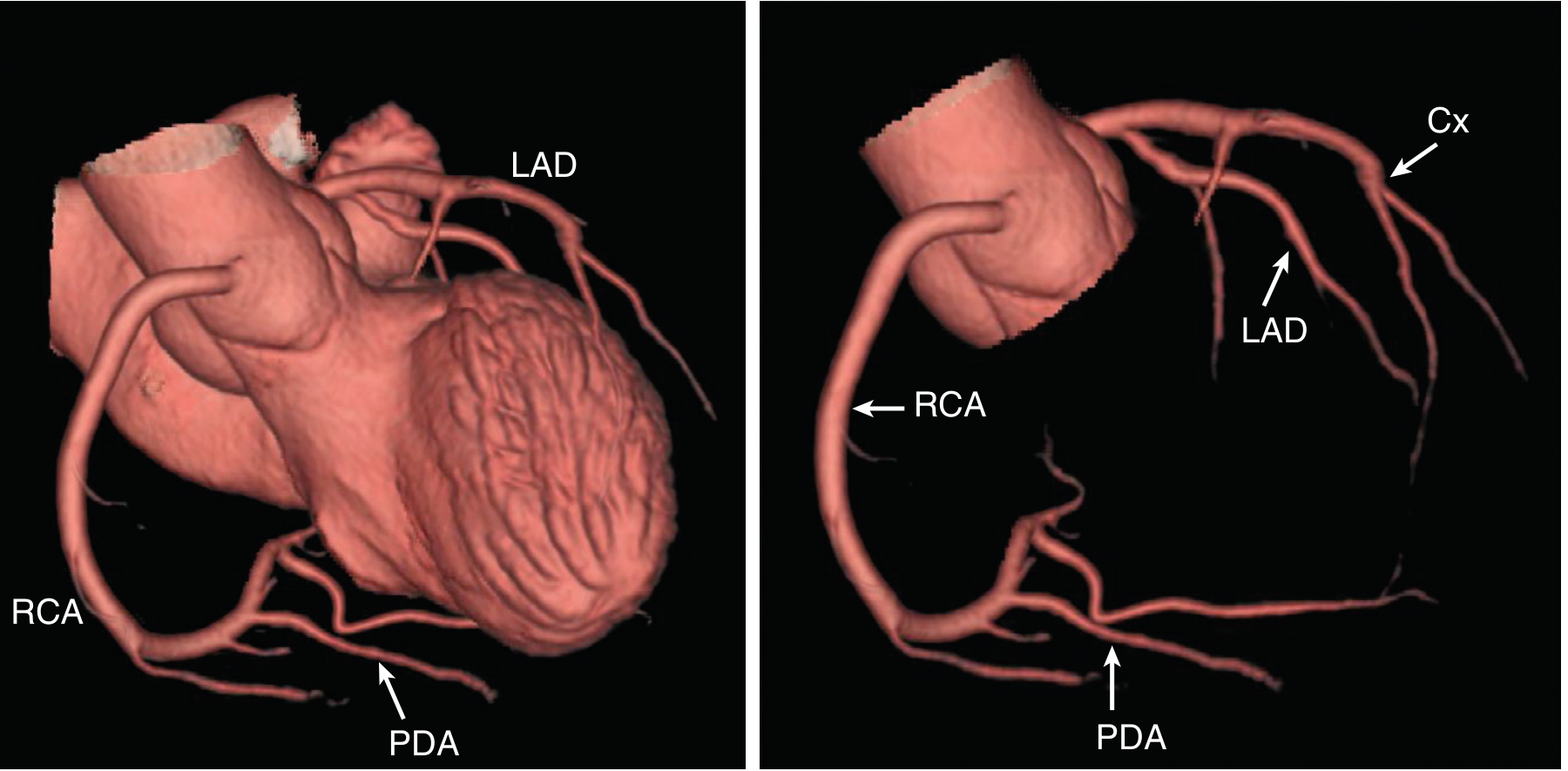
CT reconstruction showing the RCA, LAD, circumflex (Cx), and posterior descending artery (PDA):
Left Coronary Artery (LCA / Left Main)
The left main coronary artery (LMCA) originates from the left coronary sinus of Valsalva. It passes posterolateral to the main pulmonary trunk for approximately 1 cm before bifurcating into its two main branches. The left main varies greatly in length - from a few millimeters to several centimeters.
1. Left Anterior Descending (LAD) Artery
- Takes an anterolateral course relative to the pulmonary trunk
- Runs in the anterior interventricular sulcus toward the apex
- Extends around the apex in many cases, anastomosing with the PDA inferiorly
- Branches:
- Septal perforators - supply the anterior two-thirds of the interventricular septum
- Diagonal branches - supply the anterior LV free wall
2. Circumflex (Cx) Artery
- Follows the left atrioventricular groove around the left border to the posterior surface
- Terminates before reaching the crux (in most people)
- Branches:
- Obtuse marginal (OM) branches - supply the lateral LV wall
- Left marginal branch - follows the left margin of the heart
- Sinoatrial nodal branch in ~40% of people (courses on the posterior surface of the left atrium to the SA node)
- In left-dominant circulation: gives rise to the posterior descending artery (PDA)
Right Coronary Artery (RCA)
Originates from the right coronary sinus of Valsalva. Its ostium averages 2-3 mm in diameter. It runs obliquely rightward in the anterior atrioventricular sulcus, then continues posteriorly in the same groove, supplying the right atrium and right ventricle.
Branches:
- Sinoatrial (SA) nodal artery - arises near the origin of the RCA; supplies the SA node in ~60% of people
- Right marginal branch (Acute Marginal Artery, AMA) - supplies the inferior/lateral border of the RV; reaches toward the apex and forms anastomoses with the LAD
- Posterior descending artery (PDA) - in right-dominant circulation; lies in the posterior interventricular groove; supplies the inferior ventricular septum, inferior walls, and septal papillary muscle of the mitral valve via septal perforating branches
- Right posterolateral artery
- AV nodal artery (AVNA) - originates at the crux of the heart; supplies the AV node; arises from the RCA in ~80% of people. Compromise can cause heart block or arrhythmias.
Coronary Dominance
Dominance is defined by which artery gives rise to the PDA (posterior descending artery).
| Pattern | Frequency | PDA origin |
|---|---|---|
| Right dominant | ~80-85% | RCA |
| Left dominant | ~8-15% | Circumflex artery |
| Codominant | ~7% | Both RCA and Cx |
Coronary dominance variations - anterior and transverse views showing myocardial territory supplied by RCA vs LCA:
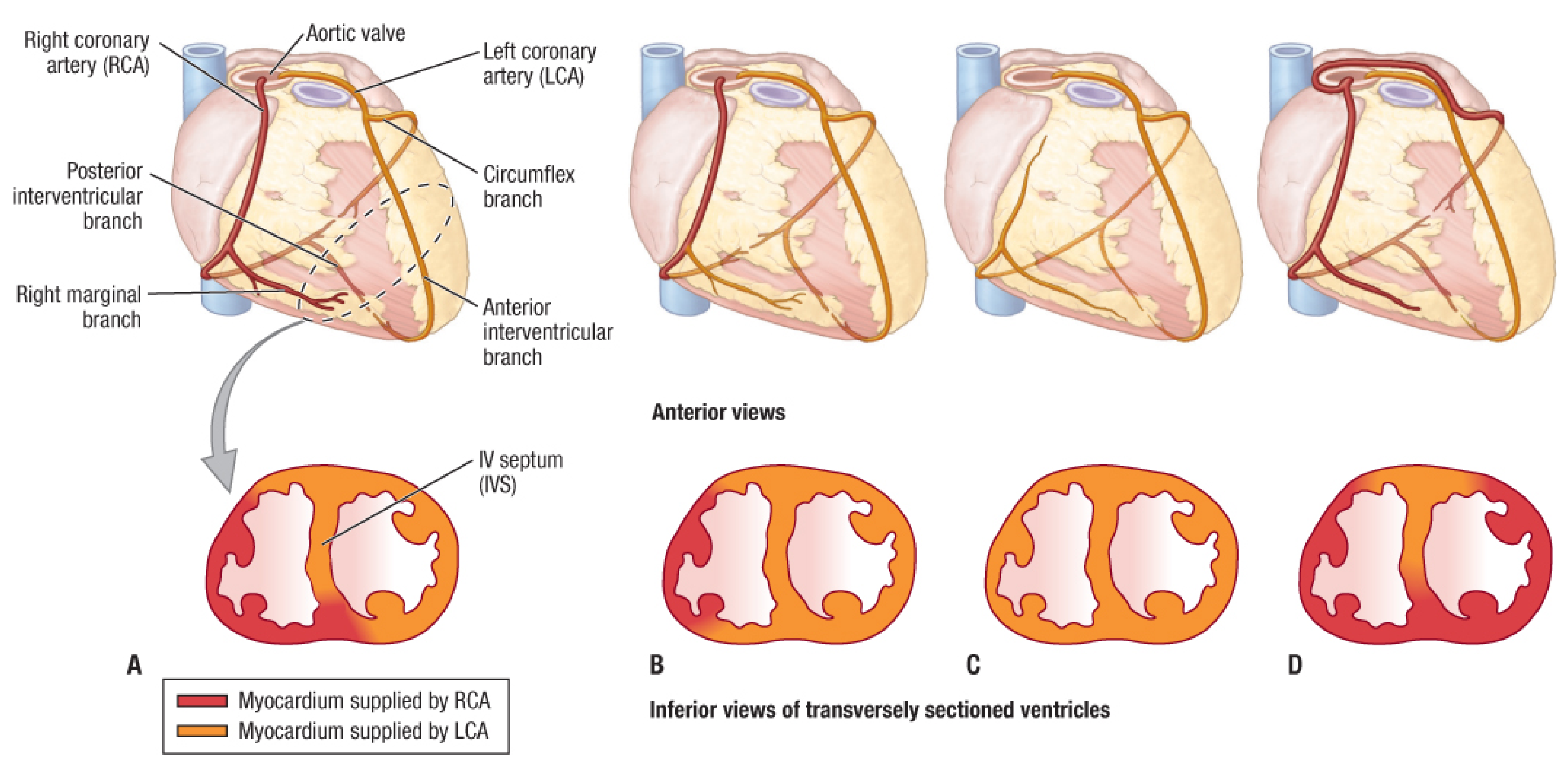
Left-dominant circulation carries a slightly higher mortality risk (HR ~1.13) in acute coronary syndrome because both the PDA territory AND the LV are supplied by the left coronary system. Isolated left main stenosis occurs in only 4-6% of cases, but given that 75-100% of the LV is supplied by LMCA branches, left main disease carries extraordinarily high mortality.
Myocardial Territories (Coronary-Wall Segment Correlation)
| Coronary Artery | Myocardial Territory |
|---|---|
| LAD | Anterior septum (via septal perforators), anterior LV wall (via diagonals), LV apex (usually) |
| Circumflex | Lateral LV wall (via obtuse marginals), inferolateral (posterior) wall |
| RCA / PDA | Inferior septum, inferior LV free wall, RV free wall, AV and SA nodes |
The LV apex has the most variable supply - it may come from the LAD alone, PDA alone, or both (most commonly).
Cardiac Veins
The heart drains primarily through veins emptying into the coronary sinus, and partly by small veins draining directly into the right atrium (Thebesian veins).
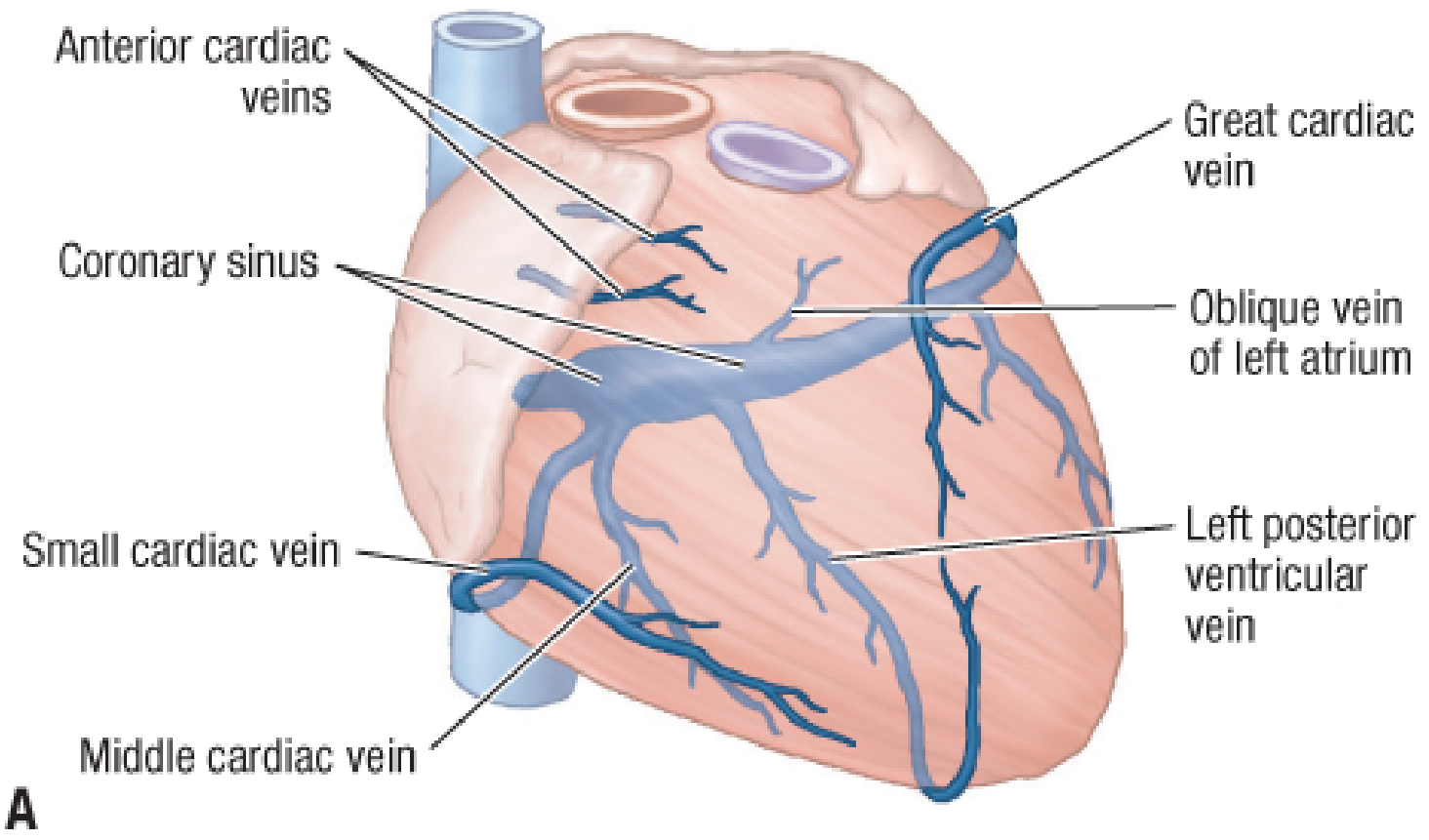
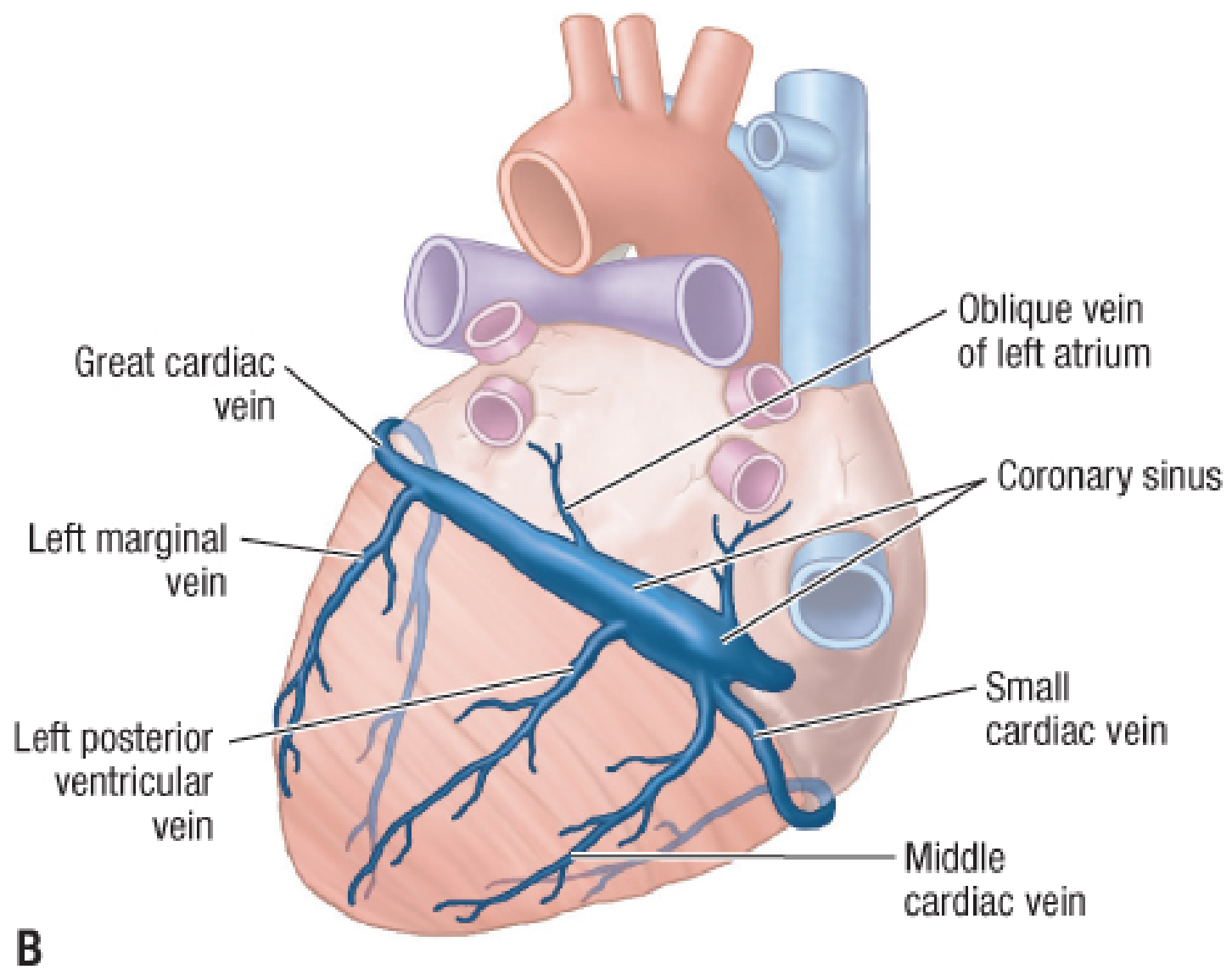
Cardiac venous anatomy - anterior view (A) and posteroinferior view (B):
| Vein | Course | Drains Into |
|---|---|---|
| Great cardiac vein | Starts at apex, runs in anterior interventricular sulcus with LAD, then passes posteriorly in the coronary sulcus | Coronary sinus (left end) |
| Middle cardiac vein | Starts at apex, runs in posterior interventricular sulcus with PDA | Coronary sinus (right end) |
| Small cardiac vein | Accompanies right marginal artery, then turns posteriorly in coronary sulcus | Coronary sinus (right end) |
| Anterior cardiac veins | Drain anterior RV wall | Directly into right atrium |
| Oblique vein of left atrium | Runs on posterior LA | Coronary sinus |
| Left posterior ventricular vein | Drains posterior LV | Coronary sinus |
The coronary sinus is a wide venous channel running left-to-right in the posterior part of the coronary sulcus, draining into the right atrium.
Key Clinical Points
- Left main stenosis is the highest-risk coronary lesion; it is found in combination with multivessel disease in 94-96% of cases
- The AV nodal artery arises from the RCA at the crux in ~80% of people - RCA occlusion can cause complete heart block
- The SA nodal artery comes from the RCA in ~60% and from the Cx in ~40% - relevant in planning ablation procedures
- The LAD is the most commonly diseased coronary artery and is sometimes called the "widow maker" when proximally occluded
Sources: Textbook of Clinical Echocardiography; Fischer's Mastery of Surgery, 8th ed.; Sabiston Textbook of Surgery, 21st ed.
Coronary anatomy as seen during cardiac surgery
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I have comprehensive material. Now let me compile the full surgical-perspective answer.
Coronary Anatomy as Seen During Cardiac Surgery
1. The Surgical Approach: Median Sternotomy
The standard access for cardiac surgery is a median sternotomy. The sternum is divided exactly in the midline. Deep to it, from cranial to caudal, the surgeon encounters:
- Interclavicular ligament
- Brachiocephalic (innominate) artery (sometimes just deep to the inferior thyroid vein)
- Left brachiocephalic vein
- Thymus (or thymic remnants)
- Pericardial sac and ascending aorta
- Right atrium and right ventricle anteriorly
- Diaphragm inferiorly
The internal mammary (thoracic) arteries descend about 1 cm lateral to the sternal margin, deep to the costal cartilages - this is the distance that must be respected during sternotomy and during IMA harvest.
The pericardium is covered with a variable layer of epicardial fat and is swept laterally before a midline incision exposes the heart.
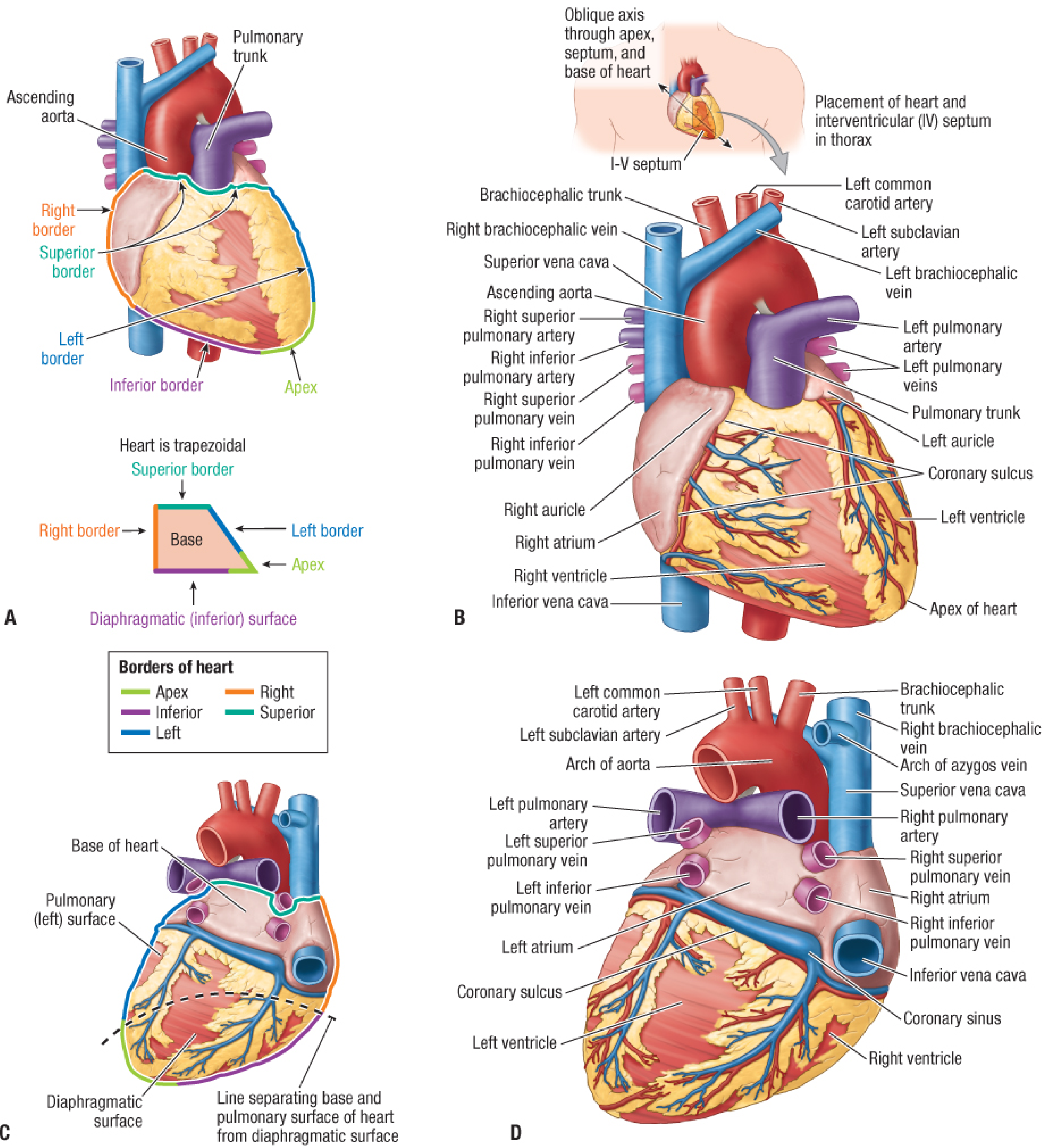
2. The Heart as Seen After Pericardiotomy
The heart appears trapezoidal with an apex, base, four borders, and four surfaces:
Surfaces directly visible surgically:
| Surface | Formed by | What the surgeon sees |
|---|---|---|
| Anterior (sternocostal) | Mainly right ventricle | Immediately faces the surgeon after pericardiotomy; LAD visible in anterior interventricular groove |
| Diaphragmatic (inferior) | LV (mostly) + RV | Accessed by lifting heart; PDA visible in posterior interventricular groove |
| Right pulmonary surface | Right atrium | Cannulation site for venous CPB cannula; right auricle accessible |
| Left pulmonary surface | Left atrium | Accessed by retracting heart rightward |
Key sulci (grooves) that guide the surgeon to coronary targets:
- Coronary sulcus (atrioventricular groove) - encircles the heart; separates atria from ventricles; contains the RCA (right side) and circumflex (left side), both buried in fat
- Anterior interventricular sulcus - runs down the anterior surface; contains the LAD and great cardiac vein
- Posterior interventricular sulcus - runs down the diaphragmatic surface; contains the PDA and middle cardiac vein
3. Coronary Arteries: What the Surgeon Sees
The Anterior Surface (Sternocostal View - First View After Pericardiotomy)
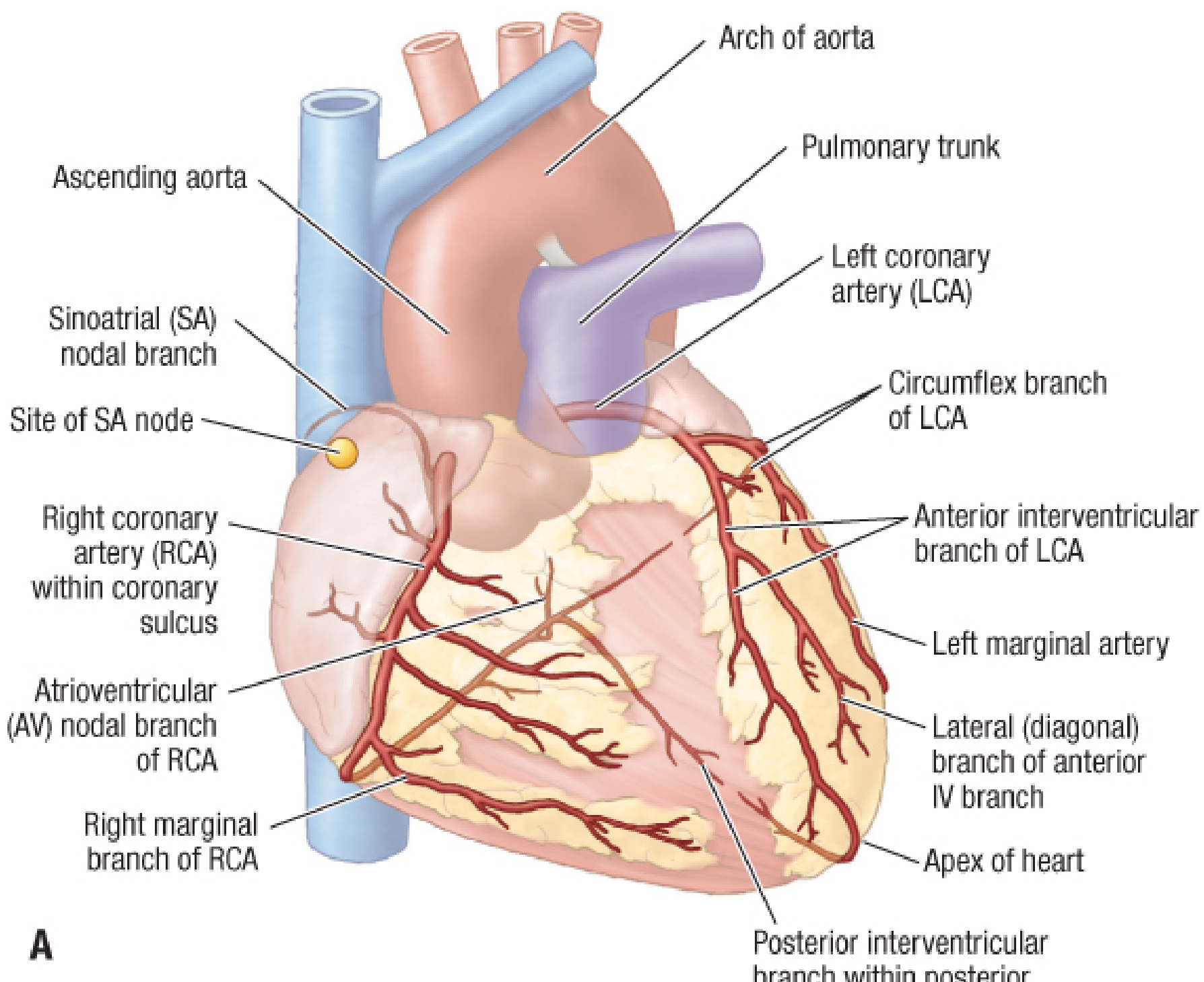
From this view the surgeon identifies:
- Ascending aorta and pulmonary trunk at the top - the aorta is the proximal anastomosis site for vein grafts
- Right coronary artery (RCA) - visible on the right side running in the right atrioventricular (coronary) sulcus, partially buried in fat, coursing from the aortic root rightward and downward around the right border
- Anterior interventricular branch (LAD) - runs in the anterior interventricular groove, partially covered by subepicardial fat; the most frequently bypassed vessel
- Diagonal branches - branch off the LAD diagonally onto the anterior LV surface; numbered D1, D2 from proximal to distal
- Circumflex artery - runs in the left atrioventricular groove, hidden by the left auricle; gives rise to obtuse marginal (OM) branches that course over the lateral LV wall
- Right marginal (acute marginal) branch of RCA - visible along the inferior (acute) border of the right ventricle, courses toward the apex
- SA nodal branch - small, arises from the RCA near its origin, ascends toward the right atrial groove (sulcus terminalis)
- Great cardiac vein - runs alongside the LAD in the anterior interventricular sulcus (important to avoid during LAD grafting)
The Posterior/Diaphragmatic View (Heart Lifted or Rotated)
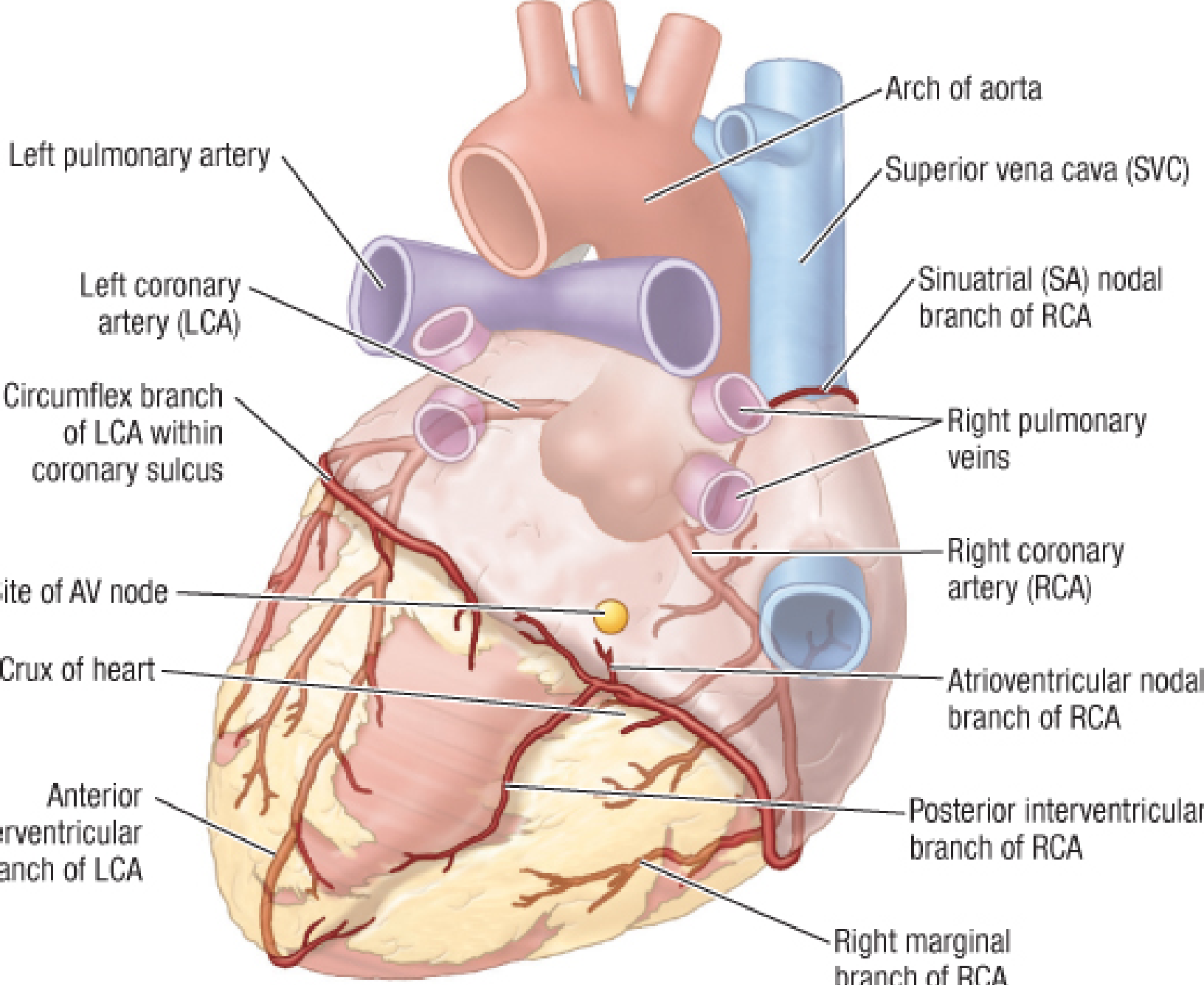
From this view:
- Posterior interventricular branch (PDA) - visible in the posterior interventricular groove, coursing toward the apex
- Crux of the heart - the crossing point of the posterior interventricular sulcus and the coronary sulcus; the AV nodal artery arises here (from the RCA in ~80%), supplying the AV node (marked by the yellow dot in the diagram above)
- Circumflex artery - visible in the left coronary sulcus, giving rise to obtuse marginal branches on the posterolateral LV
- Coronary sinus - large venous structure in the posterior coronary sulcus draining into the right atrium; used for retrograde cardioplegia delivery
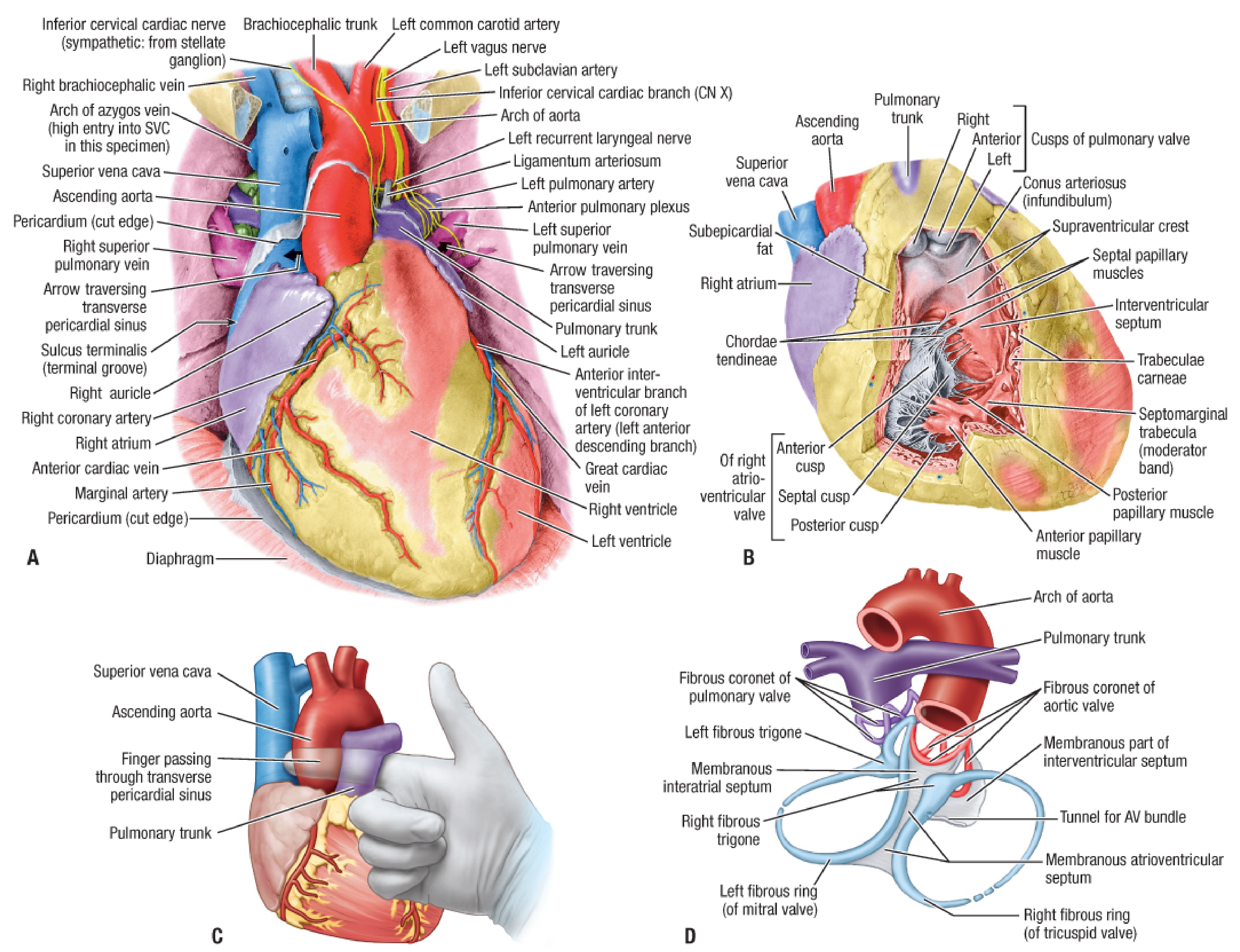
4. Full Labeled Surgical Anatomy (Anterior and Posterior)
Anterior in-situ view with pericardium opened:
All surfaces, borders, and posteroinferior view:
5. Interventricular Septum Blood Supply (Surgically Relevant)
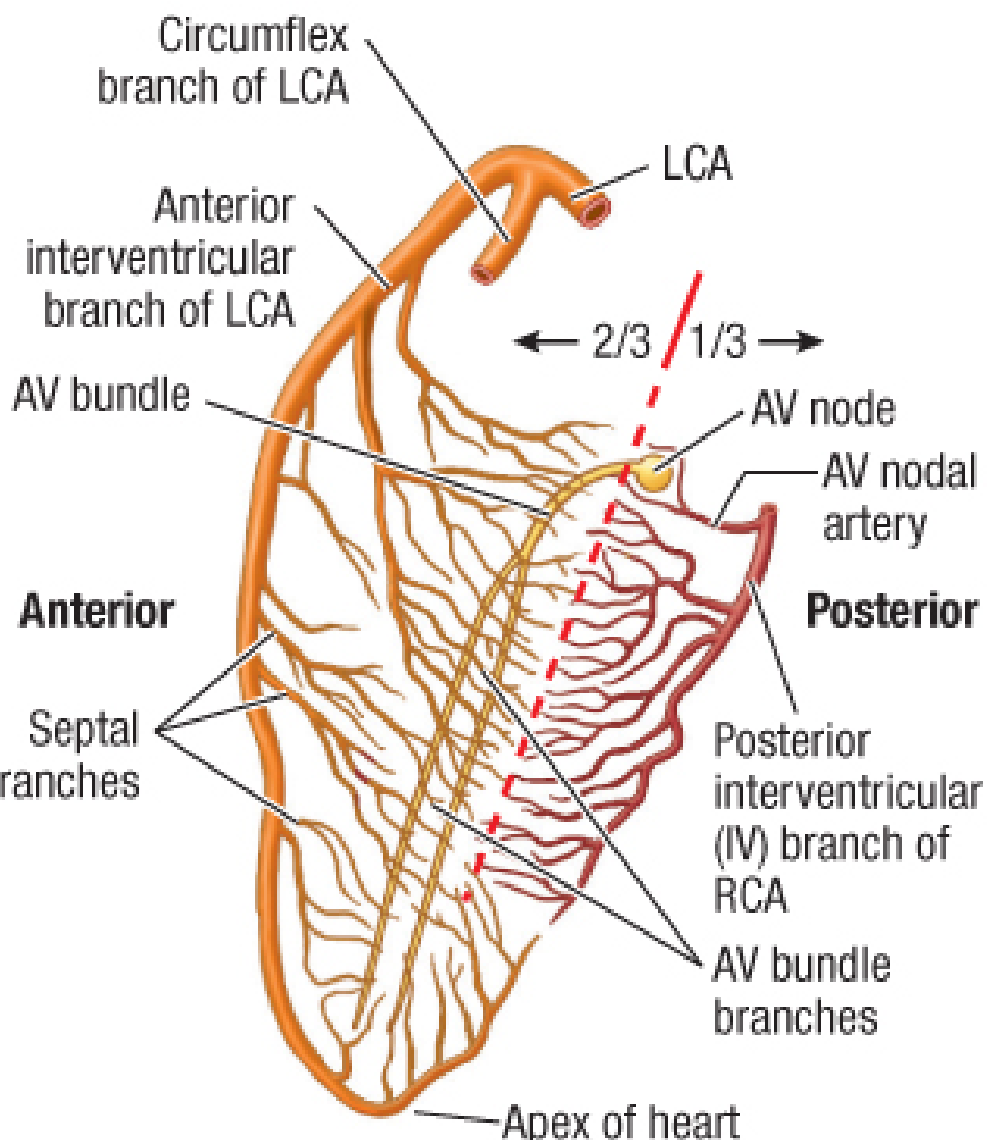
- Anterior 2/3 of septum - supplied by septal perforators of the LAD; these arise at right angles and dive deep; cutting them (e.g., during VSD repair or myomectomy) risks septal infarction
- Posterior 1/3 of septum - supplied by septal branches of the PDA (from RCA in right-dominant circulation)
- AV node and proximal AV bundle - sit at the crux, supplied by the AV nodal artery; at risk during posterior septal surgery
6. Key Surgical Landmarks and Their Clinical Importance
| Structure | Surgical Significance |
|---|---|
| Transverse pericardial sinus | Window posterior to aorta and pulmonary trunk; a finger passed through it separates these vessels for snaring during CPB setup |
| Right auricle | First cannulation point for venous return cannula in CPB |
| Ascending aorta | Site for aortic cannulation and proximal graft anastomoses; cross-clamp applied here for cardioplegia |
| Anterior interventricular sulcus (LAD) | Main CABG target; LAD runs here under fat, alongside the great cardiac vein |
| Coronary sulcus | Contains RCA (right) and Cx (left); epicardial fat must be cleared to expose these vessels |
| Posterior interventricular sulcus (PDA) | Grafted in right-dominant circulation; accessed by lifting the heart |
| Crux of heart | Extreme care needed here - AV nodal artery, coronary sinus opening |
| Internal mammary arteries | Run ~1 cm lateral to sternal edge; the LIMA is the preferred conduit for LAD grafting and must be harvested before sternum is split |
7. Epicardial Fat: The Surgeon's Practical Challenge
The coronary arteries themselves are not directly visible on the epicardial surface - they run embedded in subepicardial fat within the sulci. The surgeon must clear this fat to expose the target vessel for arteriotomy. The density of this fat varies greatly between patients (e.g., obese, diabetic patients may have very thick fat pads obscuring even large vessels). The vessels are identified by palpation of the groove, visualization of accompanying veins, and pre-operative angiographic mapping.
Sources: Fischer's Mastery of Surgery, 8th ed. (Ch. 273 - Surgical Anatomy of the Heart); Sabiston Textbook of Surgery, 21st ed. (Ch. 111 - CABG); Textbook of Clinical Echocardiography
This is a shared conversation. Sign in to Orris to start your own chat.