Peptic ulcer
Reading File
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough, well-cited response.
Peptic Ulcer Disease (PUD)
Definition
Peptic ulcer disease refers to full-thickness mucosal defects in portions of the gastrointestinal tract that are exposed to acid and pepsin. Although the name implies a central role for pepsin, acid is the indispensable factor - peptic ulcers do not occur in the absence of acid, and they heal when acid is suppressed to near-achlorhydric levels with PPIs. - Bailey and Love's Surgery, p. 1178
Sites
| Site | Notes |
|---|---|
| First part of duodenum | Most common overall |
| Gastric antrum / lesser curve (incisura angularis) | Most common gastric site |
| Stomal (post-surgical) | At gastrojejunal junction |
| Oesophagus (via GERD or ectopic mucosa) | Less common |
| Meckel's diverticulum | Contains ectopic gastric epithelium |
Ulcers characteristically form at the junction between different epithelial types, where resistance to acid damage is lowest. - Bailey and Love's Surgery, p. 1178
Aetiology and Pathogenesis
The key principle is an imbalance between mucosal offensive forces (acid, pepsin, H. pylori, NSAIDs) and defensive forces (mucus, bicarbonate, mucosal blood flow, prostaglandins).
1. Helicobacter pylori
- Responsible for >70% of PUD cases.
- Found in almost all duodenal ulcer patients and ~70-80% of gastric ulcer patients.
- Only 5-10% of infected individuals develop ulcers, implying host and strain-specific cofactors.
- Acts by disrupting the mucus layer, triggering inflammation, and increasing gastric acid output (via gastrin upregulation). - Robbins & Kumar Basic Pathology, p. 589
2. NSAIDs (including aspirin)
- Inhibit COX enzymes, suppressing prostaglandin synthesis, which reduces mucus and bicarbonate secretion and impairs mucosal blood flow.
- Asymptomatic peptic ulceration develops in 10-20% of regular NSAID users; ulcer complications (bleeding, perforation) occur in 1-2% per year. - Katzung's Pharmacology, 16th ed.
- In the US, NSAID-induced gastric ulcers are now becoming the leading cause as H. pylori rates fall and low-dose aspirin use rises in aging populations. - Robbins & Kumar, p. 589
3. Acid hypersecretion
- Duodenal and prepyloric ulcer patients tend to have higher gastric acid levels vs. controls, though the overlap is wide.
- Gastric ulcer patients often have normal acid levels - mucosal defence failure is more relevant.
- Extreme acid hypersecretion (e.g., gastrinoma in Zollinger-Ellison syndrome) causes florid, treatment-resistant ulcers. - Bailey and Love's Surgery, p. 1179
4. Other cofactors
- Cigarette smoking - reduces mucosal blood flow and increases relapse rates.
- Corticosteroids - suppress prostaglandin synthesis, impair healing.
- Alcohol-related cirrhosis, COPD, chronic renal failure, hyperparathyroidism - all increase PUD risk.
- Hypercalcaemia (from hyperparathyroidism or renal failure) stimulates gastrin secretion.
- Robbins & Kumar, p. 589
Endoscopic Appearance
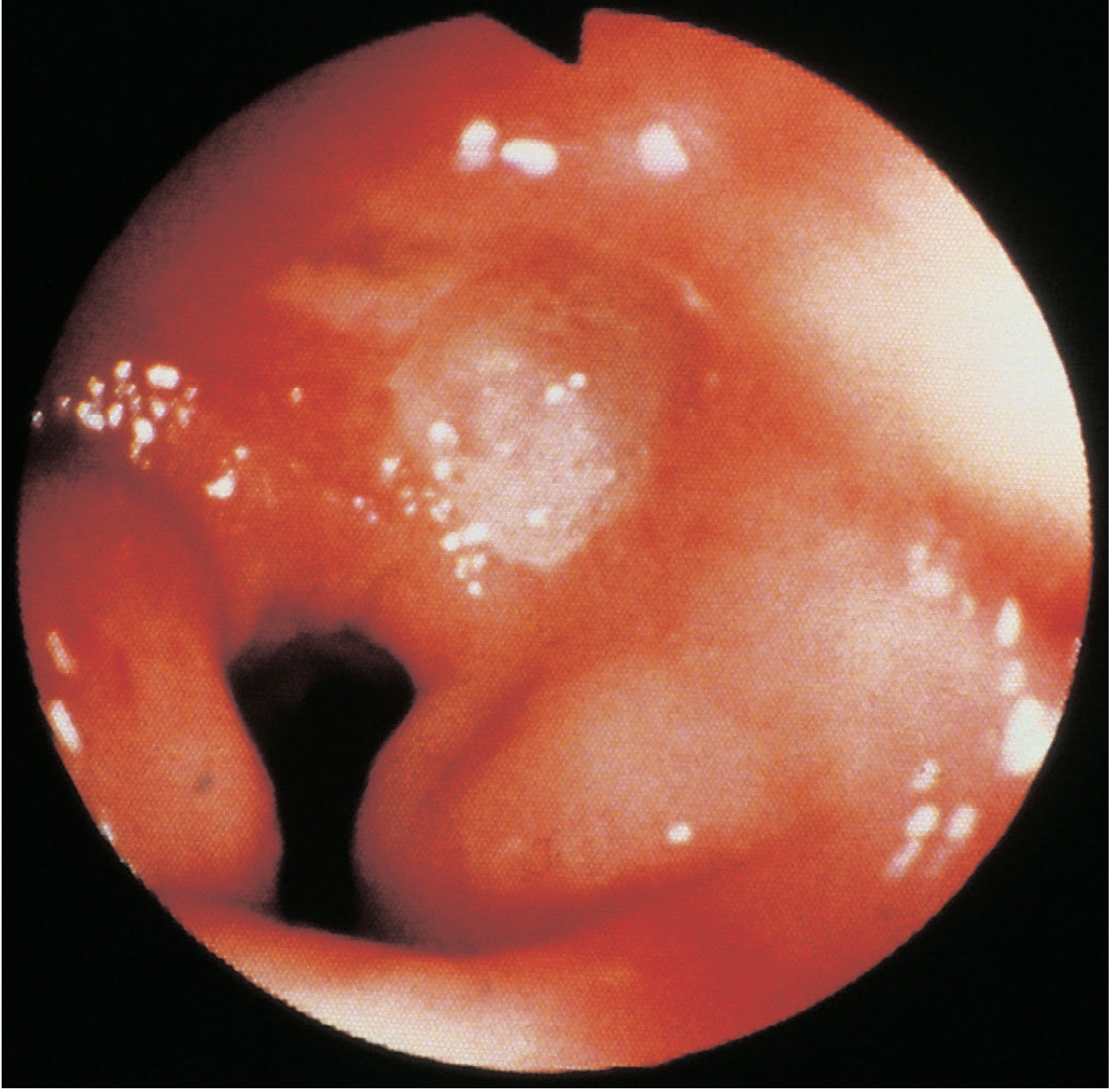
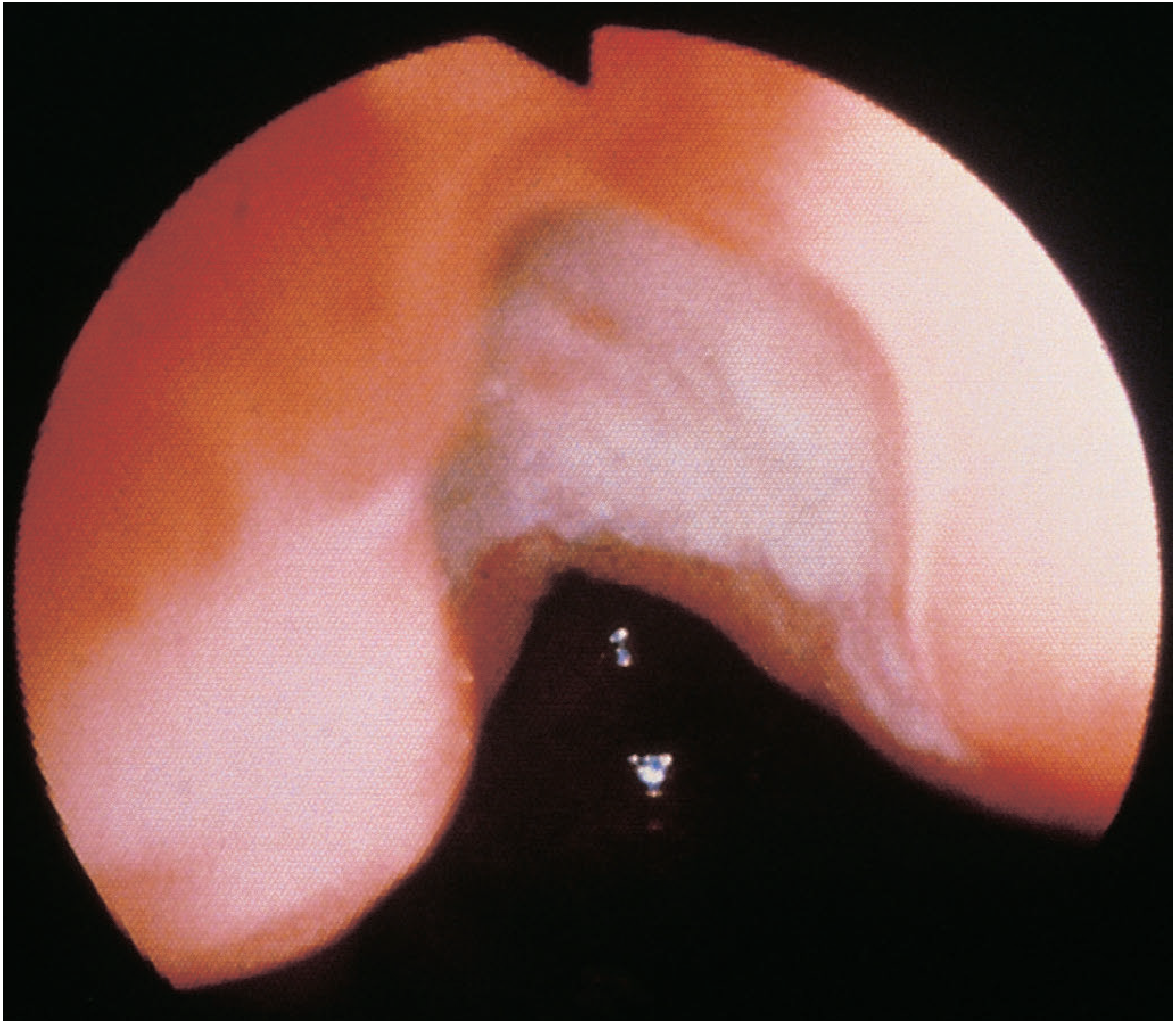
Duodenal vs Gastric Ulcer: Key Distinctions
| Feature | Duodenal Ulcer (DU) | Gastric Ulcer (GU) |
|---|---|---|
| Frequency | More common | Less common |
| Gender | Male > female | Equal |
| Age | Younger | Older |
| Acid secretion | Often elevated | Normal or low |
| Malignant potential | Virtually nil | Present - must biopsy |
| Perforation | Anterior wall ulcers | Can also perforate |
| Bleeding | Posterior wall (erodes gastroduodenal artery) | Can bleed from splenic artery |
| "Kissing ulcers" | Anterior + posterior DU simultaneously | Not applicable |
A healing gastric ulcer can mimic malignancy endoscopically - multiple biopsies are mandatory. About 70% of gastric cancers presenting as ulcers show apparent (incomplete) healing on follow-up. - Harrison's Principles, 22nd ed.
Clinical Features
- Epigastric pain - the cardinal symptom; often described as burning or gnawing.
- Relationship to meals: DU pain classically comes 2-3 hours after eating and at night (relieved by food); GU pain may be precipitated by eating.
- Symptoms are often indistinguishable between DU and GU.
- Examination typically reveals epigastric tenderness; significant findings are absent unless a complication has occurred.
- Bailey and Love's Surgery, p. 1180
Investigations
- Upper GI endoscopy (gastroduodenoscopy) - gold standard; allows biopsy, CLO (Campylobacter-like organism) testing for H. pylori, and assessment of the antrum, pylorus, duodenum, and GOJ.
- H. pylori testing: CLO test (endoscopic biopsy), urea breath test (UBT), or monoclonal stool antigen test for non-invasive detection.
- Barium meal - historical; shows characteristic "niche" sign.
- GU at body or fundus - must biopsy and re-endoscope at 8-12 weeks to confirm healing. DU does not routinely require repeat endoscopy unless symptoms persist.
- Harrison's Principles 22nd ed.; Bailey and Love's Surgery
Treatment
1. H. pylori-associated ulcers
Two goals: heal the ulcer and eradicate the organism.
Standard triple therapy (14 days):
- PPI (twice daily) + clarithromycin 500 mg BD + amoxicillin 1 g BD (or metronidazole 500 mg BD)
Quadruple therapy (now preferred first-line in areas with high clarithromycin resistance or prior clarithromycin exposure - 14 days):
Option A (bismuth quadruple):
- PPI BD + bismuth subsalicylate 524 mg QID + metronidazole 500 mg QID + tetracycline 500 mg QID
Option B (concomitant):
- PPI BD + amoxicillin 1 g BD + clarithromycin 500 mg BD + metronidazole 500 mg BD
After completing antibiotics, continue PPI once daily for 4-6 weeks total to ensure ulcer healing.
Confirm eradication 4 weeks after antibiotic completion with UBT or stool antigen test (not serology). Stop PPI at least 2 weeks before testing to avoid false negatives. - Katzung's Pharmacology 16th ed., Harrison's 22nd ed.
2. NSAID-associated ulcers
- Discontinue the NSAID if possible; treat with PPI or H2-antagonist.
- If NSAID cannot be stopped, a PPI more reliably promotes healing than an H2-blocker.
- For prevention: daily PPI in patients requiring chronic NSAID/aspirin therapy. - Katzung's Pharmacology 16th ed.
3. Acid suppression agents
- PPIs (omeprazole, esomeprazole, pantoprazole, lansoprazole): render patients virtually achlorhydric; most potent.
- H2-receptor antagonists (ranitidine, famotidine): still effective but less so than PPIs; useful in mild disease or prevention.
4. Lifestyle modification
- Cessation of smoking (reduces mucosal blood flow and increases relapse rate).
- Avoid NSAIDs, limit alcohol.
5. Refractory ulcers
- GU failing to heal after 12 weeks / DU after 8 weeks = refractory.
- Exclude: poor compliance, persistent H. pylori, covert NSAID use, continued smoking.
- Consider ZES or idiopathic acid hypersecretion. Check fasting serum gastrin.
- Harrison's Principles 22nd ed.
Complications
| Complication | Notes |
|---|---|
| Haemorrhage | Most common; posterior DU bleeds from gastroduodenal artery; Rockall score guides risk stratification |
| Perforation | Anterior DU most common; peritonitis; surgical emergency |
| Penetration | Posterior GU erodes into pancreas, splenic artery, or transverse colon |
| Gastric outlet obstruction (pyloric stenosis) | From fibrosis/scarring; presents with vomiting, succussion splash |
| Malignant transformation | Only in GU (rare); always biopsy |
The Rockall scoring system (age, haemodynamics, comorbidity, diagnosis, endoscopic stigmata) stratifies rebleeding risk and mortality after upper GI bleeding - Sleisenger and Fordtran's GI and Liver Disease
Epidemiology
- Lifetime risk: ~10% in men, ~4% in women.
- More than 4 million Americans treated annually.
- Incidence of H. pylori-related ulcers is declining in developed countries; NSAID-related ulcers are proportionally increasing.
- In developing nations, H. pylori remains the predominant cause. - Robbins & Kumar, p. 589
Recent Evidence
Three recent systematic reviews are relevant (PubMed, 2024-2025):
- PMID 38818853 (2024): Endoscopic vs. medical management of peptic ulcers with adherent clots - meta-analysis showing endoscopic therapy reduces rebleeding.
- PMID 40337979 (Cochrane, 2025): PPIs effectively prevent NSAID-induced ulcers and dyspepsia, supporting their use as prophylaxis in high-risk NSAID users.
- PMID 40132025 (2025): Pharmacist-led interventions improve PUD management outcomes.
Sources: Robbins & Kumar Basic Pathology | Bailey and Love's Short Practice of Surgery 28e | Harrison's Principles of Internal Medicine 22e | Katzung's Basic and Clinical Pharmacology 16e | Sleisenger and Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.