Whipple surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
pancreaticoduodenectomy Whipple procedure outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have very comprehensive content from multiple authoritative surgical textbooks. Let me compile the full answer.
Whipple Procedure (Pancreaticoduodenectomy)
The Whipple procedure, formally called pancreaticoduodenectomy (PD), is one of the most technically demanding operations in general surgery. It involves removal of the pancreatic head, duodenum, gallbladder, common bile duct, and (in the classic version) the distal stomach, followed by reconstruction of digestive continuity.
Overview and History
The operation was popularized by Allen Whipple at Columbia in the 1930s. A key modification - the pylorus-preserving pancreaticoduodenectomy (PPPD) - was introduced by Traverso and Longmire in 1978, preserving antral and pyloric function while producing equivalent oncologic outcomes to the classic resection. Today, both classic and pylorus-preserving variants are performed.
Indications
The Whipple is the only potentially curative operation for cancers involving the pancreatic head region. Common indications include:
| Category | Specific Conditions |
|---|---|
| Malignant | Pancreatic ductal adenocarcinoma (head/uncinate), ampullary carcinoma, distal cholangiocarcinoma, duodenal adenocarcinoma |
| Premalignant | IPMN with high-grade dysplasia, mucinous cystic neoplasm |
| Benign | Chronic pancreatitis (head-predominant disease after failed other procedures), pancreas divisum with failed minor papilla sphincteroplasty, periampullary neuroendocrine tumors |
| Trauma | Pancreatic head / duodenal C-loop destruction from penetrating trauma |
Resectability requires that the tumor does not encase the superior mesenteric artery (SMA), celiac axis, or hepatic artery. Involvement of the superior mesenteric vein (SMV) or portal vein does not automatically preclude resection - venous resection and reconstruction is feasible at high-volume centers. - Schwartz's Principles of Surgery, 11th Ed.
Preoperative Assessment
- High-quality CT scan (pancreatic protocol) is essential for staging and assessing vascular involvement
- Kocher maneuver assessment: inability to palpate a plane between tumor and the SMA pulsation suggests arterial involvement and unresectability
- Diagnostic laparoscopy may reveal liver metastases or peritoneal disease before committing to laparotomy
- Neoadjuvant therapy (FOLFIRINOX or gemcitabine-based) is increasingly used for borderline-resectable disease; operations after neoadjuvant therapy are more complex due to adhesions and fibrosis
Operative Steps
Resection Phase
- Kocherization - mobilize duodenum and pancreatic head off the inferior vena cava and aorta; assess the SMA directly
- Enter the lesser sac, identify the inferior border of the pancreas; trace the right gastroepiploic vein and middle colic vein to the SMV
- Create the SMV-portal vein tunnel under the pancreatic neck
- Dissect the porta hepatis; ligate and divide the right gastric artery and gastroduodenal artery (confirm the proper hepatic artery pulse is preserved before ligation - a replaced right hepatic artery must be identified first)
- Divide the common hepatic duct; remove gallbladder and cystic duct
- Divide the stomach (distal 30-40% in classic; 2 cm distal to pylorus in pylorus-preserving)
- Divide the jejunum 10-15 cm distal to the ligament of Treitz; pass the proximal jejunum under the mesenteric vessels to the right
- Dissect the uncinate process off the right border of the SMA, ligating fragile venous branches off the SMV
- Divide the pancreatic neck
Reconstruction Phase (in order)
The classic reconstruction uses a single Roux-en-Y jejunal limb with three anastomoses:
- Pancreaticojejunostomy (or pancreaticogastrostomy) - performed first; technique choice (duct-to-mucosa vs. invagination) depends on duct size and pancreatic texture; soft glands with small ducts carry highest fistula risk
- Choledochojejunostomy ~10 cm downstream - end-to-side, single layer interrupted sutures
- Duodenojejunostomy or gastrojejunostomy ~10-15 cm further downstream - two-layer technique; antecolic placement lowers delayed gastric emptying risk compared to retrocolic
- Schwartz's Principles of Surgery, 11th Ed.; Mulholland & Greenfield's Surgery, 7th Ed.
Classic vs. Pylorus-Preserving
| Feature | Classic Whipple | Pylorus-Preserving (PPPD) |
|---|---|---|
| Gastric resection | Distal 30-40% of stomach | Preserves pylorus and ~2 cm proximal duodenum |
| Reconstruction | Gastrojejunostomy | Duodenojejunostomy |
| Oncologic equivalence | Yes | Yes |
| DGE rate | Comparable | Comparable |
| Nutritional outcomes | Similar long-term | Similar |
Complications
Operative mortality at high-volume centers (>15 PD/surgeon/year) is <5%. Morbidity remains high.
Major Complications (ISGPS Definitions)
1. Pancreatic Fistula / Postoperative Pancreatic Fistula (POPF)
- Most common major complication: 10-30% overall
- Risk factors: soft pancreatic texture, small pancreatic duct diameter (<3 mm), high intraoperative blood loss
- Grade B: managed with drainage, antibiotics, somatostatin analogues
- Grade C: rarely requires surgical re-exploration
- Drain amylase thresholds guide drain removal (300 IU/L at day 1, 150 at day 3, 50 at day 5)
- Pancreaticogastrostomy vs. pancreaticojejunostomy show no significant difference in fistula rates in prospective randomized trials
2. Delayed Gastric Emptying (DGE)
- Occurs in 10-15% (Sabiston) to 19% (Maingot's)
- Pathophysiology is multifactorial and incompletely understood
- Treatment: conservative; IV erythromycin may help acutely; ruled out mechanical obstruction by contrast study
- ERAS protocols have reduced DGE incidence by nearly half
3. Postpancreatectomy Hemorrhage (PPH)
- Less common (~5%) but most dreaded - associated with high mortality
- Can occur early (anastomotic) or late (erosion by pancreatic fistula)
4. Biliary Leak
- Managed with wide drainage; endoscopy generally avoided in early postoperative period
- Sabiston Textbook of Surgery; Schwartz's Principles of Surgery, 11th Ed.; Maingot's Abdominal Operations
Vascular Resection
For tumors involving the SMV/portal vein, en bloc venous resection and reconstruction is acceptable at high-volume centers, particularly after neoadjuvant therapy. A systematic review of 28 retrospective studies confirmed acceptable morbidity, mortality, and survival. Arterial resection (SMA, celiac) remains controversial and is associated with significantly higher morbidity - only pursued at expert centers when frozen section confirms fibrosis rather than viable tumor. - Schwartz's Principles of Surgery, 11th Ed.
Minimally Invasive Approaches
Laparoscopic and robotic pancreaticoduodenectomy are increasingly performed. Early data show:
- Feasibility with comparable outcomes to open surgery at expert centers
- Robotic platforms may facilitate vascular dissection
- A 2024 systematic review and meta-analysis (PMID: 39153714) found robotic-assisted PD to be cost-effective with comparable long-term oncologic outcomes to open surgery
Oncologic Outcomes
- Pancreatic ductal adenocarcinoma: median survival after resection approximately 20-24 months; 5-year survival ~20-25% with negative margins and negative nodes
- Ampullary and distal bile duct cancers have considerably better prognosis after resection
- FOLFIRINOX is the current first-line regimen for metastatic/unresectable disease; single-agent gemcitabine is used in patients with poor performance status
Postoperative Care (ERAS)
- Remove nasogastric tube POD 1-2; advance diet over several days
- Early mobilization to prevent DVT and ileus
- Avoid hyperglycemia; maintain near-zero fluid balance
- Early drain removal based on drain amylase levels
- Epidural or TAP blocks + PCA for pain; epidural-associated hypotension may require fluid
- Sabiston Textbook of Surgery
Recent Evidence
- Octogenarian outcomes meta-analysis (PMID: 39266363, HPB 2024): systematic review of PD in patients 80+ - useful for counseling elderly patients on risk
- Robotic vs. open PD meta-analysis (PMID: 39153714, J Gastrointest Surg 2024): robotic approach is cost-effective with equivalent oncologic outcomes
- Postoperative nutritional support Cochrane review (PMID: 40084692, 2025): network meta-analysis on nutritional strategies after PD
Key point: Volume-outcome relationships are among the strongest in surgery for pancreaticoduodenectomy. Patients should be referred to centers performing >20 PDs/year (or individual surgeons with >15/year) where mortality drops to under 5%. - Schwartz's Principles of Surgery, 11th Ed.
Operative steps
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have comprehensive step-by-step operative detail from Fischer's Mastery of Surgery (8th ed). Now I can construct a thorough answer.
Whipple Procedure - Operative Steps in Detail
Source: Fischer's Mastery of Surgery, 8th Ed.; Schwartz's Principles of Surgery, 11th Ed.; Maingot's Abdominal Operations
The operation divides into two phases: Resection (Steps 1-6) and Reconstruction (Steps 7-9).
RESECTION PHASE
Step 1 - Entry into the Lesser Sac and Identification of the Inferior Border of the Pancreas
- Enter the lesser sac by separating the omentum from the transverse colon along the avascular areolar plane; posterior stomach wall confirms entry
- Identify the gastrocolic trunk (trunk of Henle) at the base of this plane - it gives rise to the right gastroepiploic vein, right colic vein, and anterior superior/inferior pancreaticoduodenal veins. Aggressive retraction here can tear this trunk and cause SMV laceration
- If possible, ligate the gastrocolic trunk while preserving the colic veins; this exposes the infrapancreatic SMV
- Mobilize the hepatic flexure of the colon off the duodenum and uncinate process
- For uncinate tumors, extensive SMV involvement, or anticipated venous resection - perform a full Cattell-Braasch maneuver: mobilize the entire right colon and small bowel to the ligament of Treitz (LOT), retracting cephalad to expose the root of the mesentery and 3rd/4th portions of duodenum
- Incise the retroperitoneum at the inferior border of the pancreas and trace toward the SMV
- Begin the retropancreatic tunnel anterior to the SMV from below - if inflammation prevents this, defer until later
Pitfall: Varices in the omentum or colon mesentery suggest SMV-portal vein occlusion missed on preoperative imaging.
Step 2 - Extended Kocher Maneuver
- Incise the lateral peritoneal attachments of the duodenum
- Mobilize the duodenum and pancreatic head medially off the inferior vena cava and aorta
- Continue the Kocher maneuver to the level of the left renal vein - this is the "extended" Kocher
- Allows bimanual palpation: the surgeon's hand under the head/uncinate palpates the relationship of tumor to the SMA. If no plane of normal tissue is felt between the mass and the arterial pulsation, the SMA is likely involved and resection is unlikely to achieve clear margins
- Also identifies the third portion of the duodenum and gives access to the origin of the SMA from below
Step 3 - Portal Dissection
- Identify aberrant hepatic arterial anatomy from preoperative imaging before starting portal dissection - a replaced right hepatic artery (RHA) from the SMA takes a posterior/lateral course and is vulnerable during this step
- Perform cholecystectomy using a top-down approach; identify the cystic artery and cystic duct
- Encircle and dissect the common bile duct (CBD) off the portal vein
- Divide the CBD above the cystic duct junction with electrocautery; cauterize the 3 o'clock and 9 o'clock vessels supplying the duct
- Obtain bile cultures at time of transection to guide antibiotics if deep surgical site infection occurs
- Oversew the distal segment; temporarily occlude the proximal hepatic duct with a Bulldog clamp
- Elevate the distal CBD and lymphatic tissue off the portal vein - small portal venous branches may be avulsed here causing significant hemorrhage
- Carry the anterior portal vein dissection to the level of the pancreatic neck
- Complete the retropancreatic tunnel from above, after portal dissection, to connect with the inferior approach from Step 1; confirm tunnel patency with a finger or blunt clamp
Critical: Before ligating the gastroduodenal artery (GDA), clamp it temporarily and confirm the proper hepatic artery pulse is maintained - if the pulse diminishes, a replaced right or common hepatic artery may arise from the GDA or be at risk. Ligate and divide the GDA only after this confirmation.
Step 4 - Transection of the Stomach or Pylorus
Classic Pancreaticoduodenectomy (antrectomy):
- Perform antrectomy dividing along the lesser curve between the 3rd and 4th transverse veins
- Create a window on the greater curve toward the left gastroepiploic vein
- Divide with a GIA stapler
- If an accessory or replaced left hepatic artery arises from the left gastric artery, divide only the terminal gastric branches - do not divide the main trunk
Pylorus-Preserving Pancreaticoduodenectomy (PPPD):
- Divide the duodenum approximately 2 cm distal to the pylorus with a linear stapler
- Used with caution for tumors close to the pylorus or duodenum
- Equivalent oncologic outcomes to classic resection in most settings
Step 5 - Division of the Jejunum and Proximal Mesentery
- Divide the jejunum 10-15 cm distal to the ligament of Treitz with a linear stapler
- Divide the jejunal mesentery to this point
- Pass the proximal jejunum and 4th portion of duodenum under (posterior to) the superior mesenteric vessels to the right side - this is the roux limb that will be used for reconstruction
Step 6 - Division of the Pancreatic Neck and Uncinate Process Dissection
This is the most critical step oncologically.
- Place hemostatic sutures along the superior and inferior transection lines of the pancreatic neck (above the portal vein/SMV)
- Divide the pancreatic neck with electrocautery
- Once the neck is divided, the portal vein, SMV, and splenic vein are fully exposed
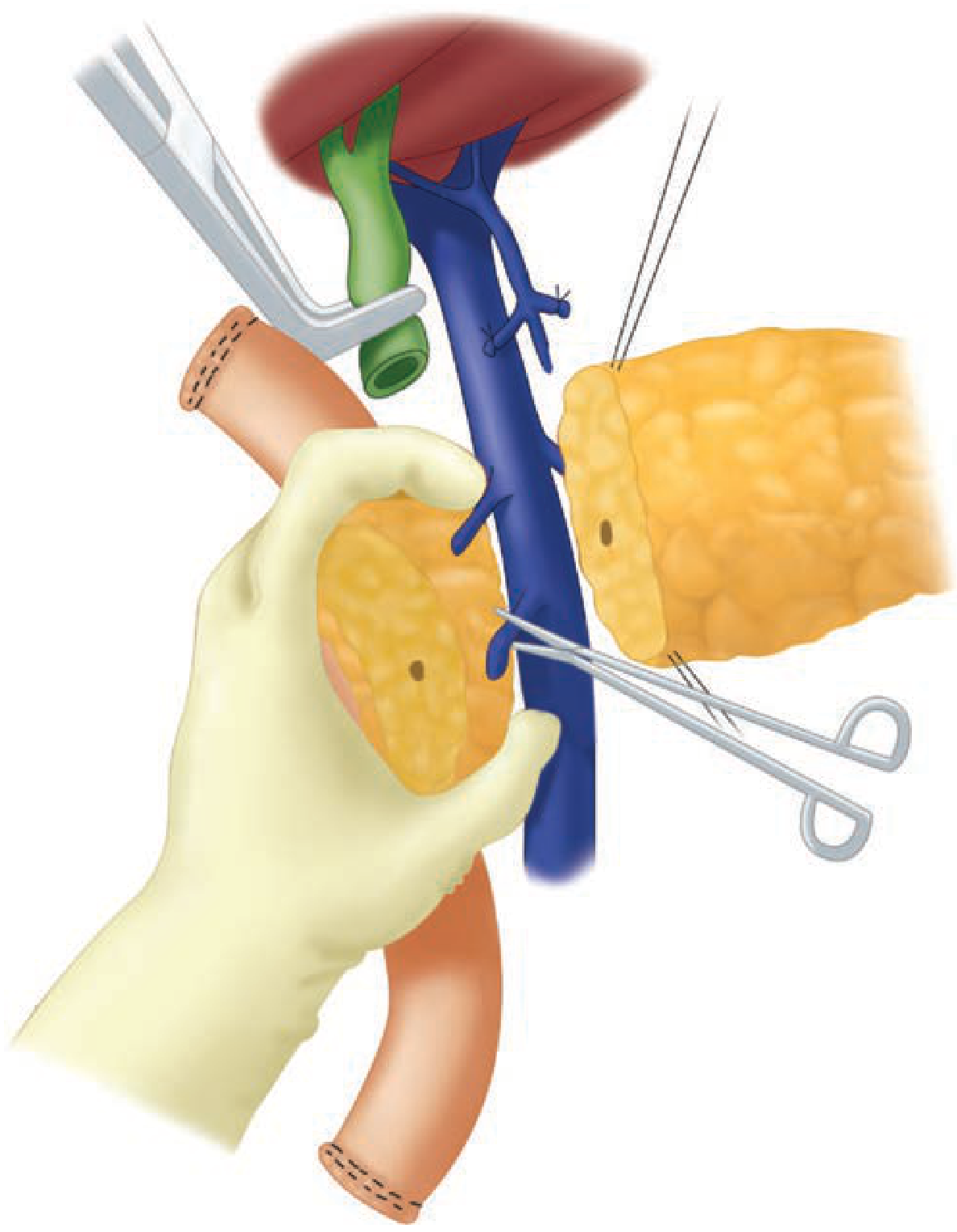
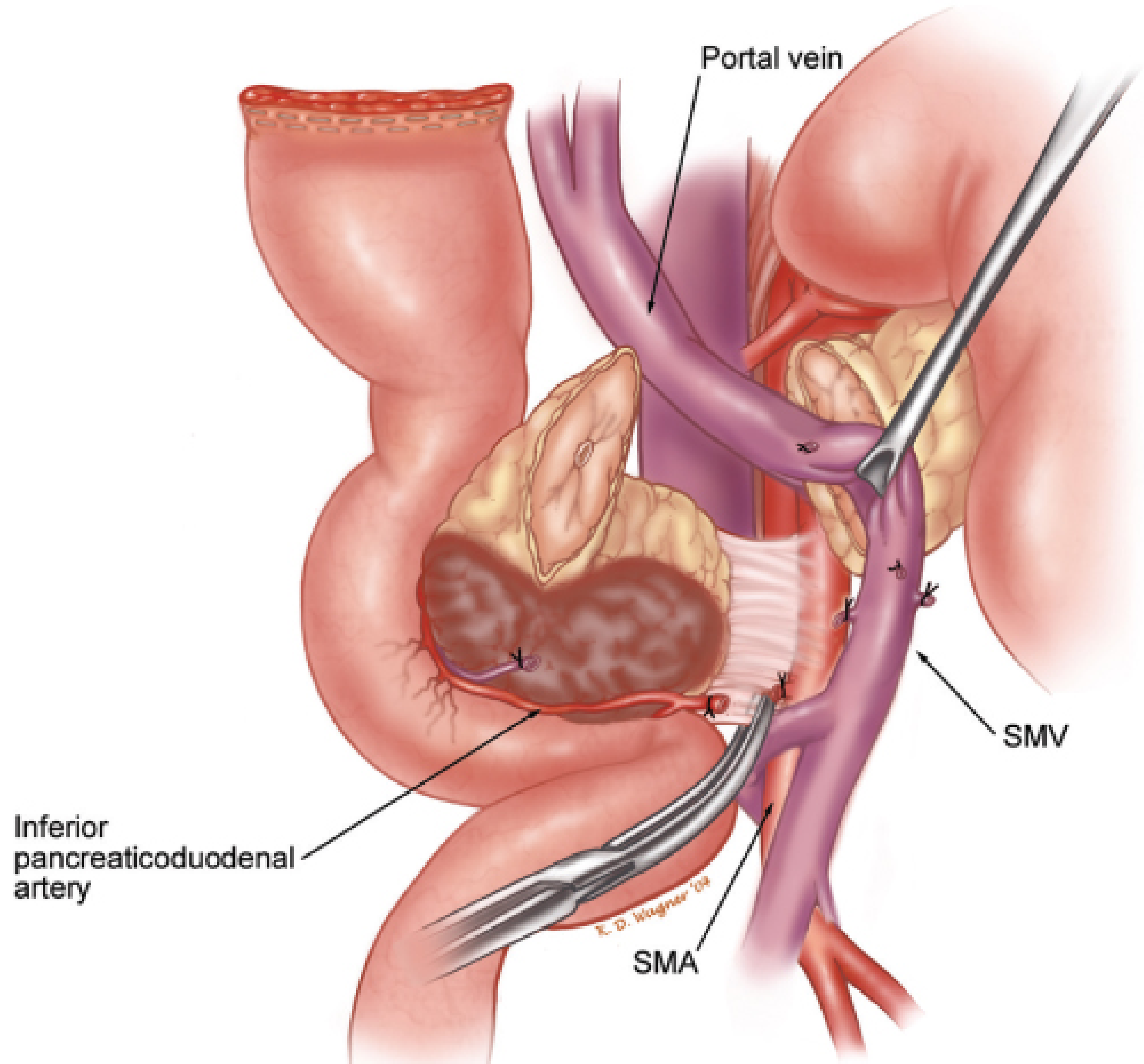
- Mobilize the SMV and carefully ligate small venous branches from the pancreatic head and uncinate process entering the right lateral wall of the SMV/portal vein - these include the superior and inferior pancreaticoduodenal veins and the right gastroepiploic vein
- Retract the SMV medially (to the patient's left) to expose the SMA below
- Develop a periadventitial plane along the SMA and carry it in a caudal-to-cranial direction; all fibrofatty, lymphatic, and perineural tissue to the right of the SMA is taken with the specimen (this is the oncologically important retroperitoneal margin)
- Individually identify, ligate, and divide the inferior pancreaticoduodenal artery (IPDA) with suture ligation - do not include large amounts of surrounding soft tissue (risk of suture slippage and postoperative hemorrhage)
- Free the uncinate process from behind the SMV and bring it with the specimen
Replaced RHA pitfall: If a replaced RHA or CHA arises from the SMA, trace it from the SMA to the porta before dividing the IPDA - avoid injury during this retroperitoneal dissection.
Bleeding control: During retroperitoneal dissection, if bleeding is encountered, direct anterior compression is ineffective. Instead, hold the specimen with the left hand - fingers posterior, thumb anterior - to compress and control hemorrhage.
- Send frozen section margins: pancreatic neck, bile duct, and SMA soft tissue margin. Wait for results before reconstruction; achieve meticulous hemostasis during this interval.
RECONSTRUCTION PHASE
Three anastomoses are performed in sequence on a single Roux-en-Y jejunal limb, in order from proximal to distal:
Step 7 - Pancreatic Anastomosis (Pancreaticojejunostomy)
- Elevate the pancreatic remnant off the splenic vein and retroperitoneal attachments for ~2 cm; preserve small branches to the splenic vein and artery where possible to avoid devascularizing the stump
- Bring the divided jejunum through a window in the transverse colon mesentery to the left of the middle colic vessels (retrocolic); or through the LOT defect (robotic technique). Close the mesocolon defect to prevent internal hernia
- Assess the pancreatic duct size - if soft gland, small duct, or eccentric duct, use a 5-Fr pediatric feeding tube stent trimmed to ~5 cm. Administer secretin if the duct is not immediately visible
- Technique: two-layer end-to-side duct-to-mucosa anastomosis
- Outer posterior row: interrupted 3-0 silk between pancreatic capsule and seromuscular bowel
- Small enterotomy made with needle-tip electrocautery (size matched to duct - avoid oversizing)
- Inner posterior row: interrupted 5-0 monofilament absorbable, full-thickness duct-to-jejunum bites; knots tied inside
- Insert stent at this point if used; secure to duct with a single absorbable suture
- Anterior inner row: complete duct-to-mucosa bites, knots outside
- Outer anterior row: interrupted 3-0 silk, capsule to seromuscular layer
- Suture tying technique: push the bowel to the pancreas - firm but gentle; follow needle curve to avoid tearing soft parenchyma
Step 8 - Biliary Anastomosis (Hepaticojejunostomy)
- Create an end-to-side hepaticojejunostomy approximately 10 cm downstream from the pancreatic anastomosis (modified Blumgart-Kelley technique)
- Use interrupted 4-0 or 5-0 absorbable monofilament sutures (running acceptable only with dilated duct, but interrupted preferred to avoid purse-stringing and stricture)
- Allow the jejunal limb to lay without tension before choosing the enterotomy site
- Place anterior and corner sutures on the bile duct first to open and expose the duct; clamp with needle in place
- Complete posterior row, tie down; then complete anterior layer with full-thickness jejunal bites
- After the anastomosis, tack the jejunum to the mesocolon with interrupted sutures to take tension off the limb
Step 9 - Gastrointestinal Anastomosis (Gastrojejunostomy or Duodenojejunostomy)
- Create anastomosis 20-30 cm distal to the hepaticojejunostomy (if too close, risk of retrograde reflux into the afferent limb causing cholangitis)
- Classic PD: gastrojejunostomy using Billroth II technique, antecolic position preferred (antecolic reduces DGE risk compared to retrocolic)
- PPPD: duodenojejunostomy, stapled or hand-sewn; also antecolic
- Place the anastomosis posteriorly along the dependent greater curvature to optimize gastric emptying
Closure
- Ensure meticulous hemostasis especially in the retroperitoneum (hard to access post-reconstruction)
- Place closed-suction drains near the pancreatic anastomosis and biliary anastomosis
- Fascia closed with running mass closure; skin closed per surgeon preference
Critical Anatomical Hazards at Each Step
| Step | Key Hazard |
|---|---|
| Lesser sac entry | Tear of gastrocolic trunk → SMV laceration |
| Kocher maneuver | IVC, right ureter injury |
| Portal dissection | Replaced RHA from SMA; avulsion of small portal branches |
| GDA ligation | Ligation of replaced/accessory RHA; confirm hepatic pulse before ligation |
| Uncinate dissection | SMA injury; IPDA suture slippage → delayed hemorrhage |
| Reconstruction | Soft small-duct pancreas = high fistula risk; tension on anastomoses |
Variant: Artery-First Approach (for borderline/venous involvement)
When tumor is adherent to the right lateral wall of the SMV-PV and medial retraction is not possible, an artery-first technique is used:
- Encircle the proximal PV and distal SMV with vessel loops
- Retract the SMV laterally (to the patient's right) instead of medially
- The SMA is then seen below; uncinate cleared from the artery first before managing the vein
- Venous resection and primary anastomosis (or graft) is then completed as a defined last step, reducing warm ischemia time to the minimum
- Fischer's Mastery of Surgery, 8th Ed.; Schwartz's Principles of Surgery, 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.