Pott spine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Pott disease" OR "tuberculous spondylitis"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook content from Campbell's Operative Orthopaedics (2026), Robbins Pathology, Adams & Victor's Neurology, and S. Das Clinical Surgery. Here is the full, integrated answer:
Pott's Disease (Tuberculous Spondylitis / Spinal Tuberculosis)
Pott's disease is tuberculous osteomyelitis of the spine, first described by Sir Percival Pott in 1779. Despite molecular evidence of the disease dating to 3000 BCE, it remains globally relevant today.
Epidemiology
- Global TB incidence exceeds 10 million cases/year with 1.3 million deaths/year; 1.2 million cases occur in children annually
- Musculoskeletal TB accounts for ~10% of all TB cases; spinal involvement is present in half of these (i.e., ~5% of all TB)
- The spine is involved in 40% of mycobacterial osteomyelitis cases overall
- Males and females are almost equally affected; incidence increases with age
- Site distribution: Thoracolumbar junction > lumbar spine > cervical spine
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 2566
Pathogenesis
- Primary infection - usually pulmonary TB (occasionally gastrointestinal or lymph node)
- Hematogenous spread to the vertebral body (metaphyseal equivalent - subchondral bone near the disc)
- Alternatively, direct extension from tracheobronchial lymph nodes into adjacent vertebrae
- An infectious endarteritis causes bone necrosis and collapse
- Infection spreads beneath and along the anterior and posterior longitudinal ligaments, leading to subligamentous spread to adjacent vertebral bodies - this explains the "skip lesions" seen on imaging
- In adults, the intervertebral disc is initially spared (avascular in adults; a key distinction from pyogenic infection); in children, the disc may be involved early
- Abscesses form, expand with necrotic debris, may track along fascial planes, and can drain spontaneously forming sinus tracts (cold abscesses)
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 2566; Robbins & Cotran Pathologic Basis of Disease p. 1094
Pathology
- Histology: Caseating granulomas with acid-fast bacilli (Langhans giant cells, epithelioid macrophages, lymphocytes, central caseous necrosis)
- Progressive anterior vertebral body destruction leads to:
- Gibbus deformity (sharply angulated kyphosis) - the hallmark deformity
- Vertebral collapse and compression fractures
- Paravertebral/cold abscess formation
- Epidural extension - more likely to cause permanent neurologic damage than the bony deformity alone
- Disc destruction + vertebral collapse = permanent scoliosis/kyphosis

Clinical Features
Constitutional symptoms (early, predominant)
- Weakness, malaise, night sweats, fever, weight loss
- ESR is invariably elevated (though normal in >50% in some series)
- Anemia and hypoproteinemia
Local symptoms
- Back pain in 70% at presentation - often months to years after symptom onset
- Progressive pain is a late symptom associated with bone collapse
- Cold abscess / intermittent draining sinuses
- Psoas abscess - tracks down from thoracolumbar disease under the psoas fascia to present as a swelling in the femoral triangle; reducible, gives impulse on coughing, painless, lateral to the femoral artery
- Retropharyngeal abscess - from cervical involvement; can cause hoarseness (recurrent laryngeal nerve), dysphagia, respiratory stridor; rarely, sudden death from erosion into great vessels
Neurological deficits
- Pott's paraplegia - spinal cord compression caused by:
- The kyphotic deformity itself (mechanical)
- Epidural abscess (pus or caseous granulation tissue extruding from infected vertebra) - the more common cause
- Pial arteritis with cord infarction (rare)
- ~30% of patients in less-developed countries present with neurologic deficits; less common in developed countries
- Neurological signs may wax and wane
- Motor function and rectal tone are good prognostic predictors
- Adams & Victor's Principles of Neurology 12th Ed, p. 1253; Campbell's Operative Orthopaedics 15th Ed 2026, p. 2567; S. Das Manual on Clinical Surgery 13th Ed
Key Distinguishing Feature vs. Pyogenic Spondylodiscitis
| Feature | Pott's Disease (TB) | Pyogenic Spondylodiscitis |
|---|---|---|
| Disc involvement | Spared early (adults) | Early disc destruction |
| Bone destruction | Anterior body, multifocal (skip lesions) | Usually contiguous |
| Abscess | Cold abscess | Warm/hot abscess |
| Onset | Insidious (months-years) | Acute/subacute |
| Organism | M. tuberculosis | S. aureus, gram-negatives |
Investigations
Laboratory
- CBC: anemia; raised ESR and CRP (though ESR may be normal in >50%)
- Tuberculin skin test: contraindicated in suspected reactivation (risk of intense skin reaction/slough)
- Interferon-gamma release assay (IGRA) preferred
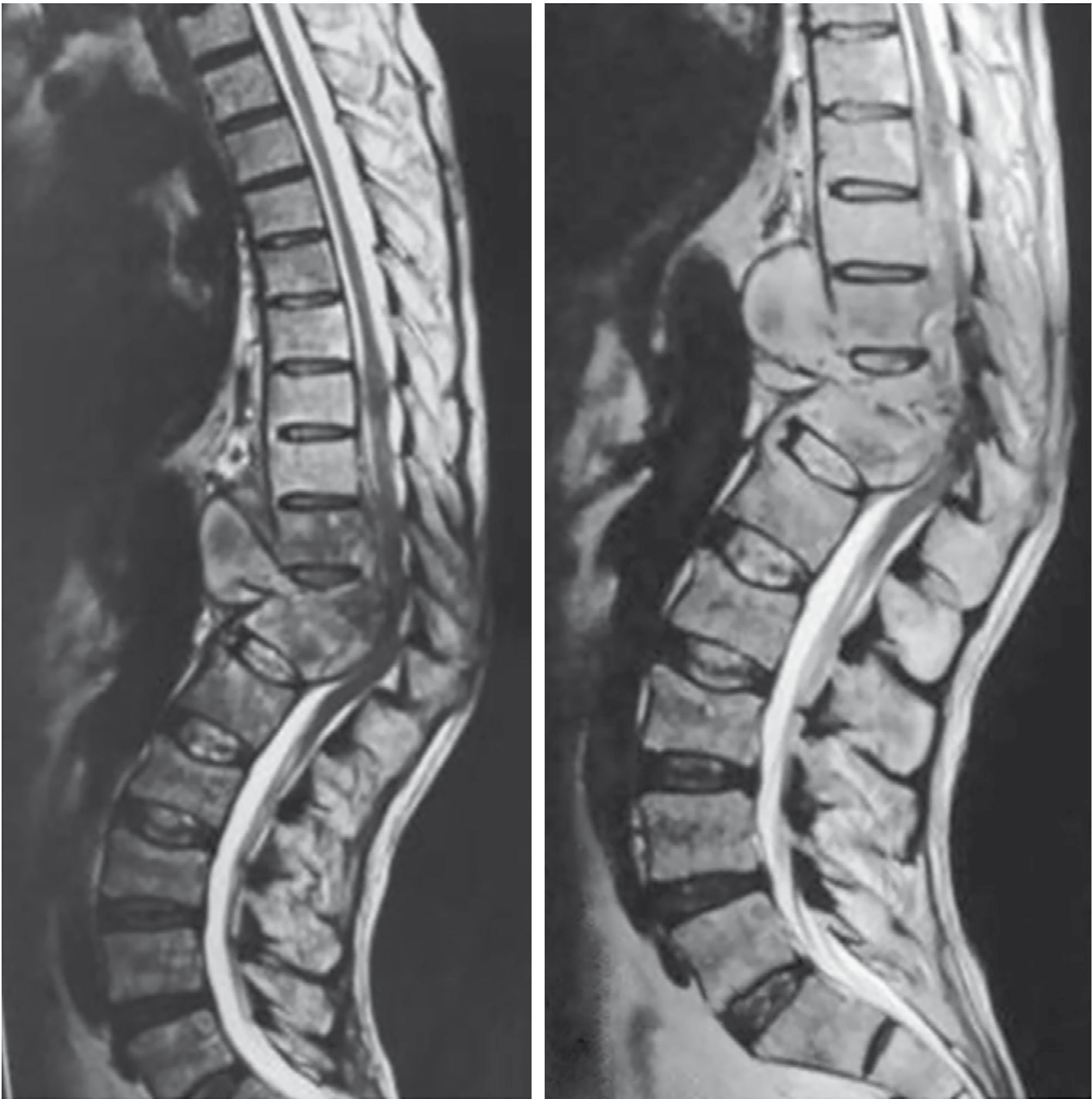
Imaging
- Plain X-ray (early): subtle decrease in disc space height, localized osteopenia
- CT: bone destruction, paraspinal abscess
- MRI with and without contrast (preferred): best for demonstrating epidural abscess, cord compression, extent of disease, and skip lesions - entire spine should be imaged
Definitive diagnosis
- Culture of biopsy specimen or PCR/rapid molecular testing (also detects drug resistance)
- Percutaneous CT-guided biopsy is usually adequate
- Open biopsy if needle biopsy is dangerous or nonproductive
Differential diagnosis: Pyogenic/fungal infection, metastases, primary bone tumors (osteosarcoma, chondrosarcoma, myeloma, eosinophilic granuloma, ABC), sarcoidosis, Scheuermann disease
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 2567
Treatment
Medical Management (first-line for most cases)
- Multi-drug anti-tuberculous therapy (ATT):
- HRZE regimen: Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E), +/- Streptomycin
- Duration: 6 months in immunocompetent patients; 18-24 months in HIV/immunocompromised or drug-resistant cases
- With early diagnosis and medical treatment, 80% of cases achieve bony fusion
- Drug-resistant TB (MDR-TB) benefits more from surgical treatment
- Outcomes are generally good; neurologic deficits often improve
Surgical Treatment
Indications:
- Neurologic deficit (compressive myelopathy)
- Severe kyphosis (>40-60° depending on level)
- Pain from spinal instability
- Failure of medical therapy
- Large paraspinal or epidural abscess
- More than four levels of vertebral involvement
Pre-operative preparation:
- ATT for at least 2-4 weeks preoperatively to suppress infection
- Nutritional support
- Manage comorbidities (hypertension, diabetes)
- Full-spine MRI to identify all involved levels including skip lesions
Surgical options:
- Anterior debridement + fusion (Hodgson-Stock operation, 1956) - gold standard historically; allows direct debridement of anterior disease
- Posterior stabilization with instrumented fusion
- Combined anterior-posterior approach for severe deformity
- Cervical approach: Drainage of retropharyngeal abscess via posterior triangle or anterior cervical approach; allows bony reconstruction
- External stabilization alone (+ long-term ATT) may give excellent results in some patients, particularly when surgery is refused
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 2567-2568; Adams & Victor's Principles of Neurology 12th Ed, p. 1253
Complications
| Complication | Notes |
|---|---|
| Gibbus deformity | Sharply angulated kyphosis; cosmetically and mechanically significant |
| Pott's paraplegia | Cord compression from deformity or epidural abscess |
| Cold/psoas abscess | Tracks along fascial planes; may present distant to spine |
| Sinus tract formation | Draining cold abscess; risk of secondary pyogenic infection |
| Secondary amyloidosis | From chronic infection |
| Respiratory compromise | Severe thoracic kyphosis reducing lung volumes |
| Sudden death | Rare; from cervical disease eroding great vessels |
Summary Mnemonic - POTT'S
- P - Paraplegia (Pott's paraplegia - the feared complication)
- O - Osteomyelitis (tuberculous, anterior vertebral body)
- T - Thoracolumbar (most common site)
- T - Tuberculosis (hematogenous spread from pulmonary focus)
- S - Skip lesions + Subligamentous spread + Spared disc (early)
Recent evidence note: A 2026 systematic review (PMID 42140478) on chronic spinal infections confirms that TB remains the dominant etiology globally, with emerging concerns about drug-resistant strains influencing both diagnostic and treatment algorithms.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Robbins & Cotran Pathologic Basis of Disease | Adams & Victor's Principles of Neurology 12th Ed | S. Das Manual on Clinical Surgery 13th Ed
This is a shared conversation. Sign in to Orris to start your own chat.