Atelectasis
Reading File
Finding Sources
Searching PubMed
atelectasis
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks plus imaging. Let me compile the full answer.
Atelectasis
Atelectasis (from Greek ateles = incomplete, ektasis = expansion) is the collapse or hypoventilation of lung units - ranging from a few alveoli to an entire lung. It is one of the most common respiratory abnormalities encountered in clinical practice.
Definition
Atelectasis is caused by hypoventilation of lung units and may involve an entire lung, a lobe, segment, or subsegment. When lung units are atelectatic, ventilation-perfusion (V/Q) mismatch leads to hypoxemia. Sustained atelectasis can also lead to infection.
- Goldman-Cecil Medicine, p. 918
Types and Pathophysiology
1. Obstructive (Resorptive) Atelectasis
- Most common type
- Caused by bronchial block to entry of air; gas distal to the obstruction is absorbed into the bloodstream
- Intrinsic obstruction: mucous plugs, foreign bodies, endobronchial tumors
- Extrinsic obstruction: peribronchial lymph node enlargement, mediastinal masses compressing the airway
- Results in retractile consolidation
2. Passive / Relaxation / Compression Atelectasis
- Occurs when the lung recoils to a smaller volume because of fluid (pleural effusion) or air (pneumothorax) in the adjacent pleural space
- The lung collapses away from the chest wall
3. Dependent / Hypostatic Atelectasis
- Lung bases and posterior segments are vulnerable
- Caused by inadequate ventilation, especially in immobilized or postoperative patients
- Gravity-dependent alveolar closure
4. Patchy Atelectasis
- Caused by alveolar filling processes such as hemorrhage and pulmonary edema
- Surfactant dysfunction (e.g., ARDS, neonatal RDS) promotes this pattern
5. Rounded Atelectasis (Folded Lung)
-
Caused by pleural thickening that invaginates and traps adjacent lung
-
Characteristically occurs in dorsal peripheral lower lobes
-
Strongly associated with asbestos-related pleural disease and other chronic pleural diseases
-
Appears as an ovoid mass-like density abutting the pleura
-
Goldman-Cecil Medicine, p. 918; Grainger & Allison's Diagnostic Radiology
Clinical Features
Most cases are asymptomatic and found incidentally on chest imaging. When symptomatic:
| Feature | Details |
|---|---|
| Dyspnea | Proportional to extent of collapse |
| Tachypnea | Common with significant collapse |
| Tachycardia | Reflex response to hypoxemia |
| Low-grade fever | Classic in postoperative atelectasis (within 24-48 h post-op) |
| Hypoxemia | From V/Q mismatch; SpO2 ≤96% on Venturi mask O2 is moderately sensitive for postoperative atelectasis |
| Reduced breath sounds | Over affected area |
- Tintinalli's Emergency Medicine; Goldman-Cecil Medicine
Postoperative Atelectasis - Special Context
This is the most common form encountered clinically. Contributing factors include:
-
Inadequate clearance of secretions after general anesthesia
-
Decreased intra-alveolar pressure
-
Postoperative pain causing splinting and hypoventilation
-
Most frequent after upper abdominal and thoracic surgery
-
Tintinalli's Emergency Medicine
Diagnosis
Chest X-Ray
Plain radiography shows:
- Loss of lung volume
- Displacement of lobar fissures, mediastinum, or diaphragm toward the involved lung (key sign of volume loss)
- Plate-like (discoid/Fleischner lines): horizontal or curvilinear opacities - common with subsegmental atelectasis
- Triangular densities or frank lobar consolidation
Fig. 1 - Right Upper Lobe Atelectasis (CXR)
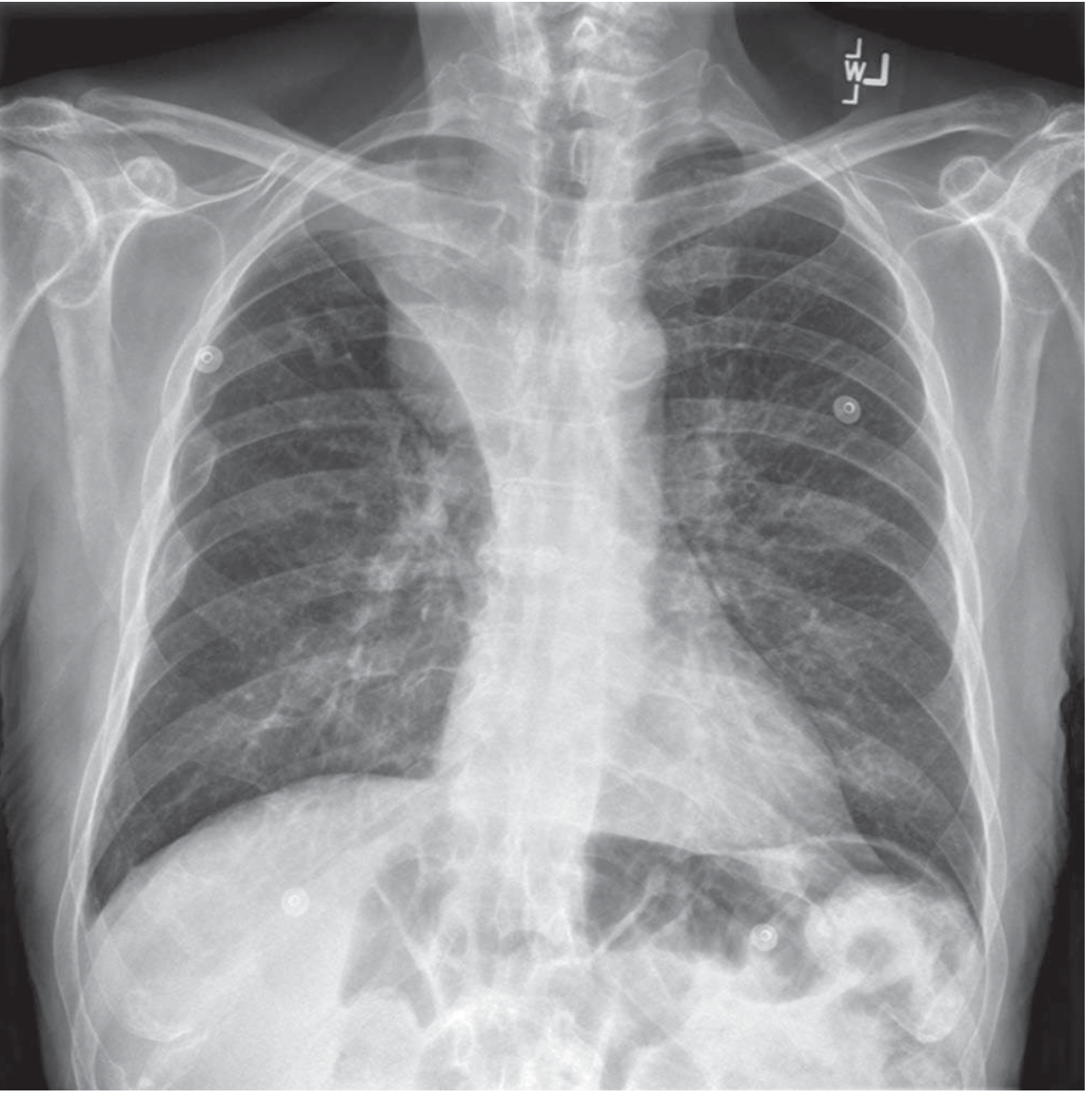 Plain chest radiograph demonstrating right upper lobe atelectasis caused by an endobronchial tumor - Goldman-Cecil Medicine, p. 918
Plain chest radiograph demonstrating right upper lobe atelectasis caused by an endobronchial tumor - Goldman-Cecil Medicine, p. 918
CT Scan
- Demonstrates the type and cause of atelectasis more precisely
- Can differentiate rounded atelectasis from parenchymal tumor
- Key CT features of rounded atelectasis:
- Subpleural location
- "Comet tail" sign - crowding of bronchi and vessels curving from the mass to the hilum
- Strong, homogeneous enhancement after IV contrast (atelectasis enhances; tumor usually does not)
- Stable on serial examinations
Fig. 2 - Rounded Atelectasis (CT)
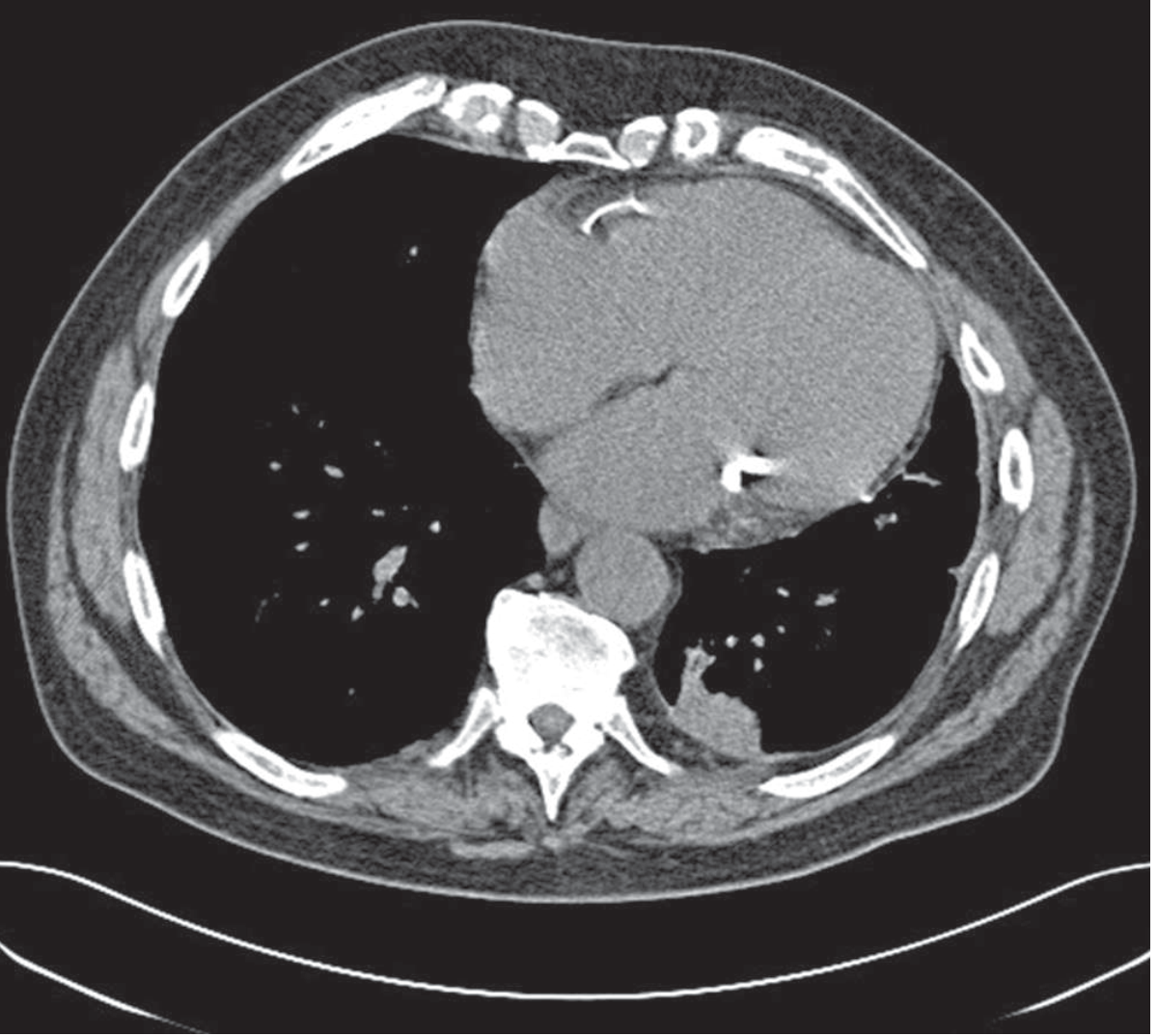 CT image of rounded atelectasis - Goldman-Cecil Medicine, p. 918
CT image of rounded atelectasis - Goldman-Cecil Medicine, p. 918
Fig. 3 - Round Atelectasis - HRCT (axial and sagittal)
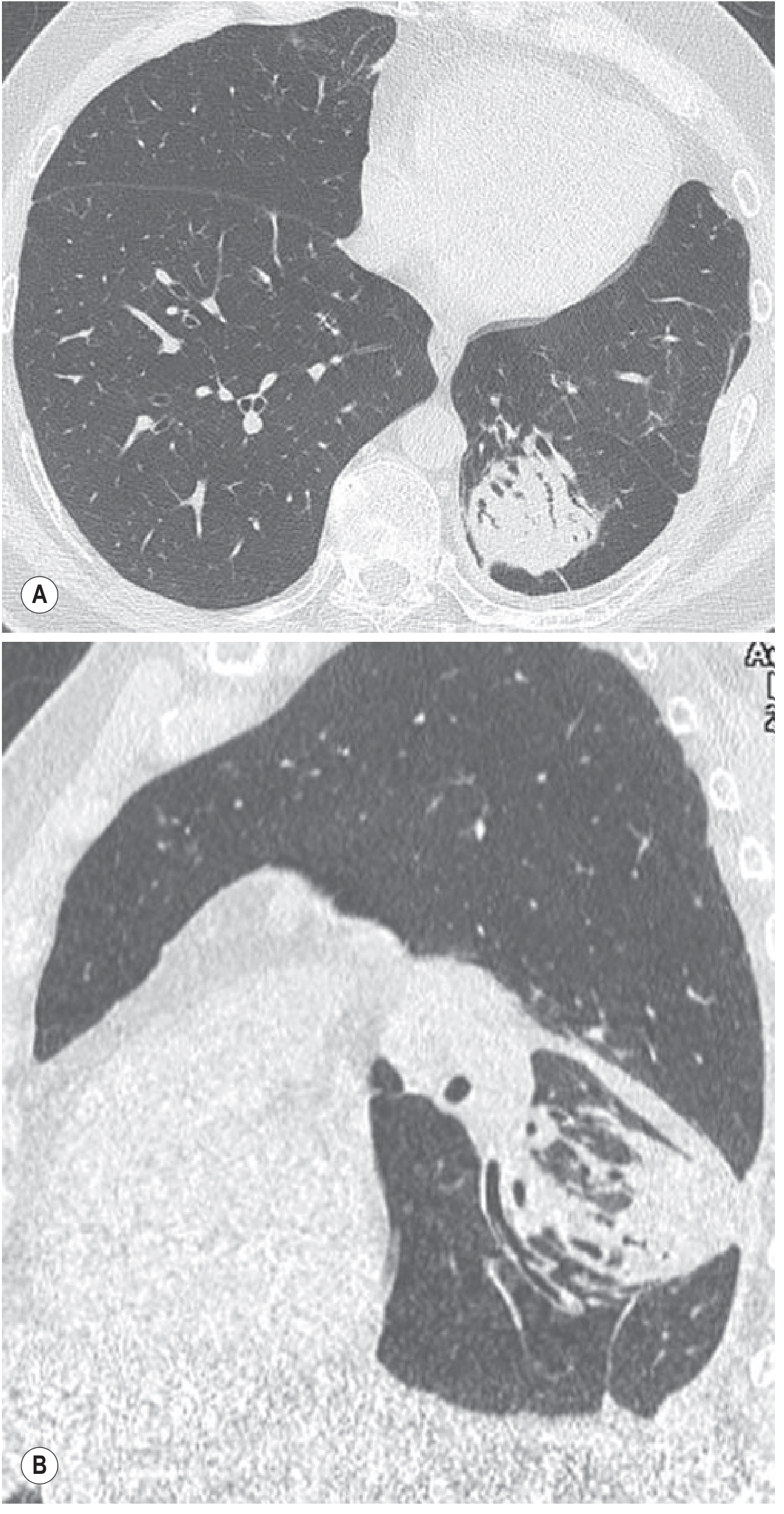 HRCT axial (A) and sagittal reformation (B) showing subpleural consolidation and the curved bronchovascular bundle ("comet tail") toward the atelectasis - Grainger & Allison's Diagnostic Radiology
HRCT axial (A) and sagittal reformation (B) showing subpleural consolidation and the curved bronchovascular bundle ("comet tail") toward the atelectasis - Grainger & Allison's Diagnostic Radiology
Bronchoscopy
- Required to confirm intrinsic vs. extrinsic compression in obstructive-resorptive atelectasis
- Determines the exact pathology of obstruction (tumor vs. mucous plug vs. foreign body)
- Can be therapeutic (mucous plug removal)
Bedside Ultrasound
- Increasingly used to confirm the diagnosis, particularly in ICU/postoperative settings
Treatment
Treatment is directed at the underlying mechanism:
| Type | Treatment |
|---|---|
| Passive/Compression | Drain the pleural space (thoracentesis or chest tube) |
| Obstructive/Resorptive | Bronchoscopy for diagnosis and removal of obstruction; repeated sessions may be needed for mucus plugs |
| Patchy | Treat the underlying parenchymal process (edema, hemorrhage) |
| Rounded | No treatment required; monitor with serial CT to differentiate from neoplasm |
| Dependent/Postoperative | Mobilization, deep breathing exercises, chest physiotherapy |
Prevention and Non-pharmacologic Measures
-
Incentive spirometry: widely prescribed after surgery; however, no RCTs have definitively proven its effectiveness
-
Preoperative inspiratory muscle training and recruitment maneuvers: may reduce atelectasis after upper abdominal and cardiac surgery
-
Prophylactic non-invasive ventilation (NIV): may reduce pulmonary dysfunction after lung resection surgery
-
Positive expiratory pressure (PEP) devices and high-frequency chest wall oscillation: used but of no proven benefit
-
Pain control: essential to enable deep breathing postoperatively
-
Patients with mild atelectasis and no hypoxemia can be managed as outpatients with pain control and encouraged deep breathing
-
Admit if: hypoxemia, underlying lung disease, debilitated patient, or diagnosis uncertain
-
Goldman-Cecil Medicine, p. 918; Tintinalli's Emergency Medicine
Complications
- Hypoxemia - from V/Q mismatch (most common)
- Superimposed infection / pneumonia - from retained secretions in collapsed lung (especially postoperative)
- Bronchiectasis - in CF patients, untreated atelectasis can progress to severe bronchiectasis of the affected segment/lobe
Recent Evidence
A 2026 BMJ meta-analysis (PMID 41956522) examined non-drug perioperative interventions to reduce postoperative pulmonary complications (including atelectasis) after abdominal surgery. A 2024 meta-analysis (PMID 38937217) found that driving pressure-guided ventilation reduces postoperative pulmonary complications in surgical patients. These reinforce lung-protective ventilation strategies as the standard of care.
Sources: Goldman-Cecil Medicine (International Ed.), p. 918 | Tintinalli's Emergency Medicine (9e) | Grainger & Allison's Diagnostic Radiology | Fishman's Pulmonary Diseases and Disorders (2-Vol Set)
This is a shared conversation. Sign in to Orris to start your own chat.