Normal blood pressure range according to age
Reading File
Searching the Web
normal blood pressure range by age 2024 guidelines
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Here is a thorough breakdown of normal blood pressure ranges by age, drawn from medical textbooks and current guidelines (2024 ESC, AHA/ACC).
Blood Pressure: Normal Ranges by Age
What the Numbers Mean
Blood pressure is recorded as systolic / diastolic (mm Hg):
- Systolic - pressure when the heart contracts
- Diastolic - pressure when the heart relaxes between beats
Adults (18+ years)
Per the WHO/ESC and AHA/ACC classifications (the standard used in clinical practice):
| Category | Systolic (mm Hg) | Diastolic (mm Hg) | |
|---|---|---|---|
| Optimal | < 120 | and | < 80 |
| Normal | 120 - 129 | and/or | 80 - 84 |
| High Normal | 130 - 139 | and/or | 85 - 89 |
| Grade 1 Hypertension | 140 - 159 | and/or | 90 - 99 |
| Grade 2 Hypertension | 160 - 179 | and/or | 100 - 109 |
| Grade 3 Hypertension | ≥ 180 | and/or | > 110 |
| Isolated Systolic Hypertension | ≥ 140 | and | < 90 |
Source: Park's Textbook of Preventive & Social Medicine; 2024 ESC Guidelines
Key 2024 update: The 2024 ESC guidelines introduced the category "Elevated BP" (SBP 120-139 or DBP 70-89 mm Hg) to recognize that cardiovascular risk rises continuously across this range, not just at the hypertension threshold. The recommended treatment target for adults on antihypertensive therapy is SBP 120-129 mm Hg (with exceptions for patients >85 years, frailty, or orthostatic symptoms).
Average Blood Pressure by Adult Age Group and Sex
These are average observed values in population studies, not targets:
| Age | Women (avg) | Men (avg) |
|---|---|---|
| 18 - 39 years | 110/68 mm Hg | 119/70 mm Hg |
| 40 - 59 years | 122/74 mm Hg | 124/77 mm Hg |
| 60+ years | 139/68 mm Hg | 133/69 mm Hg |
Note: The fact that average BP rises with age does not mean higher BP is "normal" or acceptable in older adults - the clinical targets still apply.
Children and Adolescents
Pediatric blood pressure is assessed relative to age, sex, and height percentiles - a single fixed number does not apply. Hypertension in children is defined as BP > 95th percentile for age/sex/height on repeated measurements (Brenner & Rector's The Kidney).
Typical ranges and quick clinical formulas:
| Age Group | Systolic (mm Hg) | Diastolic (mm Hg) |
|---|---|---|
| Newborn (up to 1 month) | 60 - 90 | 20 - 60 |
| Infant (1 month - 1 year) | 87 - 105 | 53 - 66 |
| Toddler (1 - 3 years) | 95 - 105 | 53 - 66 |
| Preschooler (3 - 5 years) | 95 - 110 | 56 - 70 |
| School age (5 - 10 years) | 97 - 112 | 57 - 71 |
| Adolescent (10 - 19 years) | 112 - 128 | 66 - 80 |
Quick clinical formula for children ≥ 1 year (Rosen's Emergency Medicine):
- Estimated average SBP = (Age in years × 2) + 90 mm Hg
- Estimated average DBP = ½ × estimated SBP
- Minimum acceptable SBP (5th percentile):
- Newborn to 1 month: 60 mm Hg
- 1 month to 1 year: 70 mm Hg
- 1 - 10 years: (Age × 2) + 70 mm Hg
-
10 years: 90 mm Hg
Summary: What to Aim For
| Life Stage | Target / Optimal BP |
|---|---|
| Children & Adolescents | Based on age/sex/height percentiles; < 90th percentile |
| Adults (18 - 84 years) | < 120/80 mm Hg (optimal); treatment target 120-129 mmHg systolic |
| Older adults (≥ 85 years / frail) | As low as tolerated toward 120-129 mmHg |
Important notes:
- BP should always be measured at least twice, on two separate occasions, to confirm a reading.
- White coat effect (BP higher in clinic), masked hypertension (normal in clinic, high at home), and orthostatic hypotension (drop > 20/10 mm Hg on standing) are all clinically relevant variations.
- Low BP (< 90/60 mm Hg) can also be significant if it causes symptoms such as dizziness or syncope.
Difference in measuring BP in different positions standing, sitting, and supine etc.
Finding Sources
Searching the Web
blood pressure difference positions standing sitting supine lying clinical significance
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Here is a thorough breakdown of how body position affects blood pressure measurement, including the physiology, clinical thresholds, and practical protocols.
Blood Pressure Variation by Body Position
1. The Physiology: Why Position Changes BP
When you change body position, gravity redistributes blood and triggers compensatory autonomic reflexes.
Supine (lying flat):
- Blood is evenly distributed; no hydrostatic gradient pulling blood toward the legs
- Venous return to the heart is maximal
- Cardiac output and stroke volume are at their highest
- BP is relatively stable and often slightly lower than sitting
- The heart and cuff are at the same level - measurements are most standardized
Sitting:
- Moderate venous pooling in the legs
- The baroreceptor reflex (carotid sinus and aortic arch) partially compensates by increasing heart rate and peripheral vascular resistance
- BP is typically ~5-10 mmHg higher than supine in healthy adults
- The standard clinical measurement position recommended by WHO and most guidelines
Standing:
- Blood pools in leg veins (up to 500-800 mL can pool), reducing venous return
- Cardiac output drops via the Frank-Starling mechanism
- Baroreceptor reflex activates: increased sympathetic outflow raises HR and total peripheral resistance
- In a healthy person, BP is restored within 1-2 minutes
- Initially there is a transient dip in BP, then a recovery
"When a person moves from a supine to a standing position, blood pools in the veins of the lower extremities. The capacitance of the veins allows for large blood volumes to accumulate. When blood pools in the veins, venous return to the heart decreases and cardiac output decreases (Frank-Starling mechanism), which results in a decrease in mean arterial pressure."
- Costanzo Physiology, 7th Edition
Cardiovascular responses to standing (summary table from Costanzo):
| Parameter | Initial Response to Standing | Compensatory Response |
|---|---|---|
| Mean arterial pressure | Decreases | Returns toward normal |
| Heart rate | Unchanged initially | Increases |
| Stroke volume | Decreases | Returns toward normal |
| Cardiac output | Decreases | Returns toward normal |
| Total peripheral resistance | Unchanged | Increases |
| Central venous pressure | Decreases | Increases |
2. Typical BP Differences Between Positions (Normal Adults)
| Position | Systolic BP | Diastolic BP | Notes |
|---|---|---|---|
| Supine | Lowest or near-equal to sitting | Slightly lower | Best for standardized research; relaxed state |
| Sitting | ~5-10 mmHg higher than supine | Slightly higher | Standard clinical measurement position |
| Standing | Transient drop, then near-sitting | May rise slightly | Must wait 1-3 min for stabilization |
From Creasy & Resnik's Maternal-Fetal Medicine: "Arterial blood pressures are approximately 10 mm Hg higher in the standing or sitting position than in the lateral or supine position; consistency in position during successive measurements is essential for the accurate documentation of a trend."
3. Orthostatic Hypotension - The Pathological Drop
When the compensatory reflex fails to maintain BP on standing, this is called orthostatic (postural) hypotension.
Definition (consensus standard):
- Systolic BP drop ≥ 20 mmHg within 3 minutes of standing, or
- Diastolic BP drop ≥ 10 mmHg within 3 minutes of standing
- In hypertensive patients: a drop of ≥ 30 mmHg systolic is a more appropriate threshold
- ESC additionally includes a fall in systolic BP to < 90 mmHg
- A pulse rise of > 30 bpm on standing is also a diagnostic criterion
Source: Symptom to Diagnosis, 4th Ed.; Brenner & Rector's The Kidney
Modified threshold when using seated (not supine) baseline:
- A fall of 15/7 mmHg from sitting-to-standing is used instead of 20/10 mmHg, due to reduced sensitivity when the supine baseline is skipped (Brenner & Rector's The Kidney).
4. The Normal Tilt Response vs. Orthostatic Hypotension (Illustrated)
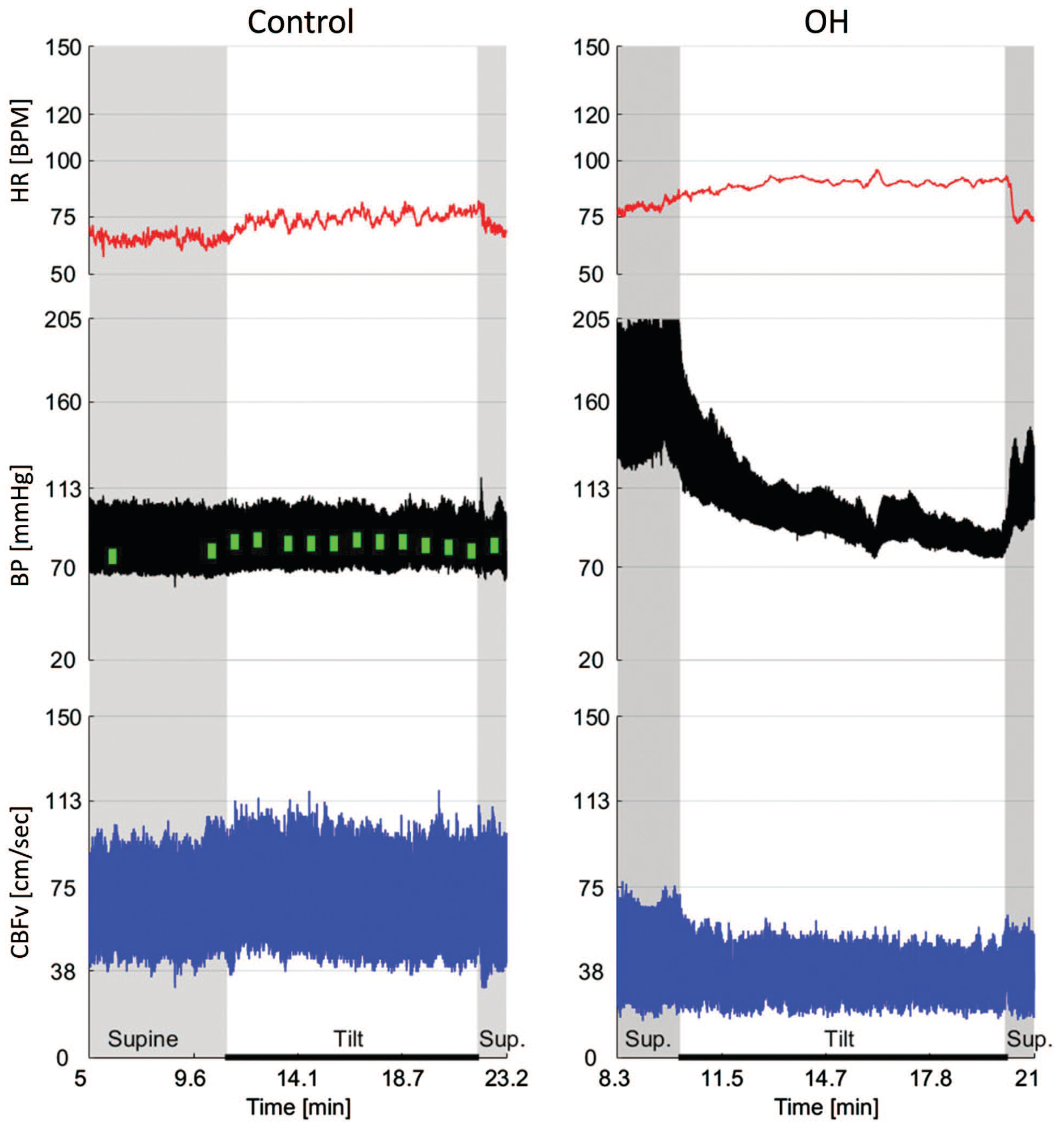
Left: Normal - BP is stable across supine and tilt phases; HR rises modestly. Right: Orthostatic hypotension - supine hypertension is followed by a sharp BP drop on tilting, with HR compensation and reduced cerebral blood flow velocity (CBFV). From Adams and Victor's Principles of Neurology, 12th Ed.
5. Standard Measurement Protocol (Clinical)
Proper technique per Roberts & Hedges' Clinical Procedures in Emergency Medicine:
- Patient lies supine for 2-3 minutes - record BP and pulse
- Patient stands - record BP, pulse, and symptoms at 1 minute (and optionally at 2-3 min)
- Allow immediate return to supine if syncope or near-syncope occurs
Key interpretation rules:
- The supine-to-standing comparison is the most sensitive - if supine BP is not measured, up to 67% of orthostatic cases may be missed
- Sitting-to-standing is acceptable in busy clinical practice but less sensitive
- An increase in pulse of > 30 bpm with standing is highly sensitive (97%) and specific (98%) for large volume blood loss (1-2 units)
- Sensitivity falls dramatically if the patient sits instead of stands (39-78% vs 97%)
- Arm position must be held constant throughout all measurements
6. Who Is Most at Risk for Positional BP Changes?
| Group | Why They Are at Risk |
|---|---|
| Elderly | Decreased baroreceptor sensitivity, reduced vasomotor tone, impaired chronotropic response |
| Diabetics | Autonomic neuropathy impairs sympathetic compensation |
| Hypertensive patients | Paradoxically high rates of orthostatic hypotension (8-34% prevalence) |
| Volume-depleted patients | Hemorrhage, dehydration, vomiting/diarrhea reduce venous reserve |
| On antihypertensives / vasodilators | Drug effect reduces compensatory vasoconstriction |
| Autonomic failure | No tachycardic response to BP drop - a key distinguishing sign |
A key differentiator: orthostatic hypotension from autonomic failure does NOT produce reflex tachycardia, whereas hypotension from volume depletion typically does produce a pronounced tachycardia. (Roberts & Hedges)
7. A Recent Note on Supine BP
A 2023 AHA-highlighted study found that high BP measured only in the supine position (but not in seated) was associated with significantly increased cardiovascular risk - 53% higher risk of coronary heart disease, 62% higher stroke risk, and 34% higher all-cause mortality. This suggests supine BP may reveal hypertension missed in routine office (seated) measurement, though routine clinical protocols have not yet been updated to require supine measurement as standard.
Bottom line: Sitting is the standard position for routine BP measurement. Always measure from the same position for comparison over time. Check standing BP whenever orthostatic hypotension is suspected - especially in the elderly, diabetics, patients on antihypertensives, and anyone with dizziness or syncope on standing.
This is a shared conversation. Sign in to Orris to start your own chat.