Explain the topic of large Blood vessels of the Gut in full detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have all the content I need for a comprehensive, detailed answer. Let me compose the full response.
Large Blood Vessels of the Gut
The gut receives its arterial supply from three major unpaired branches of the abdominal aorta - the celiac trunk, the superior mesenteric artery (SMA), and the inferior mesenteric artery (IMA). Together they account for approximately 20% of cardiac output. Venous drainage passes through the portal system to the liver before returning to the systemic circulation. The arrangement follows the embryological division of the gut into foregut, midgut, and hindgut.
Embryological Basis
The three arterial trunks correspond precisely to the three primitive gut segments:
| Embryological Gut | Artery | Structures Supplied |
|---|---|---|
| Foregut | Celiac trunk | Esophagus (distal) to proximal duodenum |
| Midgut | Superior mesenteric artery | Distal duodenum to proximal 2/3 transverse colon |
| Hindgut | Inferior mesenteric artery | Distal 1/3 transverse colon to upper rectum |
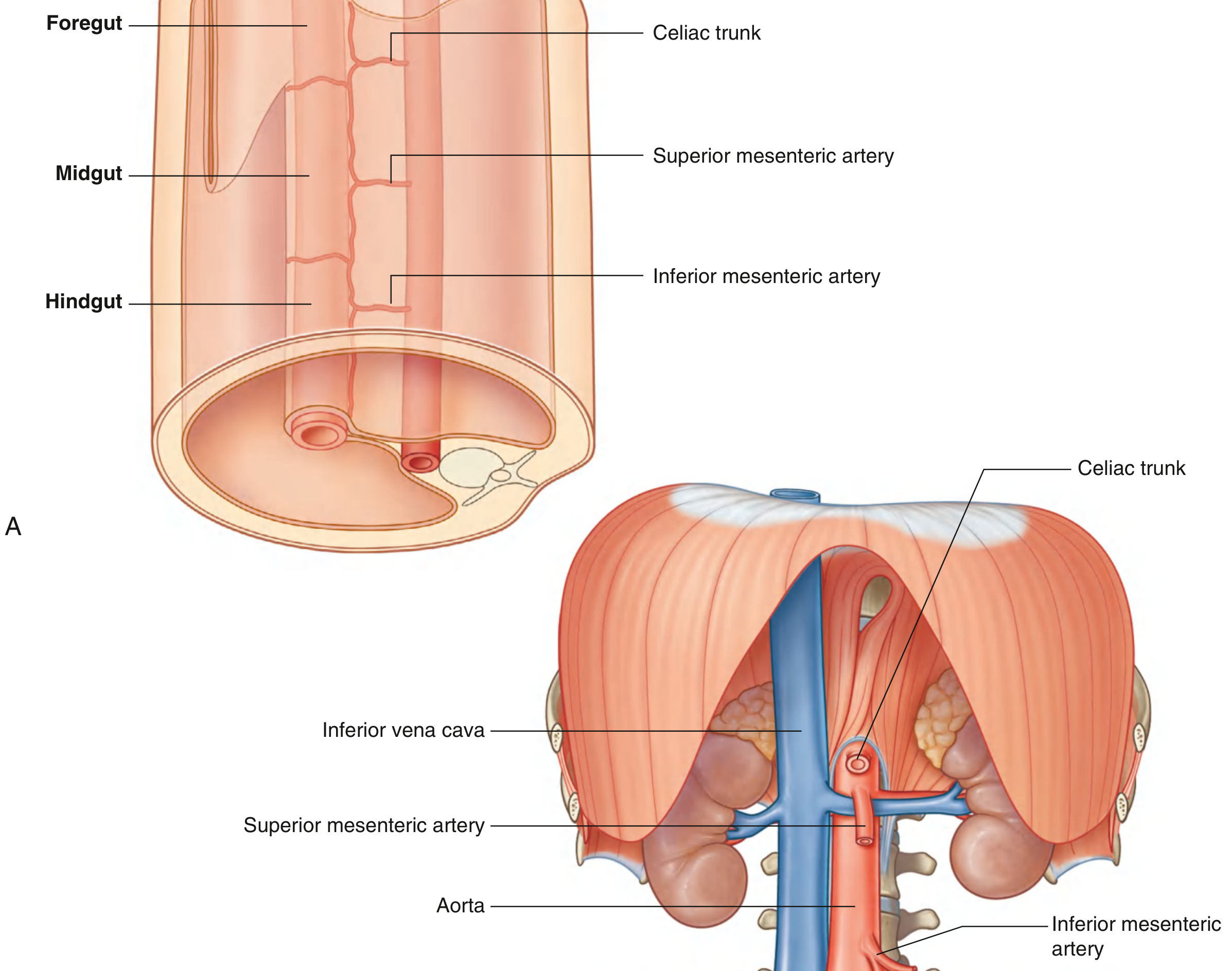
Overview Diagram of All Three Arteries
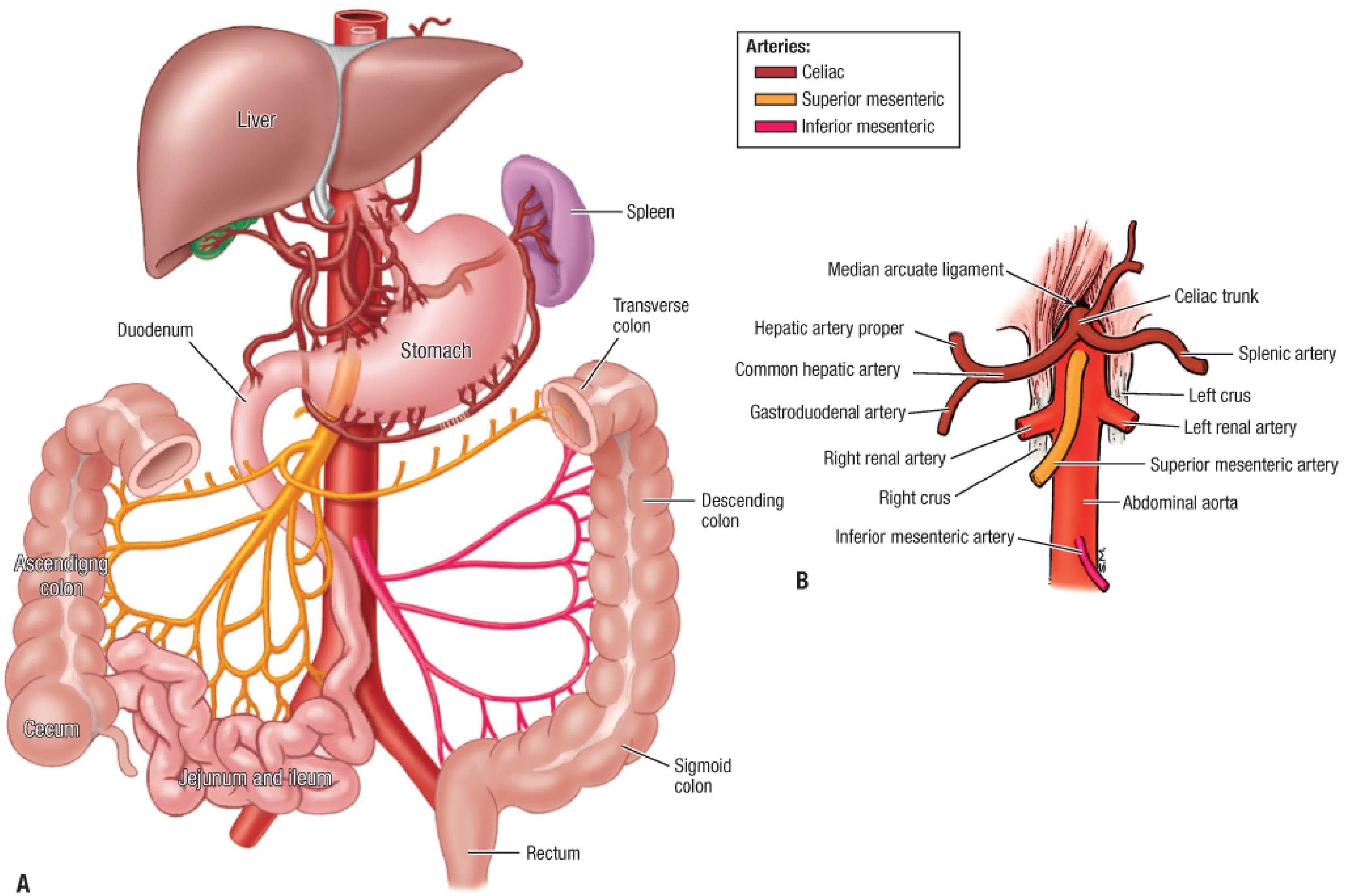
1. The Celiac Trunk (Celiac Artery)
Origin and Course
- Arises anteriorly from the aorta just inferior to the aortic hiatus at the T12 vertebral level
- It is short - typically only 1-2 cm long
- Courses anteroinferiorly before immediately dividing into its three main branches
- The celiac lymph nodes, celiac plexus, and ganglia lie in close proximity
Three Main Branches
1. Left Gastric Artery - Supplies the lower esophagus and the lesser curvature of the stomach; gives off esophageal branches ascending through the esophageal hiatus
2. Common Hepatic Artery - Runs to the right and divides into:
- Hepatic artery proper (right and left hepatic arteries to the liver)
- Gastroduodenal artery → divides into the right gastro-omental artery (along greater curvature of stomach) and the superior pancreaticoduodenal arteries (anterior and posterior), which supply the head of pancreas and proximal duodenum
- Right gastric artery (lesser curvature of stomach)
- Cystic artery (usually from right hepatic artery - supplies gallbladder)
3. Splenic Artery - The largest branch; tortuous course along the superior border of the pancreas to reach the spleen. Gives off:
- Pancreatic branches
- Short gastric arteries (to fundus of stomach)
- Left gastro-omental (gastro-epiploic) artery along the greater curvature
Structures Supplied
Lower esophagus, stomach, superior part of duodenum, proximal half of descending duodenum, head/body of pancreas, liver, gallbladder, and spleen.
Clinical Relevance - Median Arcuate Ligament Syndrome (Dunbar Syndrome)
The celiac artery can be compressed by the fibrous median arcuate ligament that forms the anterior border of the aortic hiatus. This occurs when the celiac trunk originates abnormally superiorly or when the diaphragm attaches abnormally inferiorly. This can produce postprandial pain from relative gut ischemia. - Fischer's Mastery of Surgery, 8th ed., p. 6798
2. Superior Mesenteric Artery (SMA)
Origin and Course
- Arises anteriorly from the aorta at the L1 vertebral level at an acute angle - this acute angle of origin makes it a particularly susceptible target for emboli (unlike the celiac and IMA, which originate more perpendicularly)
- Lies posterior to the pancreas proximally, then travels anterior to the fourth part of the duodenum
- Runs down into the root of the mesentery toward the right lower quadrant
Branches (in order)
1. Inferior Pancreaticoduodenal Artery (first branch)
Has anterior and posterior branches that anastomose with the anterior and posterior superior pancreaticoduodenal arteries (from the gastroduodenal artery of the celiac system), forming the pancreaticoduodenal arcades - an important collateral pathway between the celiac and SMA territories.
2. Middle Colic Artery (usually second major branch)
Travels anteriorly and divides into right and left branches:
- Right branch anastomoses with the ascending branch of the right colic artery
- Left branch anastomoses with the ascending branch of the left colic artery This is important during surgery - the middle colic artery can be followed to locate the SMA root when performing embolectomy
3. Right Colic Artery
Runs along the posterior abdominal wall to supply the ascending colon; divides into ascending and descending branches that form part of the marginal artery of Drummond
4. Ileocolic Artery
Supplies the terminal ileum, cecum, and appendix. Its descending branch gives off the appendicular artery (which passes through the mesoappendix). The descending branch of the ileocolic artery anastomoses with the terminal portion of the SMA, while the ascending branch anastomoses with the right colic artery.
5. Jejunal and Ileal Branches (10-15 branches)
Arise from the left side of the SMA as it courses toward the right lower quadrant. These branches form multiple layers of arterial arcades (anastomotic loops) in the mesentery before giving rise to vasa recta (straight arteries) that pierce the gut wall. The jejunum typically has fewer, larger arcades (1-2 tiers), while the ileum has more, smaller arcades (3-5 tiers) - a useful intraoperative distinction.
Structures Supplied
Distal duodenum, entire jejunum, entire ileum, cecum, appendix, ascending colon, and proximal two-thirds of transverse colon. Also: head and body of pancreas (via pancreaticoduodenal arcades).
Vasa Recta and Marginal Artery
The vasa recta are terminal straight arteries that branch to encircle the intestine and pierce the circular muscle. They form a rich submucosal plexus but have limited longitudinal anastomosis - destruction of vasa recti at an anastomosis site causes ischemia and anastomotic leak. The marginal artery of Drummond runs parallel to the colon 1-8 cm from the bowel wall, connecting branches of all three main colonic vessels - but it is not always complete, especially at the splenic flexure. - Fischer's Mastery of Surgery, 8th ed., pp. 6799-6803
3. Inferior Mesenteric Artery (IMA)
Origin and Course
- Arises from the anterior/left aspect of the aorta at L3 vertebral level - just superior to the aortic bifurcation into common iliac arteries
- Directed inferiorly and to the left; largely retroperitoneal course
Branches (in order)
1. Left Colic Artery (first major branch)
Divides into ascending and descending branches:
- Ascending branch → forms part of the marginal artery, anastomosing with the left branch of the middle colic artery
- Descending branch → anastomoses with the first sigmoid artery
2. Sigmoid Arteries (1-5 branches, usually 2-3)
Enter the sigmoid colon and divide into ascending and descending branches that anastomose with each other and adjacent vessels, continuing the marginal artery of Drummond.
3. Superior Rectal Artery (terminal branch)
The IMA terminates as the superior rectal (superior hemorrhoidal) artery. It crosses the left common iliac vessels in the base of the sigmoid mesocolon, enters the pelvis, and lies posterior to the rectum where it divides into right and left branches. These anastomose with the middle rectal arteries (from the internal iliac arteries) and the inferior rectal arteries (from the internal pudendal artery).
Structures Supplied
Distal third of transverse colon, descending colon, sigmoid colon, and upper/middle rectum. The distal rectum is supplied by rectal arteries from the internal iliac arteries.
Venous Exception - Inferior Mesenteric Vein
While venous drainage generally mirrors the arterial supply, the inferior mesenteric vein is an important exception. Although the IMA arises near the aortic bifurcation, the IMV ascends to the left of the aorta and drains into the splenic vein or superior mesenteric vein, posterior to the pancreas - not alongside the IMA. - Fischer's Mastery of Surgery, 8th ed., pp. 6803-6804
4. Venous Drainage - The Portal System
All venous blood from the stomach, intestines, pancreas, spleen, and gallbladder drains into the hepatic portal vein - a second capillary bed - before returning to the heart. The distal rectum is the exception, draining into the internal iliac veins.
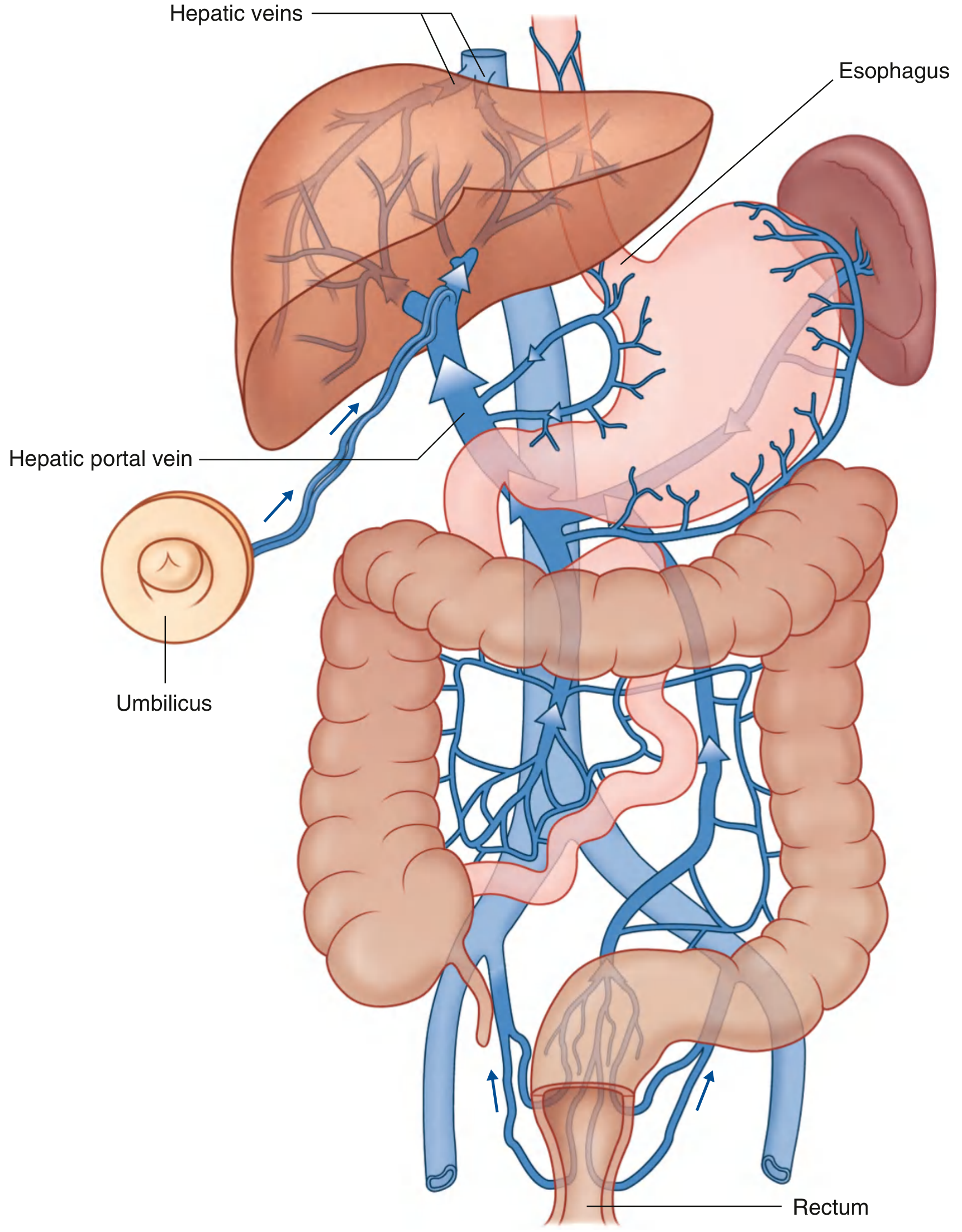
Formation of the Hepatic Portal Vein
The portal vein forms behind the neck of the pancreas at approximately the level of L2 by the union of:
- Superior mesenteric vein (drains midgut structures)
- Splenic vein (which receives the inferior mesenteric vein)
It ascends in the free edge of the lesser omentum (hepatoduodenal ligament), where it lies posterior to the bile duct and hepatic artery proper. It enters the liver at the porta hepatis and ramifies like an artery to deliver blood to hepatic sinusoids.
After the Liver
Blood exits the hepatic sinusoids into the hepatic veins (right, middle, left), which drain directly into the inferior vena cava just below the diaphragm at T8.
Purpose of the Portal Circulation
- Detoxification - Reticuloendothelial (Kupffer) cells lining sinusoids remove bacteria and particulate matter from portal blood before it reaches systemic circulation
- Nutrient processing - The liver stores 50-75% of absorbed carbohydrates and proteins temporarily for metabolic processing
- Lipid bypass - Fats absorbed as chylomicrons bypass the portal system entirely, entering intestinal lymphatics → thoracic duct → systemic circulation - Guyton and Hall, Medical Physiology, p. 782
5. Portacaval (Portosystemic) Anastomoses
Where the portal and systemic venous territories overlap, small connecting veins form potential collateral pathways. These are clinically critical in portal hypertension.
| Site | Portal Vessel | Systemic Vessel | Clinical Consequence |
|---|---|---|---|
| Lower esophagus | Tributaries of left gastric vein | Azygos/hemiazygos (systemic) | Esophageal varices |
| Lower rectum/anal canal | Superior rectal vein (portal) | Middle/inferior rectal veins (iliac) | Anorectal varices |
| Umbilicus | Para-umbilical veins (portal) | Superficial epigastric veins | Caput medusae |
| Retroperitoneum | Colic veins (portal) | Lumbar/renal veins | Retroperitoneal varices |
| Bare area of liver | Hepatic vessels | Phrenic veins | Minor anastomosis |
When portal pressure rises (e.g., in cirrhosis), these small connecting veins enlarge dramatically, allowing portal blood to bypass the liver and return to systemic circulation. This decompresses the portal system but can produce life-threatening variceal hemorrhage. - Gray's Anatomy for Students, p. 333
6. Intramural Vessels and Microcirculation
After the large extramural vessels enter the gut wall, they follow a characteristic pattern:
In the Stomach
Submucosal arterioles branch into capillaries at the base of gastric glands, pass perpendicularly through the mucosa, form a luminal capillary network, and drain into mucosal venules at the most luminal level of the lamina propria.
In the Small Intestine
Arteries pierce the muscularis and generate 1A submucosal arterioles → 2A arterioles (anastomosed pressure manifold) → 3A arterioles that descend into villi (villus microcirculation) and 4A arterioles that supply the muscularis.
Each intestinal villus contains an arteriole-venule countercurrent arrangement: the arteriole and venule run in opposite directions in close apposition. Up to 80% of oxygen diffuses directly from arterioles to adjacent venules without reaching the villus tip. Under normal conditions this is not harmful, but in circulatory shock, the resulting oxygen deficit causes villus tip ischemia and sloughing - a major cause of mucosal barrier failure. - Guyton and Hall, p. 784
In the Colon
Vasa recta from the marginal artery enter the bowel wall, supplying the muscularis and forming a rich submucosal plexus. Unlike in the small intestine, longitudinal blood flow within the colonic vasa recta is very limited.
7. Regulation of Gut Blood Flow
Under normal resting conditions, the gut receives ~1.5-2 L/min. After a meal, mesenteric blood flow rises by 1-2 L/min (the "hyperemic response"). Blood flow in villi can increase up to 8-fold during active absorption.
Vasodilators Released During Digestion
- Peptide hormones from mucosa: cholecystokinin, vasoactive intestinal peptide (VIP), gastrin, secretin
- Kinins (kallidin and bradykinin) from glandular cells - powerful local vasodilators
- Decreased oxygen tension in gut wall → increased adenosine (up to 4-fold) → vasodilation (adenosine is a potent vasodilator)
- Metabolic byproducts: CO₂, H⁺, K⁺
Neural Control
- Parasympathetic stimulation: increases blood flow secondarily through increased glandular secretion (indirect effect)
- Sympathetic stimulation: causes intense vasoconstriction of arterioles throughout the GI tract. During hemorrhagic shock, this temporarily redirects blood to vital organs but if prolonged causes gut ischemia and bacterial translocation - Guyton and Hall, p. 784
8. Watershed Areas and Clinical Vulnerability
Two anatomical regions where adjacent arterial territories meet with limited anastomosis are particularly prone to ischemia:
1. Splenic Flexure ("Griffiths' Point")
The watershed between the SMA territory (middle colic artery) and the IMA territory (left colic artery). The marginal artery is often incomplete here. This is the most vulnerable site for ischemic colitis - the mucosa sloughs off, risking infection and perforation.
2. Rectosigmoid Junction ("Sudeck's Point")
The watershed between the last sigmoid artery and the superior rectal artery - both from the IMA. Vulnerable during low anterior resection surgery.
Atherosclerosis
Atherosclerosis accounts for >90% of mesenteric artery stenosis. The CA and SMA are usually affected at their origins. If the openings of the celiac trunk and SMA become narrowed, gut blood supply falls. After a meal, oxygen demand exceeds the limited supply, causing mesenteric angina (intestinal angina) - severe postprandial pain, food avoidance, and weight loss. If the IMA alone becomes occluded, many patients remain asymptomatic because the marginal artery of Drummond gradually enlarges to maintain left colon perfusion via collaterals from the SMA territory. - Gray's Anatomy for Students, p. 415; Fischer's Mastery of Surgery, p. 6806
Summary Table: Three Main Gut Arteries
| Feature | Celiac Trunk | Superior Mesenteric Artery | Inferior Mesenteric Artery |
|---|---|---|---|
| Origin from aorta | T12 (just below hiatus) | L1 | L3 |
| Angle of origin | Perpendicular (anteroinferior) | Acute angle anteriorly | Perpendicular |
| Gut territory | Foregut | Midgut | Hindgut |
| Embolic risk | Lower | Highest (acute angle) | Lower |
| Key branches | Left gastric, common hepatic, splenic | Inf. pancreaticoduodenal, middle colic, right colic, ileocolic, jejunal/ileal | Left colic, sigmoid arteries, superior rectal |
| Collateral with | SMA (pancreaticoduodenal arcades) | Celiac + IMA (marginal artery) | SMA (marginal) + iliac (rectal) |
Key Sources:
- Gray's Anatomy for Students, 4th ed., pp. 329-333, 413-415
- Fischer's Mastery of Surgery, 8th ed., pp. 6798-6807
- Yamada's Textbook of Gastroenterology, 7th ed., pp. 246-247
- Guyton and Hall Textbook of Medical Physiology, pp. 782-784
This is a shared conversation. Sign in to Orris to start your own chat.