Ophthalmology instruments with their figure
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content and figures from Kanski's Clinical Ophthalmology. Let me compile the full, well-organized answer with all the images.
Ophthalmology Instruments
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
1. Slit Lamp (Biomicroscope)
The slit lamp is the cornerstone instrument of ophthalmic examination. It combines a binocular stereoscopic microscope with a variable-intensity light source that can be shaped into a thin "slit" beam to provide a cross-sectional view of the eye.
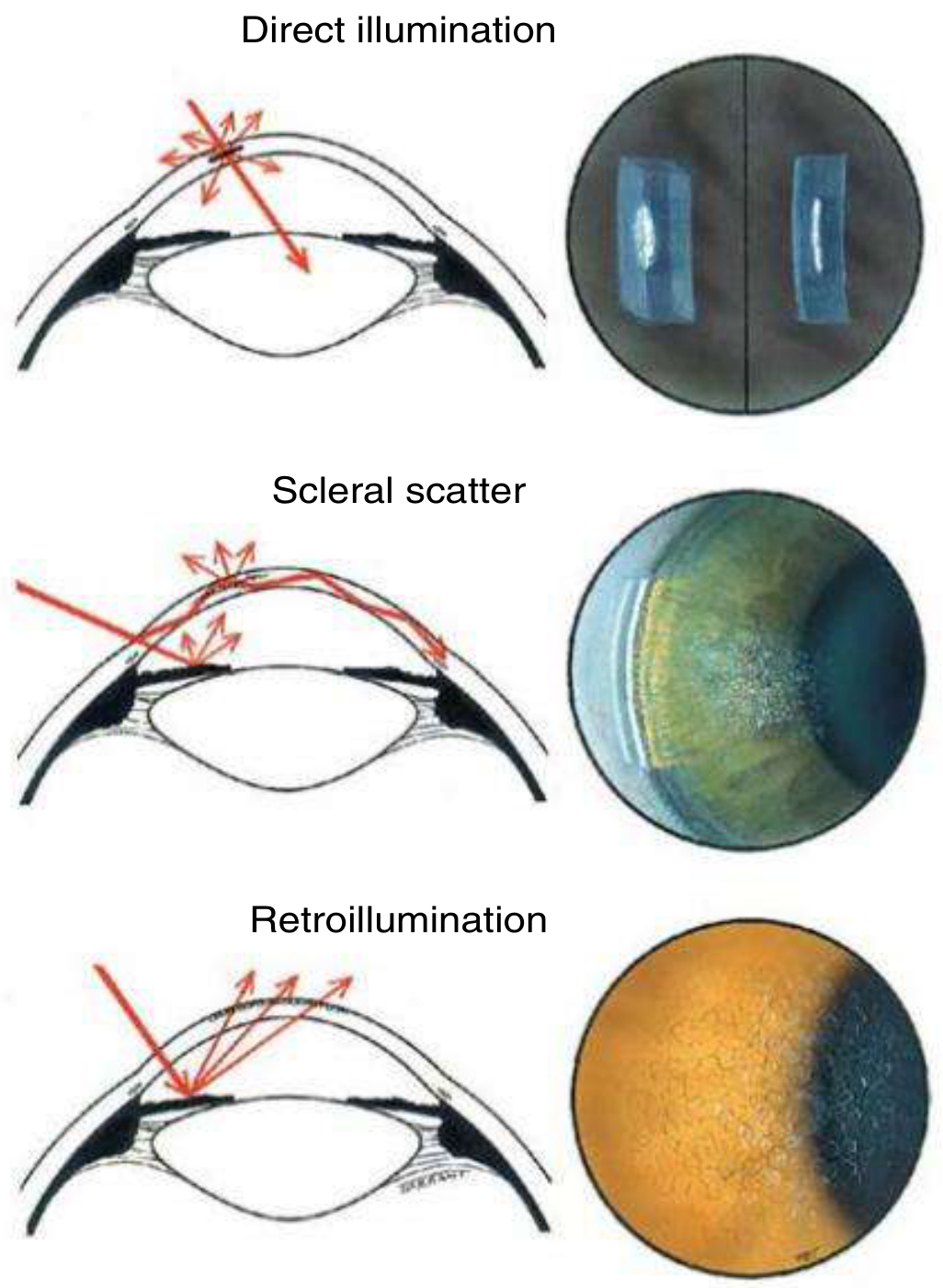
Illumination techniques used with the slit lamp:
- Direct illumination - a narrow oblique slit beam creates an optical cross-section of the cornea, allowing depth estimation of lesions
- Scleral scatter - the beam is decentered to the limbus; light undergoes total internal reflection within the cornea, illuminating any stromal haze or infiltrates
- Retroillumination - reflected light from the iris or fundus illuminates the cornea from behind, detecting fine epithelial/endothelial changes
- Specular reflection - shows endothelial abnormalities such as guttata and reduced cell density
2. Portable (Hand-held) Slit Lamp
The Keeler PSL Classic is a hand-held slit lamp that allows high-quality anterior segment examination in patients who cannot sit at a standard slit lamp - useful for bedridden patients, children, and outreach settings.

3. Direct Ophthalmoscope
A hand-held instrument providing a magnified (x15), monocular view of the fundus. Key features:
- Can be used at the bedside
- Retroillumination with +15 D lens detects lens/vitreous opacities
- Cobalt blue filter detects corneal abrasions after fluorescein instillation
- Limitation: No stereopsis and small field of view
4. Binocular Indirect Ophthalmoscope (BIO)
The head-mounted BIO provides a wide-field, stereoscopic, inverted view of the fundus through a hand-held condensing lens. It offers superior visualization through media opacities and allows scleral indentation.

Condensing lens powers used with BIO:
| Lens Power | Magnification | Field of View | Main Use |
|---|---|---|---|
| 20 D | ×3 | ~45° | Standard fundus examination |
| 28 D | ×2.27 | 53° | Small pupils |
| 40 D | ×1.5 | 65° | Children / broad scan |
5. Goldmann Three-Mirror Contact Lens
A contact lens placed on the anaesthetized cornea using coupling fluid. It contains three angled mirrors that allow different zones of the fundus to be examined at the slit lamp:
- Large trapezoid mirror (75°) - equatorial retina
- Rectangular mirror (67°) - peripheral retina
- Dome-shaped (smallest) mirror (59°) - extreme periphery, pars plana, and gonioscopy
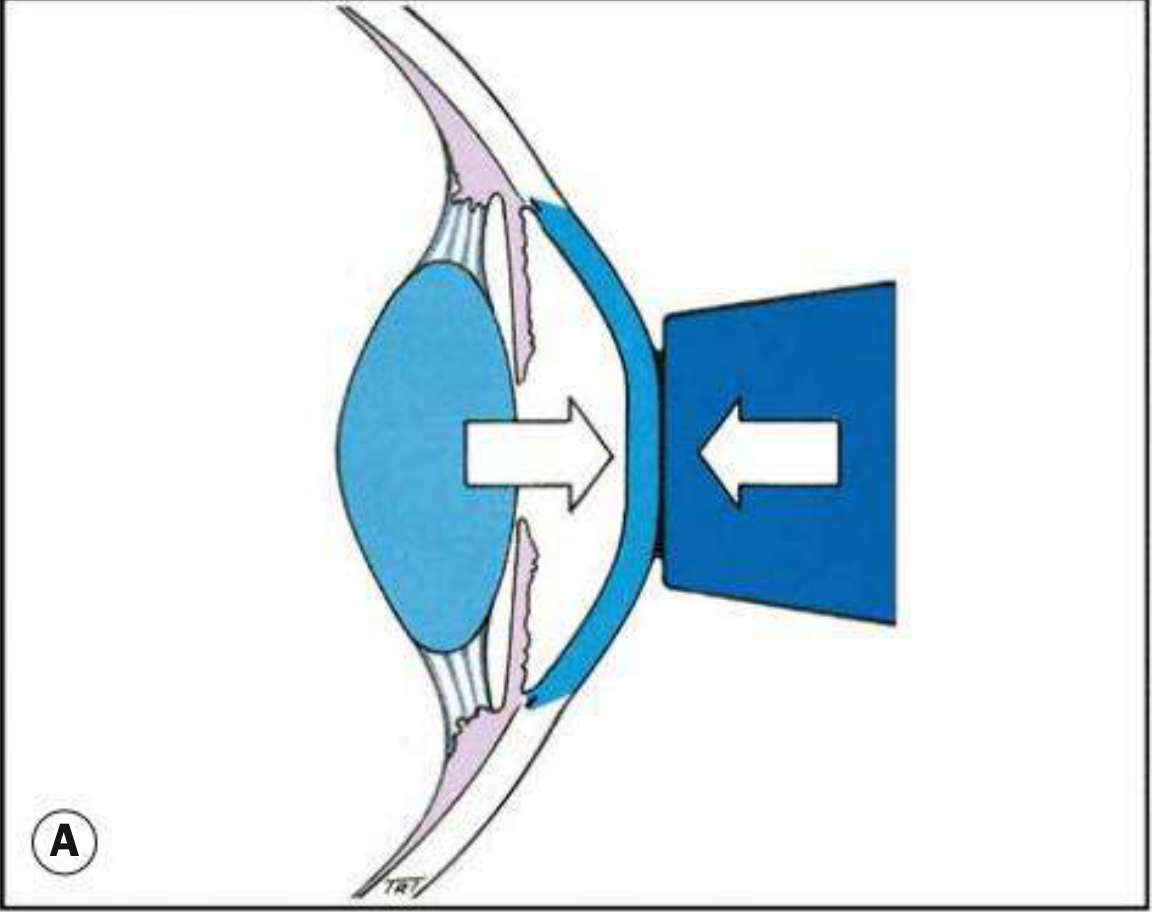
6. Goldmann Applanation Tonometer
The gold standard for measuring intraocular pressure (IOP). Based on the Imbert-Fick principle: IOP = Force / Area of applanation. The tonometer head contains a double prism and is mounted on the slit lamp. Corneal rigidity and capillary attraction cancel out when the flattened diameter = 3.06 mm.
Technique: Topical anaesthetic + fluorescein dye is instilled; the tonometer prism is gently applied to the cornea under cobalt blue illumination.

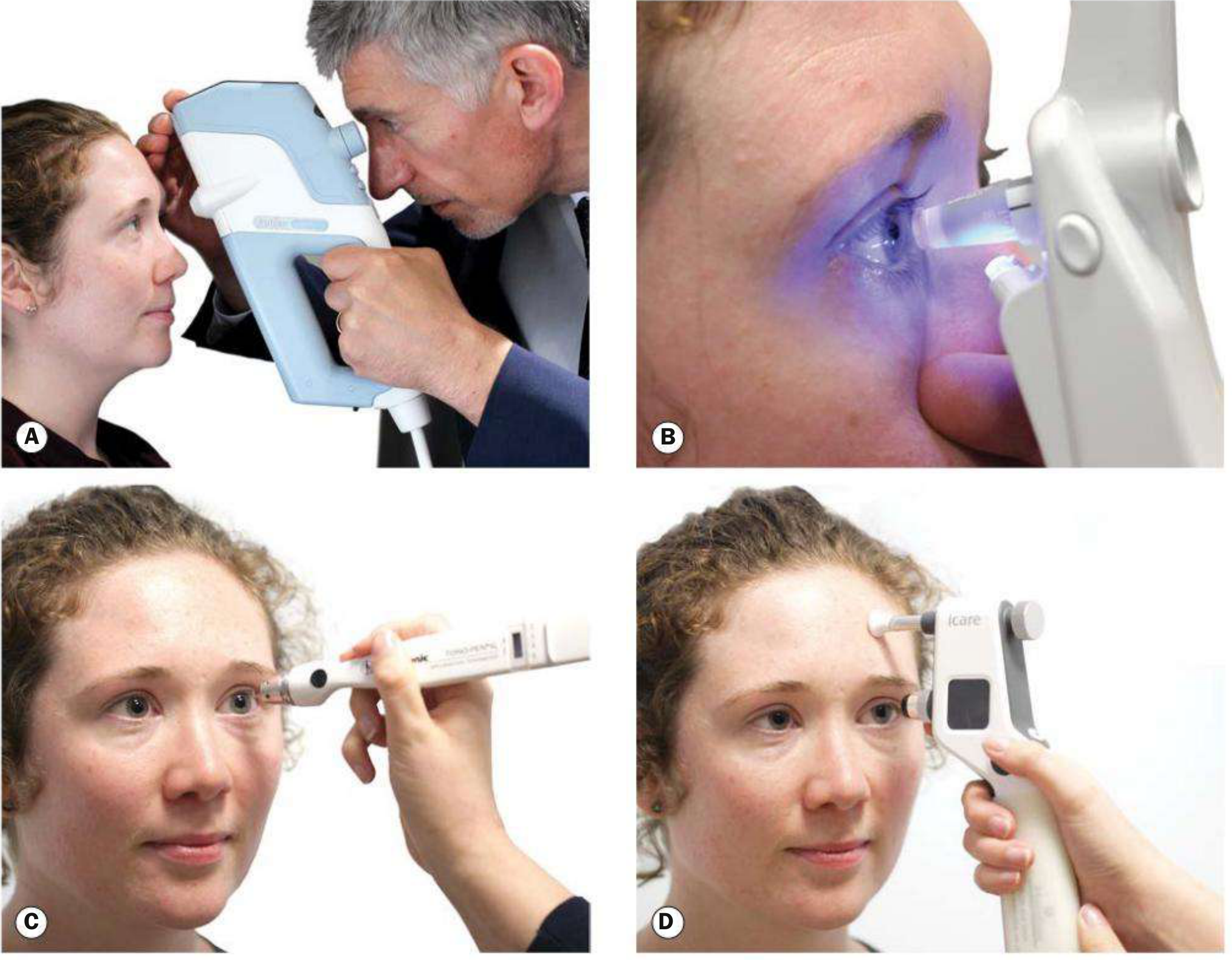
7. Other Tonometers
| Tonometer | Principle | Key Feature |
|---|---|---|
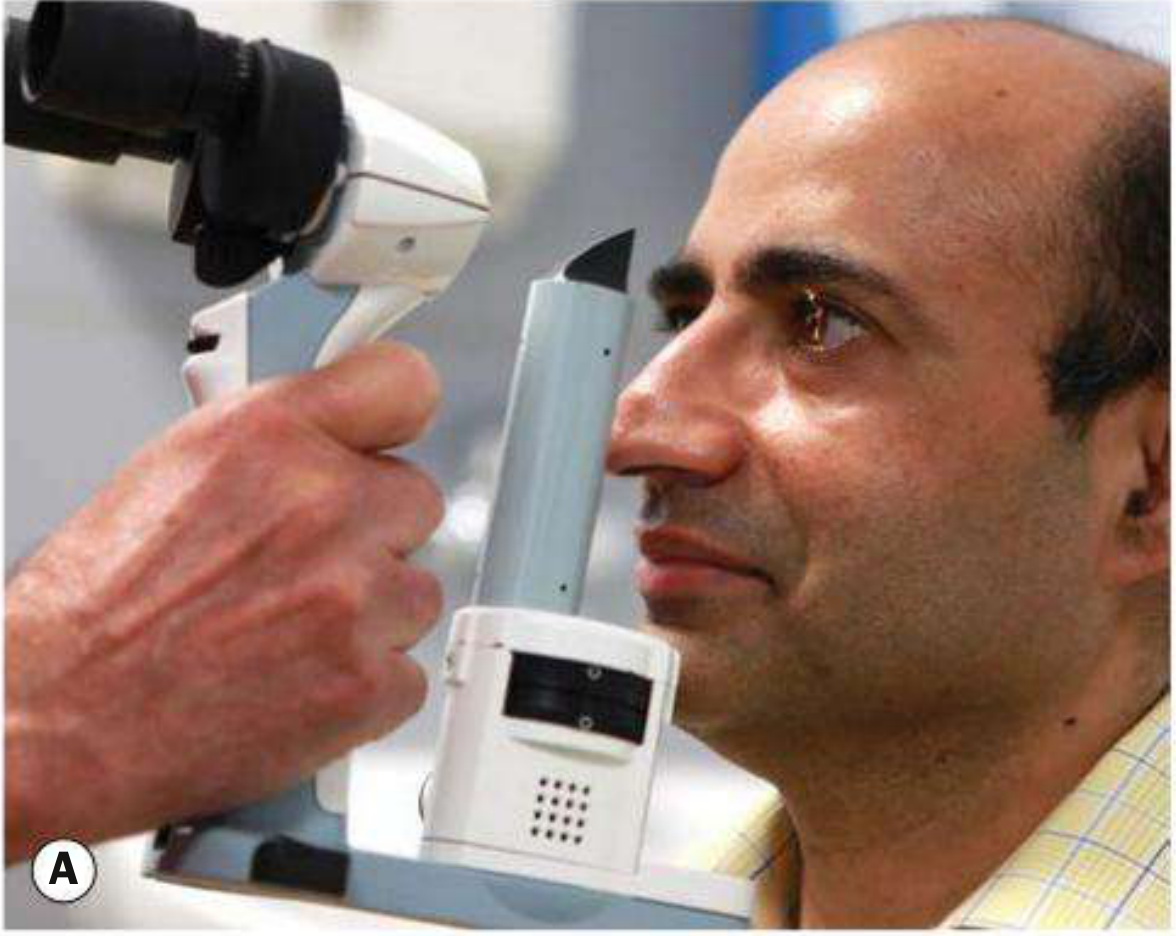
| Non-contact (Pulsair) | Air-jet applanation | No anaesthesia needed; community screening |
| Perkins Applanation | Goldmann prism + portable light source | Hand-held; use in anaesthetized/bedridden patients |
| Tono-Pen AVIA | Electronic indentation/applanation | Useful for distorted/oedematous corneas; portable |
| iCare (Rebound) | Deceleration of a 1.8 mm probe ball on corneal contact | No anaesthesia; suitable for self-monitoring at home |
| PASCAL (DCT) | Dynamic contour (solid-state sensor) | Measures IOP more independently of corneal properties |
| Schiotz | Indentation (plunger of known weight) | Seldom used today; historical importance |
8. Gonioscopy Lenses
Used to visualize the anterior chamber angle (which cannot be seen directly due to total internal reflection at the tear film-air interface). Goniolenses have a refractive index similar to the cornea, eliminating this reflection.
Two types:
Goldmann / Haag-Streit Three-Mirror Lens (Indirect gonioscopy)
- Requires coupling fluid (methylcellulose)
- Provides an inverted, magnified view of the opposite angle
- Suitable for laser trabeculoplasty
Zeiss / Posner / Sussman Four-Mirror Gonioprism (Indirect, indentation gonioscopy)
- Contact surface is flatter than the cornea - no coupling fluid needed
- Four mirrors allow 360° angle assessment without rotating the lens
- Allows indentation (dynamic) gonioscopy to distinguish appositional from synechial closure

9. Summary Table
| Instrument | Function | Key Principle |
|---|---|---|
| Slit lamp | Anterior + posterior segment examination | Variable-beam biomicroscopy |
| Portable slit lamp | Bedside/field anterior segment exam | Hand-held slit beam |
| Direct ophthalmoscope | Fundus (monocular, magnified) | Retroillumination, x15 magnification |
| Binocular indirect ophthalmoscope | Wide-field fundus exam, scleral indentation | Condensing lens, inverted image |
| Goldmann three-mirror lens | Peripheral fundus + angle (slit lamp) | Three mirrors at different angles |
| Goldmann applanation tonometer | IOP measurement (gold standard) | Imbert-Fick; flattening diameter 3.06 mm |
| Non-contact tonometer | IOP screening | Air-jet applanation |
| Perkins tonometer | IOP in non-seated patients | Portable Goldmann prism |
| Tono-Pen | IOP in irregular corneas | Electronic indentation |
| iCare | IOP; self-monitoring | Rebound (probe deceleration) |
| Zeiss goniolens | Angle examination + indentation | Four-mirror; no coupling fluid |
| Goldmann goniolens | Angle + peripheral fundus | Three-mirror; coupling fluid required |
All figures and clinical content sourced from Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition, the standard ophthalmic reference text.
This is a shared conversation. Sign in to Orris to start your own chat.