I have a patient who is been diagnosed by acute lower respiratory infection, hospise t his report for influenzas but the test is not yet confirmed but still they are giving him cap fluvir 75mg is it acceptable???
Reading File
Finding Sources
Searching PubMed
oseltamivir empirical treatment influenza lower respiratory infection unconfirmed
Searching the Web
oseltamivir empirical use before influenza test confirmation guidelines 2024
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is a full, well-supported answer:
Is Empirical Cap Fluvir (Oseltamivir) 75 mg Acceptable Before Test Confirmation? YES - It Is Standard Practice
Short answer: Absolutely acceptable and clinically recommended. Waiting for confirmatory influenza test results before starting oseltamivir in a hospitalized patient with acute lower respiratory infection (ALRI) and clinical suspicion of influenza goes against current guidelines from IDSA, CDC, and WHO.
What the CDC Decision Algorithm Says
The CDC's own flowchart (below) is unambiguous for this situation:
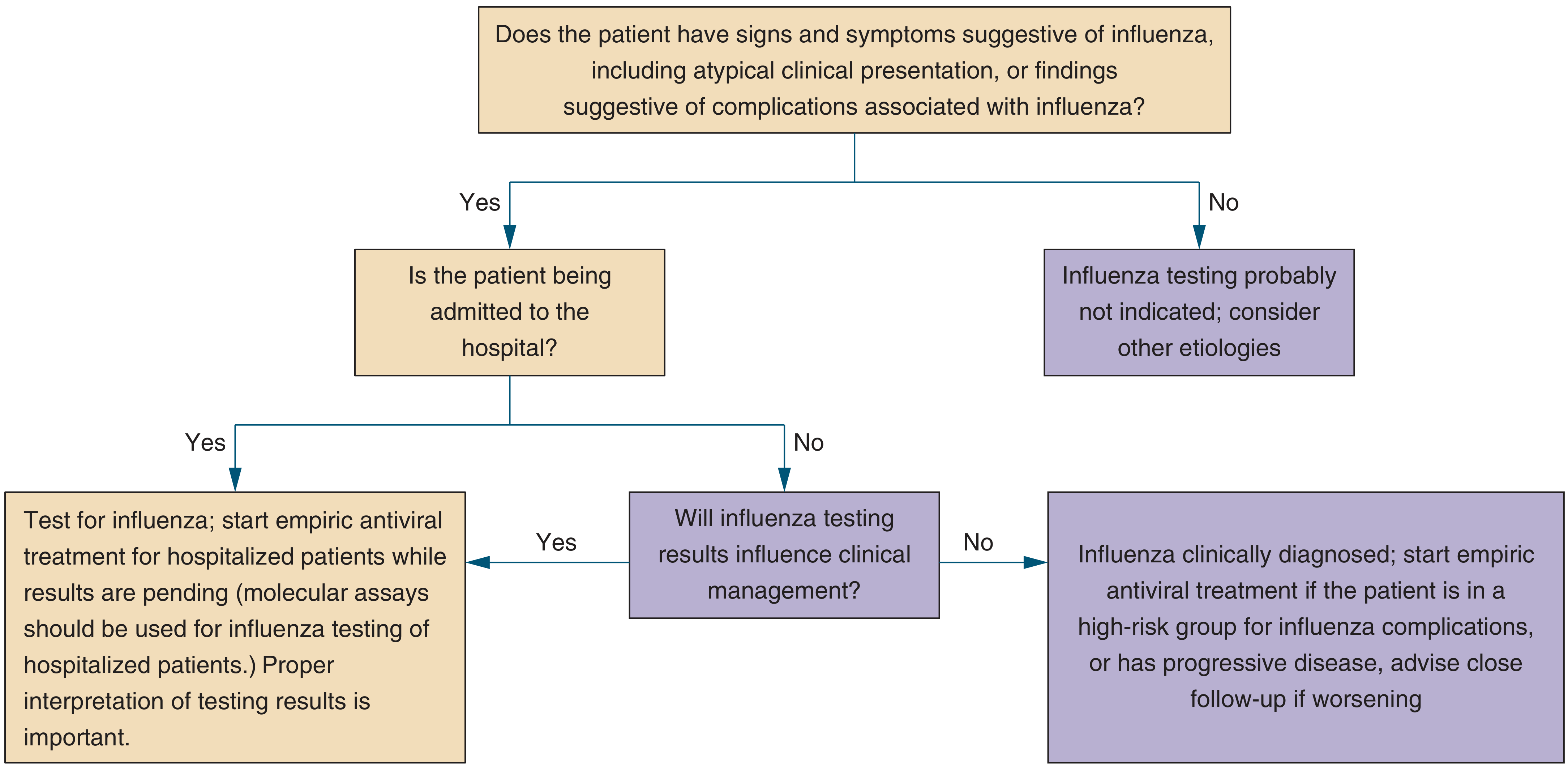
For a hospitalized patient with signs/symptoms suggestive of influenza:
"Test for influenza; start empiric antiviral treatment for hospitalized patients while results are pending. Molecular assays should be used for influenza testing of hospitalized patients."
The algorithm literally instructs you to treat AND test simultaneously - not wait for results.
- Symptom to Diagnosis: An Evidence Based Guide, 4th Ed., p. 192
Why Empirical Treatment Is Justified Here
1. Rapid tests have poor sensitivity
Rapid antigen tests have sensitivity of only 33-87%. A negative rapid test does NOT rule out influenza (negative LR = 0.13-0.67). So a "not yet confirmed" result may simply be a false negative - not a true exclusion.
2. Lower respiratory tract involvement changes the equation
In hospitalized patients with severe lower respiratory tract disease, nasopharyngeal swabs can be negative even when lower respiratory specimens (sputum, BAL) are positive. This is another reason not to wait.
3. Time is critical
The greatest benefit of oseltamivir comes from early treatment. While the 48-hour window is cited for outpatients with mild illness, hospitalized patients benefit even beyond 48 hours after symptom onset.
What Major Guidelines Say
| Authority | Recommendation |
|---|---|
| IDSA | Treat ALL hospitalized patients as early as possible, regardless of symptom duration or test result. Oseltamivir is the first-line drug for hospitalized patients. |
| CDC | Start empiric antiviral treatment while results are pending in hospitalized patients. Do not delay for test results. |
| WHO (2024 guidelines) | Treatment should not be delayed while awaiting laboratory results in patients requiring hospitalization. |
| Harrison's (2025) | "CAP patients with proven influenza should be given anti-influenza treatment (e.g., oseltamivir)." Clinicians should remain vigilant for bacterial co-infection/superinfection, especially MRSA. |
- Harrison's Principles of Internal Medicine, 22E (2025), p. 1072
- Rosen's Emergency Medicine, p. 3047
- StatPearls - Oseltamivir empiric use guidelines
Oseltamivir 75 mg Dosing Confirmation
-
Adults and children >40 kg: Oseltamivir 75 mg twice daily for 5 days - this is the standard treatment dose
-
For hospitalized patients who remain severely ill after 5 days, extended daily dosing can be considered
-
Note: If your patient has renal impairment (reduced creatinine clearance), dose adjustment is required
-
Recheck the dosing frequency - the standard is 75 mg BID (twice daily), not once daily
-
Rosen's Emergency Medicine, p. 3037
One Important Additional Point
Oseltamivir does NOT replace antibacterial therapy in a patient with ALRI/CAP. Bacterial-viral co-infection (especially with S. aureus/MRSA following influenza) is a serious risk. The patient should receive:
- Oseltamivir 75 mg BID x 5 days (for suspected influenza)
- Appropriate antibacterial coverage per CAP guidelines (beta-lactam ± macrolide, or respiratory fluoroquinolone)
- Monitor closely for secondary bacterial pneumonia (MRSA superinfection)
Bottom line: The treating team's decision to start Cap Fluvir 75 mg empirically is clinically sound, guideline-compliant, and the right call for a hospitalized patient with ALRI and suspected influenza. The confirmatory test should still be sent (preferably a molecular/PCR assay rather than a rapid antigen test for hospitalized patients), but treatment must not wait for the result.
But it's been 3 days now without confirmation they are giving him that drug and he is having symptoms of high grade fever,bodyache, headache, cough with expectorant, throat irritation and weakness when he was admitted
Finding Sources
Finding Sources
Searching the Web
influenza clinical diagnosis without lab confirmation symptoms classic presentation treatment guidelines
Finding Sources
Finding Sources
Finding Sources
Reading File
Here is a thorough breakdown of the situation now that you have shared the full symptom picture:
The Symptom Picture Strongly Supports Influenza - Treatment Is Correct
Clinical Presentation Analysis
Your patient has essentially the textbook presentation of influenza. This is not ambiguous:
| Symptom | Significance |
|---|---|
| High grade fever | Classic - influenza causes sudden, high fever (38.5-40°C) |
| Body ache / myalgia | One of the most distinctive features of influenza vs. other URTIs |
| Headache | Hallmark systemic symptom of influenza |
| Cough with expectoration | Indicates lower respiratory tract involvement |
| Throat irritation | Pharyngeal involvement, common in influenza |
| Weakness / malaise | Severe prostration is a defining feature of influenza |
As described in Sherris & Ryan's Medical Microbiology:
"Onset is usually abrupt... these include fever, myalgia, headache, and occasionally shaking chills. Within 6 to 12 hours the illness reaches its maximum severity, and cough develops. The acute findings persist, sometimes with worsening cough, for 3 to 5 days, followed by gradual improvement."
- Sherris & Ryan's Medical Microbiology, 8th Ed., p. 333
This clinical picture - even without lab confirmation - is sufficient justification to continue antiviral therapy. The IDSA guidelines explicitly state that a clinical diagnosis of influenza can be made based on presenting symptoms and clinical judgment. A patient does not need a positive test result to receive treatment.
Is Continuing Oseltamivir After 3 Days Still Appropriate?
Yes. The standard course is oseltamivir 75 mg twice daily for 5 days. Day 3 means the patient is still mid-course. Stopping early or withholding would be wrong. The team should complete the full 5-day course.
For hospitalized patients who remain severely ill at day 5, extended dosing beyond 5 days can even be considered.
Critical Warning: Watch for Bacterial Superinfection
This is the most important clinical concern right now. The productive cough (cough with expectorant) is a flag. Classic influenza causes a dry cough initially. A cough that becomes productive of purulent sputum during or after influenza strongly suggests secondary bacterial pneumonia.
From Sherris & Ryan's:
"The most common and important complication of influenza virus infection is bacterial superinfection... often heralded by an abrupt worsening of the patient's condition after initial stabilization. The bacteria most commonly involved include Streptococcus pneumoniae, Haemophilus influenzae, and Staphylococcus aureus (including MRSA)."
- Sherris & Ryan's Medical Microbiology, 8th Ed., p. 333
Ask the clinical team these questions:
- Is the patient already on antibacterial coverage? - For a hospitalized patient with ALRI + suspected influenza, antibacterial therapy (CAP regimen) should be running alongside oseltamivir - not just the antiviral alone.
- Has sputum culture / Gram stain been sent? - This is essential, especially with productive cough at day 3.
- Is the patient improving or worsening? - If after 48-72 hours of treatment there is no improvement or the patient is deteriorating, this mandates reassessment.
Summary: What Should Be Happening
| Action | Status |
|---|---|
| Oseltamivir 75 mg BID x 5 days | ✅ Continue - appropriate and evidence-based |
| Antibacterial coverage (beta-lactam ± macrolide, or respiratory fluoroquinolone) | Must verify this is running |
| Influenza PCR/molecular test (not just rapid antigen) | Should be pending or already sent |
| Sputum Gram stain + culture | Should be sent given productive cough |
| Blood cultures | Should be sent for hospitalized patient |
| Monitor for bacterial superinfection signs | Ongoing - any sudden worsening is a red flag |
| Supportive care (hydration, antipyretics, oxygen if SpO2 <94%) | Essential |
The patient's clinical syndrome is a strong clinical diagnosis of influenza. Continuing Cap Fluvir 75 mg is not only acceptable - it is the right decision. The key thing to watch right now is whether bacterial co-infection is developing alongside the viral illness.
This is a shared conversation. Sign in to Orris to start your own chat.