Pain, its types, mechanisms of formation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer.
Pain: Types, Mechanisms, and Pathways
Definition
The International Association for the Study of Pain (IASP) defines pain as "an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage." This definition recognizes the interplay between the objective physiological sensory aspects of pain and its subjective, emotional, and psychological components. Notably, the term nociception (from Latin noci = harm/injury) describes the neural responses to traumatic or noxious stimuli - all nociception produces pain, but not all pain results from nociception.
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 1970
Classification of Pain
Pain can be classified in three major ways:
| Classification Axis | Examples |
|---|---|
| Pathophysiology | Nociceptive vs. neuropathic |
| Temporal | Acute vs. chronic |
| Location/Source | Somatic (superficial/deep), visceral, referred |
1. By Pathophysiology
A. Nociceptive Pain
Caused by the activation or sensitization of peripheral nociceptors - specialized receptors that transduce noxious stimuli. It serves a protective function: to detect, localize, and limit tissue damage.
- Results from ongoing stimulation of peripheral nociceptors by tissue injury or inflammation (e.g., sprains, arthritis, tumor invasion)
- Usually responds well to NSAIDs and opioids
- Subtypes: somatic and visceral (see below)
B. Neuropathic Pain
Results from direct injury to or acquired abnormalities of peripheral or central neural structures. It arises from signal-processing changes in the CNS.
-
Classically described as burning, tingling, shooting, or electric sensations
-
Examples: complex regional pain syndrome (CRPS), post-herpetic neuralgia, trigeminal neuralgia, phantom limb pain, diabetic neuropathy, central pain after stroke or spinal cord injury
-
"Anesthesia dolorosa" - spontaneous burning pain occurring without any peripheral stimulus - can be triggered by ablation of trigeminal sensory neurons
-
Does NOT respond to NSAIDs; generally poorly responsive to opioids; first-line treatment involves anticonvulsants (e.g., gabapentin, pregabalin) and tricyclic antidepressants
-
Eric Kandel, Principles of Neural Science, 6th Ed., p. 521; Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 1971
2. By Temporal Duration
A. Acute Pain
- Caused by noxious stimulation due to injury, disease, or abnormal function of muscle or viscera
- Almost always nociceptive
- Has a clear protective function and usually resolves as healing occurs
- Elicits measurable neuroendocrine stress responses (tachycardia, hypertension, sweating)
B. Chronic Pain
-
Persists beyond 1-6 months past the usual course of an acute disease, or after a reasonable healing time
-
May be nociceptive, neuropathic, or mixed
-
Psychological mechanisms and environmental factors play a major role
-
Patients often have attenuated neuroendocrine responses, prominent sleep disturbances, and mood disorders
-
Driven by a combination of peripheral, central, and psychological mechanisms
-
Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 1974
3. By Location/Source
A. Superficial Somatic Pain
- Arises from skin or subcutaneous tissues
- Well-localized, sharp or burning quality
B. Deep Somatic Pain
- Arises from muscles, tendons, joints, or bones
- Dull, aching quality; less well-localized
- Both intensity and duration of stimulus affect degree of localization
C. Visceral Pain
Four subtypes:
- True localized visceral pain - dull, diffuse, usually midline; associated with autonomic features (nausea, vomiting, sweating, BP/HR changes)
- Localized parietal pain - sharp, stabbing
- Referred visceral pain - pain felt at a distance from the source organ
- Referred parietal pain
Referred Pain occurs because visceral and somatic afferent inputs converge on the same lamina V neurons in the spinal cord. The brain cannot distinguish the source, so it attributes the pain to the skin. Classic example: cardiac ischemia felt as left arm and chest pain (dermatomes T1-T4).
| Visceral Source | Referred Dermatome |
|---|---|
| Heart | T1-T4 |
| Diaphragm (central) | C4 |
| Gallbladder/Liver/Stomach | T6-T9 |
| Small intestine | T9-T11 |
| Bladder/Rectum | S2-S4 |
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 1972-1973
Mechanisms of Pain Formation: The Four Processes
The pain system algorithm involves four sequential processes:
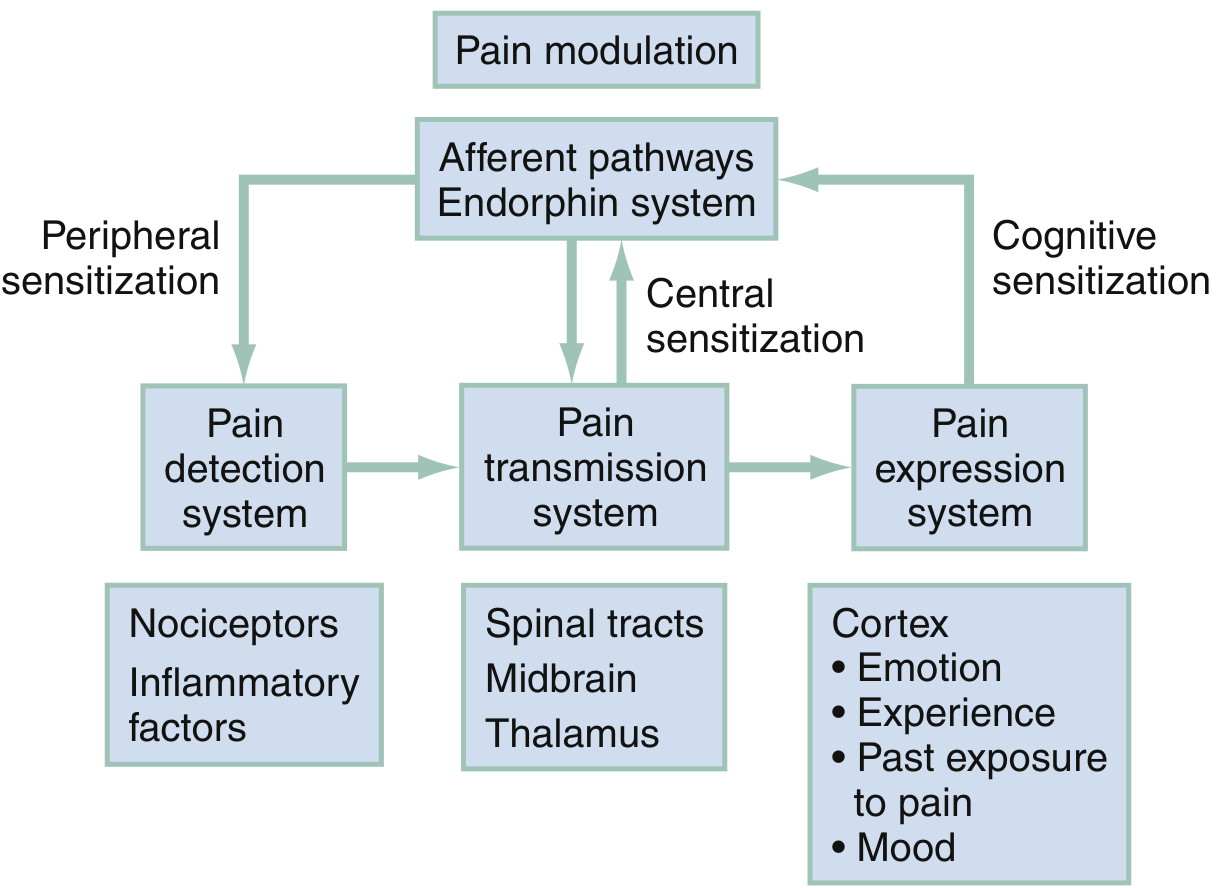
Fig. The pain system algorithm - ROSEN's Emergency Medicine
Step 1: Transduction (Pain Detection)
Nociceptors are free nerve endings in cutaneous, muscular, and visceral tissues. Three main types:
| Nociceptor Type | Stimulus Detected |
|---|---|
| Mechanoreceptors | Mechanical deformation (sharp pressure, cutting) |
| Thermoreceptors | Extremes of heat (>43°C) or cold (<17°C) |
| Polymodal nociceptors (PMNs) | Thermal, mechanical, AND chemical stimuli |
| Silent nociceptors | Normally inactive; activated by inflammation and chemical mediators |
Nociceptors are activated by TRP (transient receptor potential) channels - particularly TRPV1, which responds to heat, capsaicin, and low pH. Chemical mediators from tissue injury (bradykinin, prostaglandins, substance P, serotonin, leukotrienes) lower the threshold of nociceptor activation - this is called peripheral sensitization.
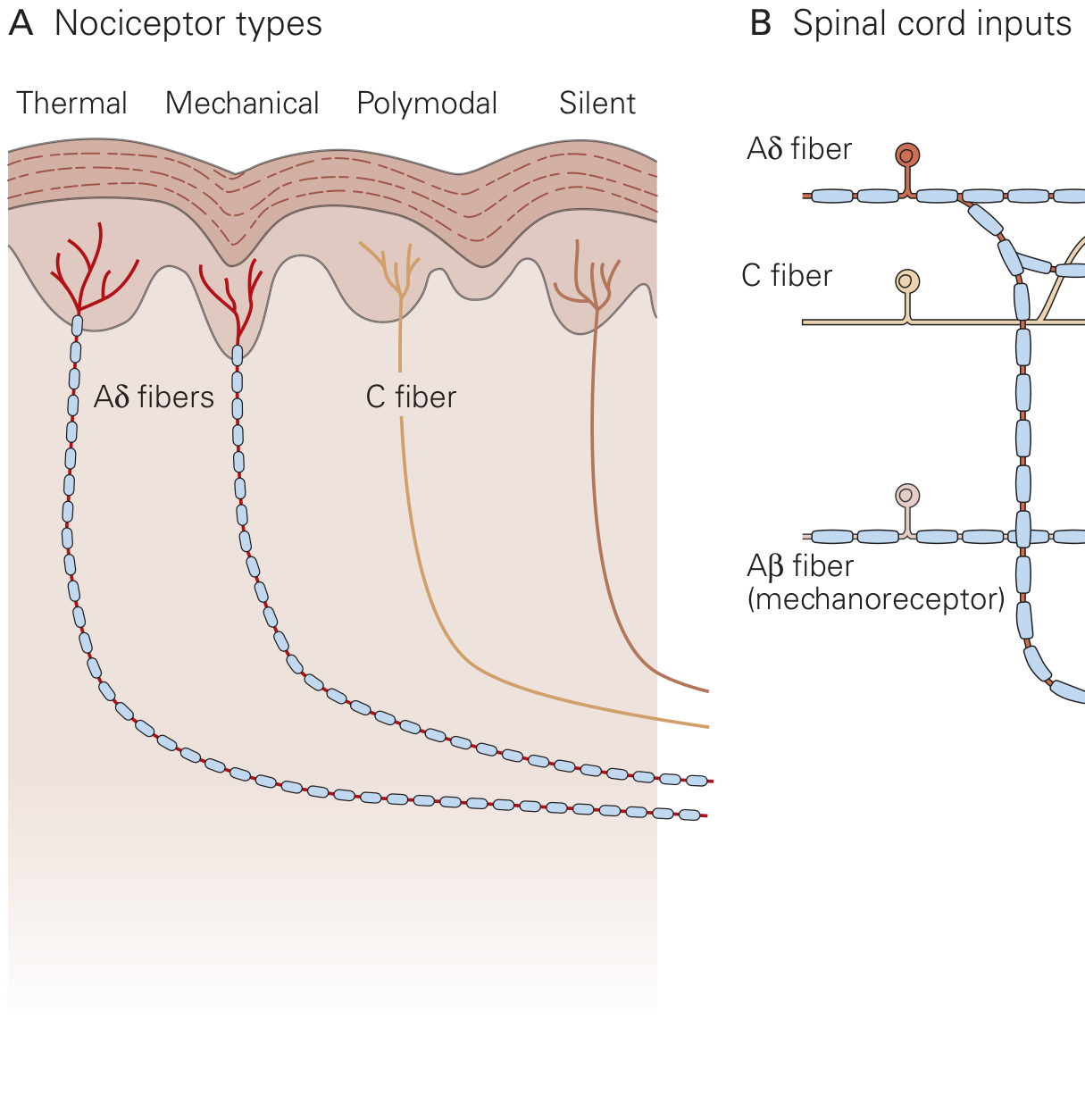
Fig. Nociceptive fibers terminating in different laminae of the dorsal horn - Kandel, Principles of Neural Science
Step 2: Transmission (Pain Conduction)
Signals travel via primary afferent nerve fibers from the periphery to the spinal cord dorsal horn:
| Fiber | Quality of Pain | Myelin | Diameter | Speed |
|---|---|---|---|---|
| A-delta (Aδ) | Sharp, initial, well-localized ("first pain") | Thinly myelinated | 1-4 μm | 12-30 m/s |
| C fibers | Dull, aching, burning ("second pain"), persistent | Unmyelinated | 0.3-1.5 μm | 0.5-2 m/s |
In the dorsal horn, primary afferents synapse in highly organized laminae:
- Lamina I (marginal layer): Receives Aδ and C fiber input; contains nociceptive-specific neurons that project to the midbrain and thalamus
- Lamina II (substantia gelatinosa): Dense interneurons - both excitatory and inhibitory - that modulate pain signals
- Laminae III-IV: Mixed interneurons and projection neurons receiving Aβ (innocuous touch) input
- Lamina V: Wide dynamic range (WDR) neurons - respond to both noxious and innocuous stimuli; receive convergent somatic AND visceral input (explaining referred pain)
From the dorsal horn, second-order neurons cross to the contralateral side and ascend via the spinothalamic tract to the thalamus and then to the somatosensory cortex.
- ROSEN's Emergency Medicine, p. 92; Kandel, Principles of Neural Science, 6th Ed., p. 522
Step 3: Modulation
Modulation occurs at three levels and can either inhibit or facilitate pain:
Peripheral modulation - inflammatory mediators (prostaglandins, bradykinin, substance P, cyclic AMP, leukotrienes, serotonin, thromboxanes) lower nociceptor thresholds → peripheral sensitization → allodynia (pain from normally innocuous stimuli)
Central sensitization (spinal cord level) - at least three mechanisms:
- Wind-up: Repeated C-fiber stimulation progressively amplifies the response of second-order WDR neurons (via NMDA receptor activation)
- Dorsal horn neuron receptor field expansion: Injured neurons recruit adjacent neurons into their receptive field
- Hyperexcitability of flexion reflexes
Supraspinal modulation - descending pathways from the periaqueductal gray (PAG), raphe nuclei, and locus coeruleus release endorphins, serotonin, and norepinephrine to inhibit pain transmission (the basis of endogenous analgesia and the action of opioids/antidepressants).
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 1975
Step 4: Perception (Pain Expression)
The final stage where neural signals are interpreted as the conscious experience of pain in the cortex. This is shaped by:
- Emotion and mood
- Past experiences with pain
- Cognitive expectations
- Cognitive sensitization (anxiety, catastrophizing amplify pain perception)
Key Terminology
| Term | Meaning |
|---|---|
| Allodynia | Pain from a normally non-noxious stimulus |
| Hyperalgesia | Increased pain response to a noxious stimulus |
| Hyperesthesia | Increased response to mild stimulation |
| Paresthesia | Abnormal sensation without apparent stimulus |
| Anesthesia dolorosa | Pain in an area lacking sensation |
| Hyperpathia | Hyperesthesia + allodynia + hyperalgesia with overreaction and after-sensation |
| Dysesthesia | Unpleasant abnormal sensation with or without stimulus |
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 1970
Summary
Pain is a complex sensory-emotional experience generated by a four-step process: transduction at nociceptors, transmission via Aδ and C fibers through the dorsal horn and spinothalamic tract, modulation at peripheral, spinal, and supraspinal levels, and perception in the cortex. The two broad pathophysiologic categories - nociceptive (protective, stimulus-driven) and neuropathic (neural damage-driven, often stimulus-independent) - differ markedly in their mechanisms, character, and response to treatment. Central sensitization (wind-up, receptor field expansion) is the key mechanism behind chronic pain amplification and the transition from acute to chronic pain states.
This is a shared conversation. Sign in to Orris to start your own chat.