Earliest cardiac signs in ACS
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Now I have comprehensive information to provide a thorough answer. Let me compile the complete picture.
Earliest Cardiac Signs in ACS
1. ECG Changes (Minutes After Occlusion)
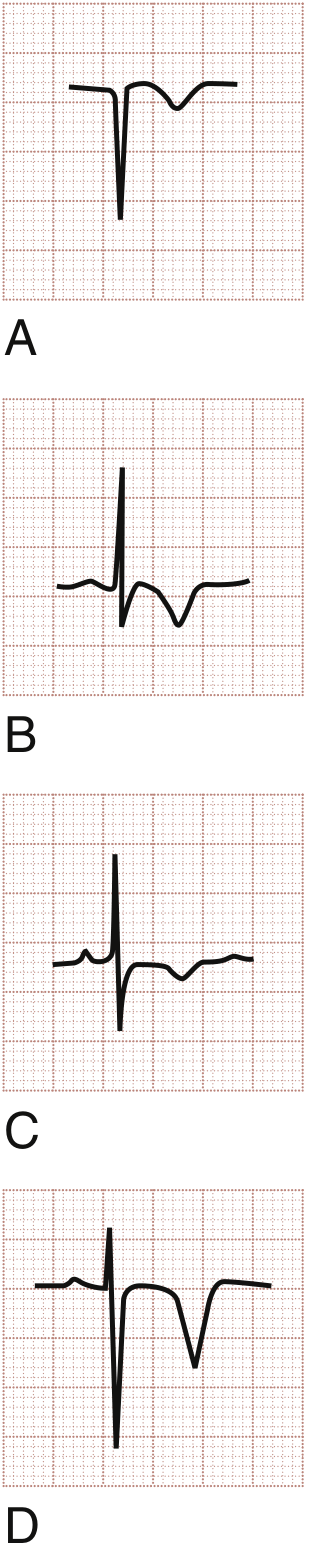
Hyperacute T Waves — The Earliest ECG Finding
The hyperacute T wave is the first electrocardiographic manifestation of STEMI, appearing within minutes of coronary blood flow interruption.
Characteristics:
- Tall, broad-based, and asymmetrical (unlike the symmetric tall T waves of hyperkalemia)
- ST segment may already be elevated at the J-point
- Seen in the distribution of the ischemic territory
- Transient — rapidly progresses to frank ST elevation, so often missed on the initial ECG
"The earliest electrocardiographic finding in STEMI is the hyperacute T wave... a tall and peaked structure that can appear within minutes of the interruption of blood flow." — ROSEN's Emergency Medicine
Differential for tall T waves: Hyperkalemia, benign early repolarization, LVH, LBBB, acute pericarditis.
ST-Segment Elevation (STEMI Evolution)
As ischemia progresses, hyperacute T waves give way to ST-segment elevation:
- Morphology evolves: flat → convex → domed ("tombstoned")
- Measured from the TP segment baseline (or PR terminal)
- Dynamic — waxes and wanes with symptoms (distinguishes from benign causes)
- ST elevation is a consequence of currents of injury from ischemia lowering resting membrane potential in the affected zone
STEMI localization:
| Territory | Leads with ST elevation |
|---|---|
| Anterior | V1–V6 |
| Inferior | II, III, aVF |
| Lateral | I, aVL, V5–V6 |
| Posterior | Reciprocal ST depression V1–V3 (no direct elevation) |
| Right ventricle | Right-sided leads (V3R–V4R) |
ST Depression — NSTEMI / Subendocardial Ischemia
- Seen in unstable angina and NSTEMI
- Typically horizontal or downsloping (upsloping is less specific)
- May also precede ST elevation in evolving STEMI
- Diffuse ST depression + ST elevation in aVR → severe ischemia (left main or proximal LAD occlusion equivalent)
STEMI Equivalents — Critical Patterns Not to Miss
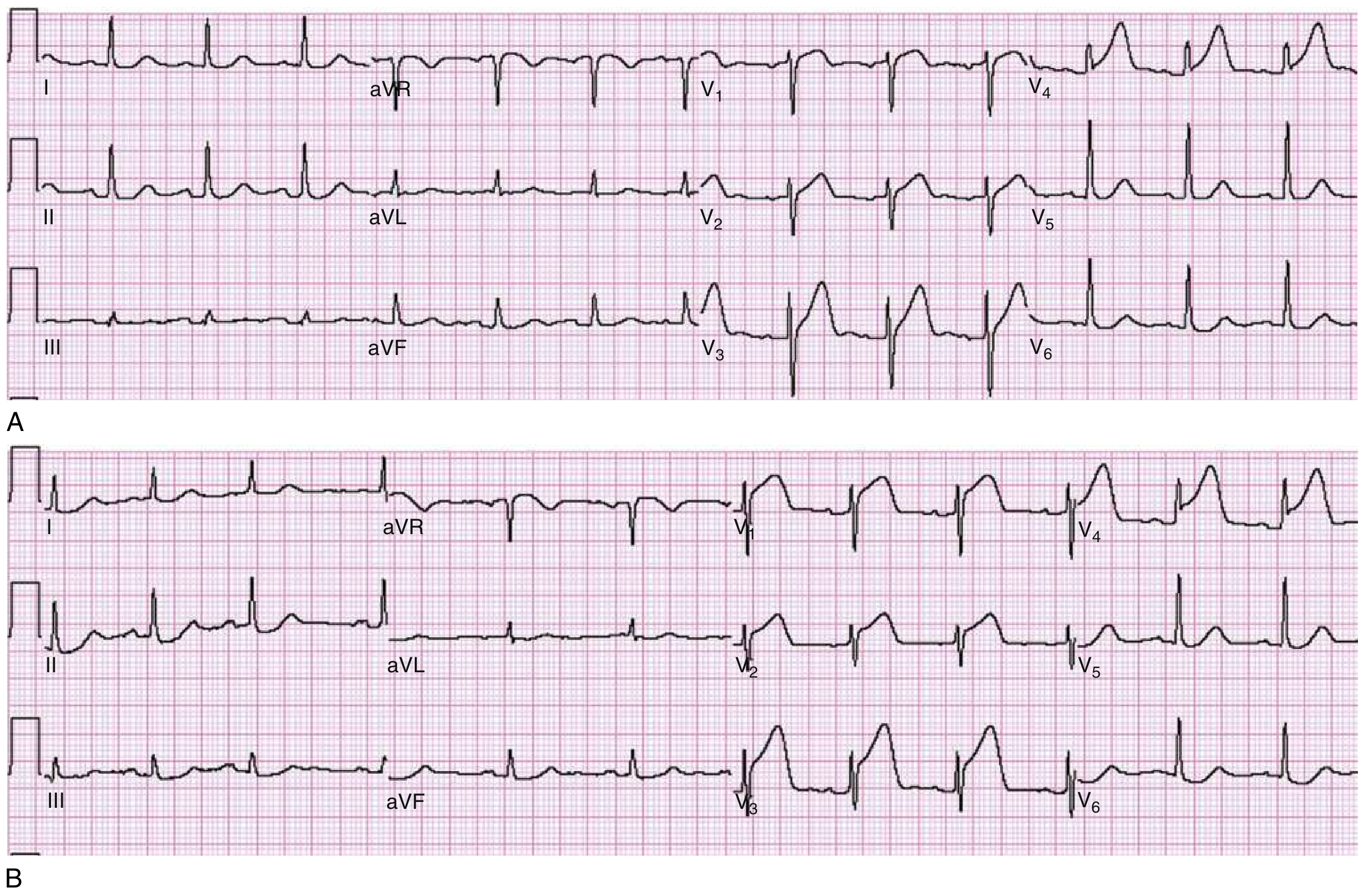
Wellens Syndrome (proximal LAD occlusion warning):
- Type A: Biphasic T waves in V2–V3 (25% of cases)
- Type B: Deeply inverted T waves in V2–V3 (75% of cases)
- Patient is often pain-free at the time of ECG — but the lesion is critical
- Can progress to massive anterior STEMI within hours
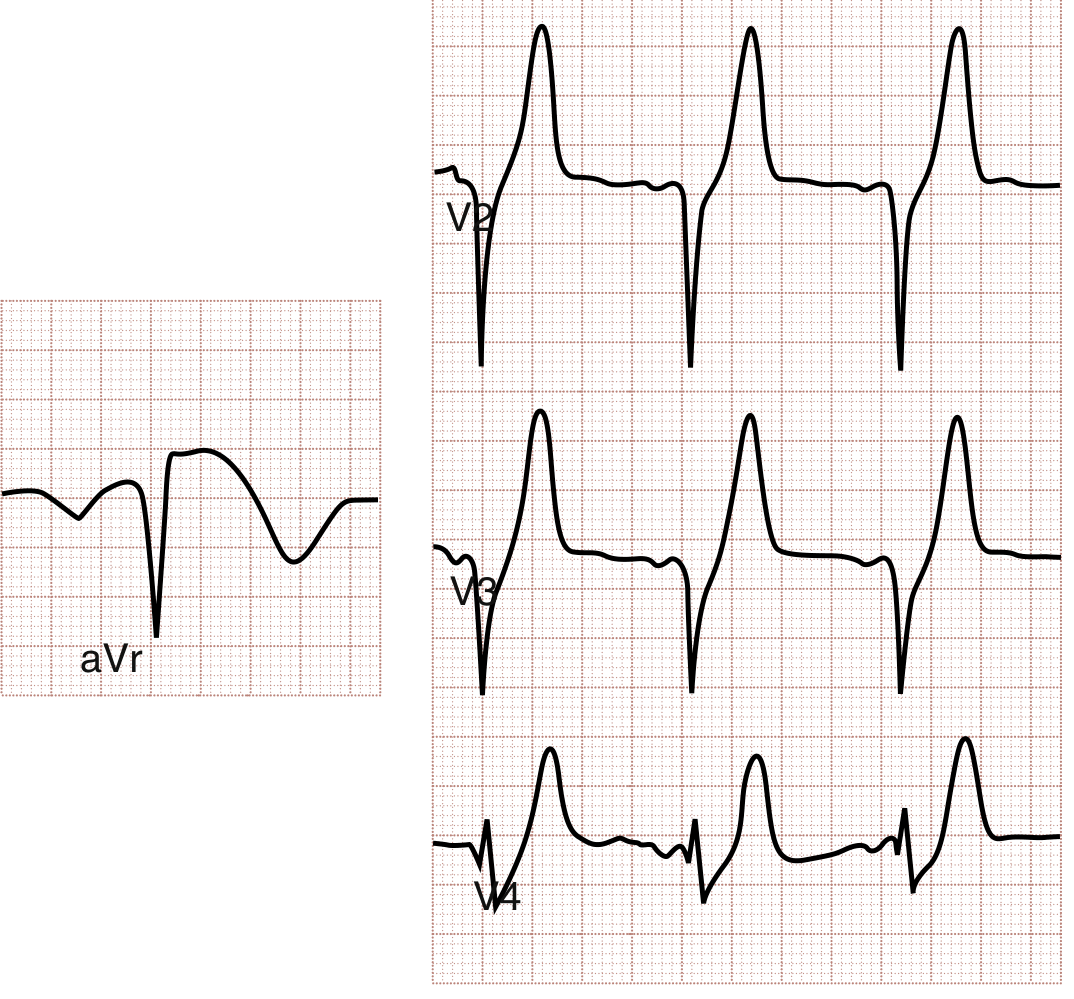
de Winter Pattern (proximal LAD occlusion):
- ST depression at the J-point + prominent upward T waves in precordial leads
-
- ST elevation in aVR
- Treated as a STEMI equivalent — may not progress to classic ST elevation but represents total/near-total LAD occlusion
Posterior MI:
- No direct ST elevation on standard 12-lead
- Presents as ST depression + tall R wave in V1–V3
- Confirmed with posterior leads V7–V9
T-Wave Inversions
- Classically narrow and symmetrical in ACS (unlike broad asymmetric post-MI inversions)
- May represent subacute/evolving ischemia
- Pseudonormalization — a previously inverted T wave that appears "normal" during chest pain is an ischemic sign
Q Waves — Late Finding
- Represent irreversible myocardial necrosis
- May appear within the first hour of infarction, but most commonly develop at 8–12 hours
- Their presence does NOT preclude emergent reperfusion — treat based on clinical history and symptoms
2. Cardiac Biomarkers (Hours After Infarction)
| Biomarker | Rises | Peaks | Notes |
|---|---|---|---|
| High-sensitivity troponin I/T | 1–3 hours | 24–48 hours | Most sensitive early marker; rises before symptoms evolve |
| Conventional troponin T | 2–3 hours | ~48 hours | Remains elevated up to 2 weeks |
| CK-MB | 3–6 hours | 12–24 hours | Less sensitive early |
The Fourth Universal Definition of MI requires a rising and/or falling pattern of troponin with at least one value above the 99th percentile URL to distinguish acute myocardial injury from chronic elevation.
Summary: Chronological Sequence of Earliest Signs
Minutes 0–30: Hyperacute T waves (ECG)
Minutes 30–60: ST-segment elevation (STEMI) or ST depression (NSTEMI/UA)
Hours 1–3: High-sensitivity troponin begins to rise
Hours 1–12: T-wave inversions (evolving ischemia or post-reperfusion)
Hours 8–12: Pathologic Q waves develop (necrosis complete)
A normal ECG does not exclude ACS — up to 6% of STEMI patients have a normal initial ECG. Serial ECGs every 15–30 minutes, coupled with serial high-sensitivity troponins (0h/1h or 0h/2h protocols), are the standard approach.
Sources: ROSEN's Emergency Medicine; Harrison's Principles of Internal Medicine 22E; Braunwald's Heart Disease; Robbins & Kumar Basic Pathology
Cardiac examination findings in ACS patient
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have sufficient data for a comprehensive, well-structured answer.
Cardiac Examination Findings in ACS
Cardiac examination in ACS spans from a nearly normal exam in uncomplicated unstable angina to dramatic findings when large infarction, shock, or mechanical complications supervene. Findings are best organized by system of examination.
General Appearance & Vital Signs
| Finding | Significance |
|---|---|
| Diaphoresis, pale/cool/clammy skin | Sympathetic activation; marker of significant ischemia |
| Sinus tachycardia | Compensatory; common in large infarcts or pain response |
| Bradycardia (HR <60) | RCA occlusion → inferior MI → AV nodal ischemia (vagal effect) |
| Hypertension | Sympathoadrenal surge; common early |
| Hypotension | Cardiogenic shock, RV infarction, or vagal reaction |
| Tachypnea | Secondary to pulmonary congestion or pain |
"If the patient has a large area of myocardial ischemia or a large NSTEMI, the physical findings can include diaphoresis; pale, cool skin; sinus tachycardia; a third and/or fourth heart sound; basilar rales; hypotension; and in severe cases, cardiogenic shock." — Harrison's Principles of Internal Medicine 22E
Jugular Venous Pressure (JVP)
- Elevated JVP → Left heart failure with raised filling pressures; or RV infarction
- RV infarction triad (complicates inferior MI): hypotension + elevated JVP + clear lung fields
- Kussmaul's sign (JVP rises on inspiration) may be present in RV infarction
Precordial Examination
Inspection & Palpation
- Dyskinetic apical impulse — paradoxical outward movement of infarcted segment during systole; indicates large anterior wall MI / LV aneurysm
- Displaced apex beat — suggests LV dilatation from prior infarction or acute severe dysfunction
- May be normal in small infarcts
Auscultation — Heart Sounds
S1 and S2
- Soft S1 — reduced contractility of the ischemic myocardium reduces mitral valve closing force
- Paradoxical splitting of S2 — if LBBB or severe LV dysfunction delays aortic valve closure
S4 Gallop (Atrial Gallop) — Very Common
- Present due to reduced LV compliance from ischemia/infarction
- Heard in late diastole (pre-systole), best at the apex with the bell
- Can be normal in elderly individuals, so less specific in isolation
- Represents atrial kick into a stiff, non-compliant ventricle
S3 Gallop (Ventricular Gallop) — Significant Finding
- Heard in early diastole — due to rapid passive filling of a volume-overloaded or poorly compliant ventricle
- Indicates significant LV dysfunction / heart failure
- Low-pitched, best at apex in left lateral decubitus position
- Associated with higher Killip class and worse prognosis
"The presence of an S3 gallop is useful for detecting left ventricular [dysfunction]" — Goldman-Cecil Medicine
Auscultation — Murmurs
New Systolic Murmur — Always Pathological in ACS Context
Three mechanical complications must be urgently differentiated by echocardiography:
| Complication | Murmur | Timing | Notes |
|---|---|---|---|
| Papillary muscle dysfunction/rupture → Acute MR | Holosystolic, harsh, at apex → axilla | Day 3–5 (rupture); earlier with dysfunction | Posteromedial PM most vulnerable (single blood supply from RCA); sudden pulmonary edema |
| Ventricular Septal Defect (VSD) | Holosystolic, harsh, at lower left sternal border, with thrill | Day 3–5 | Step-up in O₂ saturation from RA to RV on catheterization |
| Free wall rupture → Pseudoaneurysm | May have no murmur; presents as sudden cardiovascular collapse or tamponade | Day 3–7 | Beck's triad if tamponade develops |
"Papillary muscle rupture occurs in approximately 1% of patients with AMI, is more common with inferior myocardial infarction, and usually occurs 3 to 5 days after AMI." — Tintinalli's Emergency Medicine
Soft or Absent Murmur — Do Not Be Falsely Reassured
- In secondary (ischemic) MR, the murmur can be soft and underwhelming despite severe regurgitation, due to reduced ventricular contractility and large regurgitant orifice
- A new murmur + hemodynamic deterioration mandates urgent echo regardless of murmur intensity
Auscultation — Pericardial Rub
- Pericardial friction rub — appears 12 hours to 10 days post-MI (early pericarditis — Dressler-related or direct extension)
- Scratchy, to-and-fro sound; louder on leaning forward
- Three-component rub (systolic, early diastolic, presystolic) is pathognomonic
- In STEMI, early pericarditis (direct) occurs within 24–72 hours over the infarct zone
Lung Examination
| Finding | Significance |
|---|---|
| Basilar crackles (rales) | Pulmonary venous congestion from LV failure |
| Widespread crackles / pulmonary edema | Severe LV failure, large infarct, acute MR or VSD |
| Clear lungs | Uncomplicated ACS OR RV infarction (high JVP + clear lungs) |
Persistent rales above the lung bases post-STEMI is an independent predictor of increased cardiovascular risk.
Peripheral Examination
| Finding | Significance |
|---|---|
| Cold, mottled extremities | Low cardiac output / cardiogenic shock |
| Weak/absent peripheral pulses | Cardiogenic shock or acute limb ischemia (LV thrombus embolization) |
| Peripheral edema | Pre-existing heart failure or evolving failure post-MI |
Killip Classification — Examination-Based Prognostic Staging
| Class | Examination Findings | In-Hospital Mortality |
|---|---|---|
| I | No heart failure; no S3, no rales | ~6% |
| II | Mild-moderate HF; S3 gallop, rales <50% lung fields, or elevated JVP | ~17% |
| III | Severe HF; rales >50% lung fields (pulmonary edema) | ~38% |
| IV | Cardiogenic shock: hypotension (SBP <90), cold skin, oliguria, altered sensorium | ~67–81% |
Summary Table
| Examination Area | Key Finding | What It Tells You |
|---|---|---|
| General | Diaphoresis, pallor | Large ischemic burden |
| Vitals | Tachycardia / Bradycardia | Compensatory / inferior MI/vagal |
| JVP | Elevated, Kussmaul's | RV infarction or severe LHF |
| Precordium | Dyskinetic impulse | LV aneurysm / large anterior MI |
| S4 gallop | LV non-compliance | Ischemia/infarction (common) |
| S3 gallop | Rapid filling / LV dysfunction | Worse prognosis / Killip II+ |
| Soft S1 | Poor contractility | Large infarct |
| New systolic murmur | MR, VSD, free wall rupture | Mechanical complication → urgent echo |
| Pericardial rub | Pericarditis | 12h–10 days post-MI |
| Basilar rales | Pulmonary congestion | LV failure |
Sources: Harrison's Principles of Internal Medicine 22E; ROSEN's Emergency Medicine; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Fuster & Hurst's The Heart, 15th Ed; Textbook of Clinical Echocardiography
This is a shared conversation. Sign in to Orris to start your own chat.