Classification and complications of fractures. Splint and tractions.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
fracture types classification diagram transverse oblique spiral comminuted
Searching Images
Salter Harris epiphyseal fracture classification types children
Searching Images
traction splint femur fracture application Thomas splint
Reading File
I now have comprehensive material from multiple authoritative sources. Here is the complete synthesis:
Fractures: Classification, Complications, Splints & Traction
1. CLASSIFICATION OF FRACTURES
Fractures are classified along several orthogonal axes.
A. By Aetiology / Formation Mechanism
| Type | Description |
|---|---|
| Traumatic | Direct force → transverse or comminuted fracture; indirect force (lever/rotation) → oblique or spiral fracture |
| Pathologic | Minor trauma to diseased bone (metastases, osteomyelitis, osteoporosis, Paget's, osteogenesis imperfecta, bone cysts) |
| Stress (Fatigue) | Repeated sub-maximal loading; classic example is the march fracture (2nd metatarsal in soldiers/runners). Radiographs often negative early; bone scan or MRI is more sensitive |
Pathologic fractures may occur without any significant trauma and must be suspected when the mechanism is inconsistent with the injury. — Tintinalli's Emergency Medicine, p. 1808
B. By Fracture Morphology (Pattern of the Fracture Line)
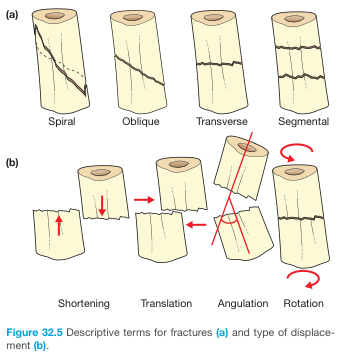
| Pattern | Description |
|---|---|
| Transverse | Fracture line ⊥ long axis; result of direct blow |
| Oblique | Diagonal fracture line; angulated force |
| Spiral | Winds around the shaft; rotational (torque) mechanism |
| Comminuted | >2 fragments (>6 fragments in some definitions); high-energy impact |
| Segmental | Two separate fracture lines create a free-floating segment |
| Avulsion | Fragment pulled off by ligament/tendon insertion |
| Bending/Wedge | Bending force creates a third triangular fragment |
| Greenstick | Cortex fractures on tension side, periosteal tube intact; children only |
| Torus (Buckle) | Cortex buckles on compression side without complete break; children only |
— General Anatomy and Musculoskeletal System, THIEME Atlas, p. 72
C. By Soft-Tissue Integrity (Open vs. Closed)
Closed fracture – skin intact over fracture site.
Open fracture – any wound communicating with the fracture (including small puncture wounds from protruding bone that recedes back). Major risk: osteomyelitis.
Gustilo-Anderson Open Fracture Classification
| Grade | Wound / Energy | Features |
|---|---|---|
| I | <1 cm; low energy | Minimal contamination |
| II | 1–10 cm; moderate | Some comminution, some contamination |
| IIIA | >10 cm; high energy | Gross contamination, adequate bone coverage |
| IIIB | >10 cm; high energy | Exposed bone, periosteal stripping |
| IIIC | Similar to IIIB | + Vascular involvement requiring repair |
— Tintinalli's Emergency Medicine, p. 1809
D. By Location Along the Bone
- Epiphyseal – involving the articular end
- Metaphyseal – flared region near the growth plate
- Diaphyseal – shaft
Also distinguished as proximal / mid-shaft / distal and intra-articular vs. extra-articular.
E. By Displacement
Fracture fragments may be:
- Translated – shifted sideways
- Angulated – angled relative to axis
- Shortened (overlapping) – due to muscle spasm/pull
- Rotated – twisted on the long axis
— Bailey & Love's Short Practice of Surgery, p. 442
F. Salter-Harris Classification (Paediatric Physeal Fractures)
Epiphyseal plate fractures cannot occur in fully-grown adults. Growth plate damage may disrupt future bone elongation.
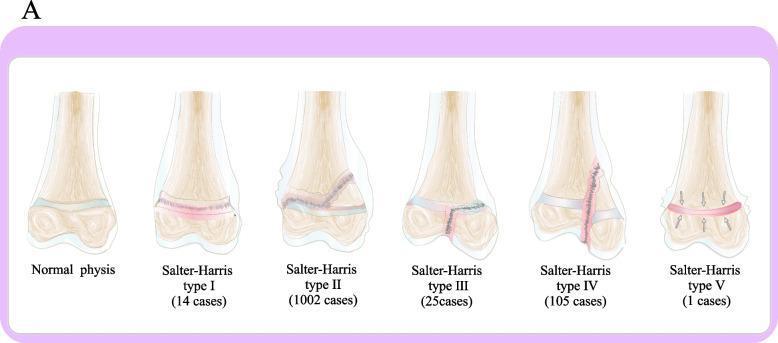
| Type | Fracture Path | Mnemonic (SALTR) | Risk of Growth Disturbance |
|---|---|---|---|
| I | Through physis only (separation) | Slip | Low |
| II | Physis + metaphysis (Thurston-Holland fragment) | Above | Low–moderate; most common (~75%) |
| III | Physis + epiphysis (intra-articular) | Lower | Moderate |
| IV | Crosses metaphysis + physis + epiphysis | Through | High |
| V | Crush/compression of physis | Ram | High; often missed acutely |
— Tintinalli's Emergency Medicine, p. 1814–1815
G. AO/OTA Classification
The AO (Arbeitsgemeinschaft für Osteosynthesefragen) / OTA system classifies fractures alphanumerically by bone (number), segment (1=proximal, 2=diaphysis, 3=distal), and fracture type (A=simple, B=wedge, C=complex/comminuted). This is the internationally standard system used for research and surgical planning. — Rockwood & Green's Fractures in Adults, 10th ed.
2. FRACTURE HEALING
Three overlapping phases:
- Inflammatory phase – haematoma, neutrophils/macrophages, cytokine release, revascularisation begins
- Reparative phase – granulation tissue, callus formation (collagen → cartilage → woven bone); necrotic bone ends resorbed by osteoclasts (creates the radiographic fracture line if initially invisible)
- Remodelling phase – longest phase (years); callus resorbed, trabecular bone laid along stress lines
Healing terms:
| Term | Definition |
|---|---|
| Union | Complete healing |
| Delayed union | Prolonged healing (typically >6 months) |
| Malunion | Healed with residual deformity |
| Nonunion | Failed healing, usually from poor vascularity or instability |
— Tintinalli's Emergency Medicine, p. 1809
3. COMPLICATIONS OF FRACTURES
Immediate (at time of injury)
- Haemorrhage – a closed femur fracture can lose 1–2 L into the thigh; open fractures carry higher risk
- Neurovascular injury – nerve or vessel damage at the fracture site or nearby joint (e.g., axillary nerve with shoulder fracture/dislocation, popliteal artery with knee dislocation, anterior interosseous nerve with supracondylar fractures)
- Skin/soft tissue damage – tenting of skin by bone fragment can convert a closed fracture to an open one
Early (hours to days)
- Compartment syndrome – rising pressure within a closed fascial compartment → ischaemia. Classic 6 P's: Pain (out of proportion, with passive stretch), Pressure, Paraesthesia, Paralysis, Pallor, Pulselessness. Orthopaedic emergency requiring fasciotomy
- Fat embolism syndrome – fat globules from marrow enter circulation; presents 24–72 h post-fracture with hypoxia, confusion, petechial rash (especially long-bone and pelvic fractures)
- Vascular thrombosis / DVT – immobility after fracture
- Infection / wound contamination (open fractures)
Late (weeks to months)
- Osteomyelitis – especially with open fractures; can be chronic and lead to amputation
- Avascular necrosis (AVN) – disruption of blood supply; classic sites: femoral head (neck of femur fracture, hip dislocation), scaphoid (proximal pole), lunate
- Nonunion / malunion – inadequate immobilisation, infection, poor blood supply, excessive distraction, smoking, diabetes, steroids
- Post-traumatic osteoarthritis – intra-articular fractures with residual incongruity
- Complex Regional Pain Syndrome (CRPS) / reflex sympathetic dystrophy – burning pain, allodynia, autonomic changes
- Growth disturbance – paediatric physeal injuries (Salter III–V)
- Contracture / stiffness – prolonged immobilisation (especially knee)
- Implant failure / refracture – after hardware removal
4. SPLINTS
Splinting is the first-line immobilisation in acute fractures. Unlike circumferential casts, splints allow for swelling without vascular compromise.
General Principles
- Immobilise the joint above and below the fracture
- Apply adequate padding (especially bony prominences)
- Maintain proper positioning while the material sets
- Assess neurovascular status before and after application
Common Splint Types
| Splint | Indication | Position |
|---|---|---|
| Shoulder immobiliser | Clavicle, proximal humerus, reduced shoulder dislocations | Arm adducted, internally rotated at side |
| Arm sling | Radial head fractures, supplementary support | Elbow ~90° flexion, forearm neutral |
| Long-arm gutter splint | Elbow and forearm injuries | Elbow ~90°, palm facing abdomen |
| Short-arm splint | Distal radius / wrist | Wrist in neutral or slight extension |
| Thumb spica | Scaphoid, 1st metacarpal (Bennett's), thumb fractures | Thumb abducted |
| Knee immobiliser | Tibial plateau, patellar fractures, ligamentous injuries | Knee in extension |
| Posterior ankle mold | Ankle fractures, severe sprains | Ankle at 90° (neutral dorsiflexion) |
| Prefabricated leg splint | Tibia/fibula fractures | Neutral alignment |



— Tintinalli's Emergency Medicine, p. 1818–1820
5. TRACTION SPLINTS
Historical Context
The traction splint was developed by Sir Hugh Owen Thomas in the late 1800s for femoral fractures. Modified to a half-ring design by Robert Jones, it reduced WWI femoral fracture mortality from 80% to 15%.
Purpose
Traction splints counteract the powerful thigh muscles that shorten a fractured femur, causing the thigh to lose its cylindrical shape and accumulate 1–2 L of blood. By restoring anatomical alignment, they:
- Reduce haemorrhage (increase tissue pressure, decrease dead space)
- Relieve pain
- Prevent neurovascular damage
- Reduce incidence of fat embolism

Indication
Isolated midshaft femur fracture (primary indication)
Contraindications
- Pelvic fractures
- Hip injuries with gross displacement
- Significant knee injuries
- Ankle/foot avulsion or amputation
- Associated distal tibia-fibula or ankle fracture in the same extremity (traction will distract that fracture)
- Open femur fracture — use with caution; consider only if definitive care is significantly delayed
Common Traction Splint Devices
| Device | Design |
|---|---|
| Hare Traction Splint | Half-ring; causes ~30° hip flexion |
| Kendrick Traction Device (KTD) | Compact half-ring |
| Ferno-Trac (Ferno-Washington) | Half-ring variant |
| Sager Emergency Traction Splint | No half-ring; no hip flexion; can be used bilaterally |
Application Principles (Ferno Traction Splint)
- Apply ankle hitch around posterior of heel; D-ring positioned inferiorly
- One rescuer maintains manual traction while lifting the leg
- Slide splint under patient with ischial pad seated firmly against ischial tuberosity
- Attach traction hook to D-ring; turn traction dial until leg resumes normal length (compare with uninjured side)
- Secure 4 Velcro straps (2 above, 2 below knee)
- Reassess neurovascular status
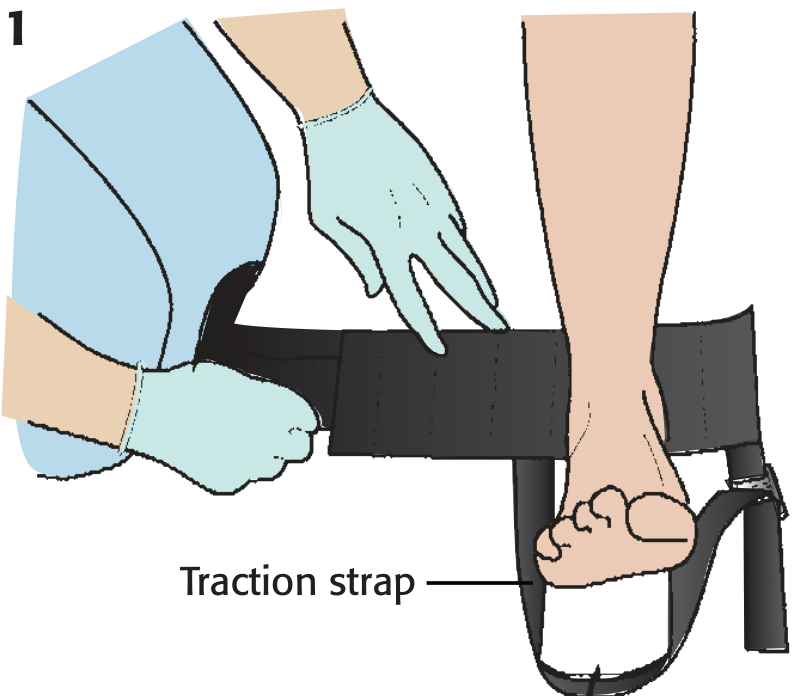
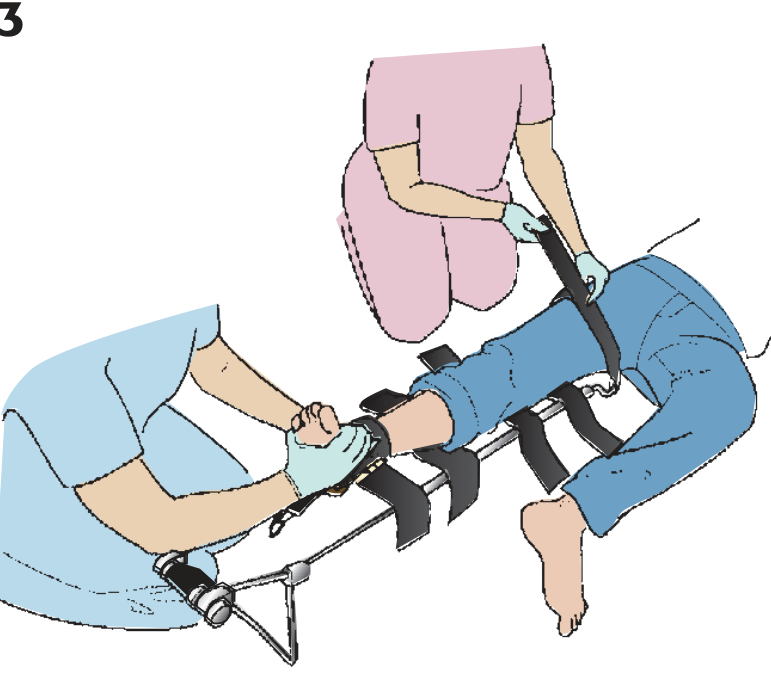
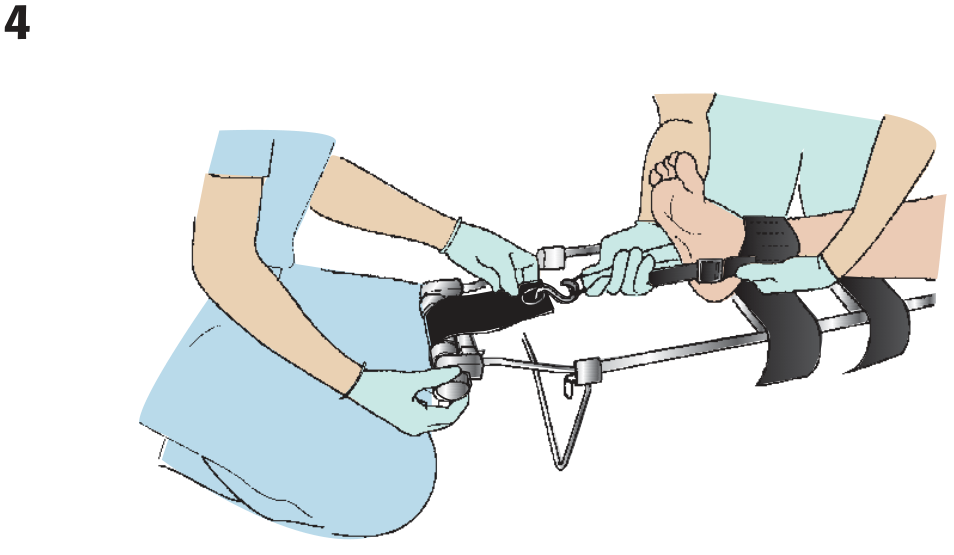
— Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1078–1084
Site-Based Immobilisation Summary
| Site | Preferred Method |
|---|---|
| Hip | Leg-to-leg strapping + full body immobilisation |
| Midshaft femur | Traction splint (first choice); rigid splint if contraindicated |
| Knee | Cardboard or vacuum splint in position found |
| Tibia/fibula | Cardboard, air, or vacuum splint |
| Ankle | Pillow, cardboard, or air splint |
| Foot | Pillow or air splint |
| Toe | Buddy-taping to adjacent toe |
Sources:
- General Anatomy and Musculoskeletal System — THIEME Atlas of Anatomy, pp. 72–73
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, pp. 1808–1820
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, pp. 1078–1086
- Rockwood & Green's Fractures in Adults, 10th ed., Chapter 2
- Bailey & Love's Short Practice of Surgery, 28th ed., pp. 442–444
This is a shared conversation. Sign in to Orris to start your own chat.