Explain me peritonitis for inicet all thing's
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full INICET-focused response.
Peritonitis - Complete INICET Review
1. Definition
Peritonitis is inflammation of the peritoneum - the largest serous membrane of the body (surface area ~1.8 m²). It can be localised or diffuse, acute or chronic, and bacterial or non-bacterial.
- Bailey & Love's Short Practice of Surgery, p. 1109
2. Classification (Most Important for INICET)
A. By Source (Primary vs Secondary vs Tertiary)
| Type | Definition | Key Features |
|---|---|---|
| Primary (SBP) | No obvious intraabdominal source | Cirrhosis + ascites; single organism; no anaerobes |
| Secondary | From intraabdominal viscus or perforation | Polymicrobial; anaerobes present |
| Tertiary | Persistent infection after adequate treatment | Often resistant organisms; poor prognosis |
B. By Extent
-
Localised: Only one area of peritoneum inflamed; involuntary guarding and rebound tenderness in that area
-
Diffuse/Generalised: Entire peritoneal cavity involved; "board-like" rigidity; life-threatening
-
Harrison's Principles of Internal Medicine 22E, p. 1113
3. Causes of Peritonitis
Bacterial (most common)
| Path of Infection | Examples |
|---|---|
| GI perforation | Perforated peptic ulcer, appendix, diverticulum |
| Transmural translocation (no perforation) | Pancreatitis, ischaemic bowel, SBP |
| Exogenous contamination | Drains, open surgery, trauma, peritoneal dialysis |
| Female genital tract | Pelvic inflammatory disease |
| Haematogenous spread | Rare, septicaemia |
Non-bacterial
-
Chemical: Bile peritonitis, barium, pancreatic enzymes (sterile peritonitis)
-
Allergic: Starch peritonitis
-
Traumatic: Operative handling
-
Ischaemic: Strangulated bowel, vascular occlusion
-
Endometriosis: Haemorrhage into peritoneal cavity
-
Ruptured dermoid cysts: Release keratins - intense granulomatous reaction
-
Miscellaneous: Familial Mediterranean fever
-
Bailey & Love, p. 1109; Robbins Pathologic Basis of Disease
4. Organisms Involved
Secondary Peritonitis (polymicrobial)
- Gram-negative: E. coli (most common), Klebsiella
- Gram-positive: Streptococci, Staphylococcus aureus, Enterococci
- Anaerobes: Clostridium perfringens, Bacteroides (rule in secondary; rule out primary)
Primary (Spontaneous) Bacterial Peritonitis (SBP)
-
Single organism (key feature!)
-
E. coli (most common), Streptococci, Klebsiella, Pneumococci
-
Anaerobes are rare - if present, reconsider diagnosis!
-
Harrison's 22E, p. 1114; Robbins
5. Pathogenesis of SBP (INICET Favorite)
SBP occurs in cirrhosis with ascites (in ≤10% of cirrhotic patients) via:
- Altered gut microbiota (Enterobacteriaceae overgrowth)
- Small intestinal bacterial overgrowth
- Deficiency in Paneth cell defensins
- Portal hypertensive enteropathy
- Bacterial translocation → haematogenous seeding of ascites
- Defective complement and opsonisation in ascitic fluid (low protein)
- Reduced PMN phagocytic activity in advanced liver disease
Also seen in: nephrotic syndrome (children), congestive heart failure, SLE, lymphedema, viral hepatitis.
- Harrison's 22E, p. 1113
6. Pathology / Morphology (Robbins)
-
Dense collections of neutrophils + fibrinopurulent debris coating viscera and abdominal wall
-
Serous fluid accumulates → becomes suppurative as infection progresses
-
Subhepatic and subdiaphragmatic abscesses may form
-
Except in tuberculous peritonitis, reaction usually remains superficial (does NOT penetrate gut wall)
-
Fibrin plaques cause bowel loops to adhere to each other and to parietes
-
Inflamed peritoneum appears: reddened, thickened, velvety texture
-
Robbins, Cotran & Kumar Pathologic Basis of Disease
7. Clinical Features
Localised Peritonitis
- Pain in the affected area (somatic pain from parietal peritoneum)
- Involuntary guarding - reflex abdominal wall contraction
- Rebound tenderness (Blumberg's sign) - pain worsens on releasing hand
- Phrenic/shoulder-tip pain - if subdiaphragmatic (referred to C5 dermatome)
- Pelvic peritonitis - deep tenderness on rectal/vaginal examination
Diffuse (Generalised) Peritonitis
- Acute, severe abdominal pain - worse on movement, coughing, deep respiration
- "Hippocratic facies" - patient gravely ill looking, lies still
- "Board-like rigidity" - entire abdomen hard on palpation
- Scaphoid abdomen - in thin patients (rectus muscle contraction)
- Constitutional: anorexia, malaise, fever, nausea/vomiting
- Absent/reduced bowel sounds (paralytic ileus)
- Vital signs: tachycardia, pyrexia, hypotension (in advanced cases)
- Late: septic shock, SIRS, MODS → loss of consciousness
Signs may be diminished in obese patients or those on immunosuppressive medications - important INICET catch!
- Bailey & Love, p. 1109-1110
8. Diagnosis
Laboratory
- CBC: leukocytosis (raised WBC)
- CRP/ESR: elevated
- LFTs, RFTs, electrolytes, blood cultures
- Ascitic fluid tap (MOST IMPORTANT for SBP):
- >250 PMNs/μL = diagnostic for SBP ✓
- Culture (inoculate 10 mL directly into blood culture bottle - improves yield)
- Culture before starting antibiotics
Imaging
| Investigation | Finding |
|---|---|
| Erect CXR | Free air under diaphragm (pneumoperitoneum) - perforation |
| Lateral decubitus X-ray | Alternative if patient too ill for erect position |
| CT abdomen (investigation of choice) | Identifies source, free fluid, abscesses |
| Ultrasound | Useful for tubo-ovarian pathology; less specific otherwise |
| Laparoscopy | If above inconclusive |
Normal peritoneal fluid: protein <30 g/L, WBC <300/μL (mostly mononuclear)
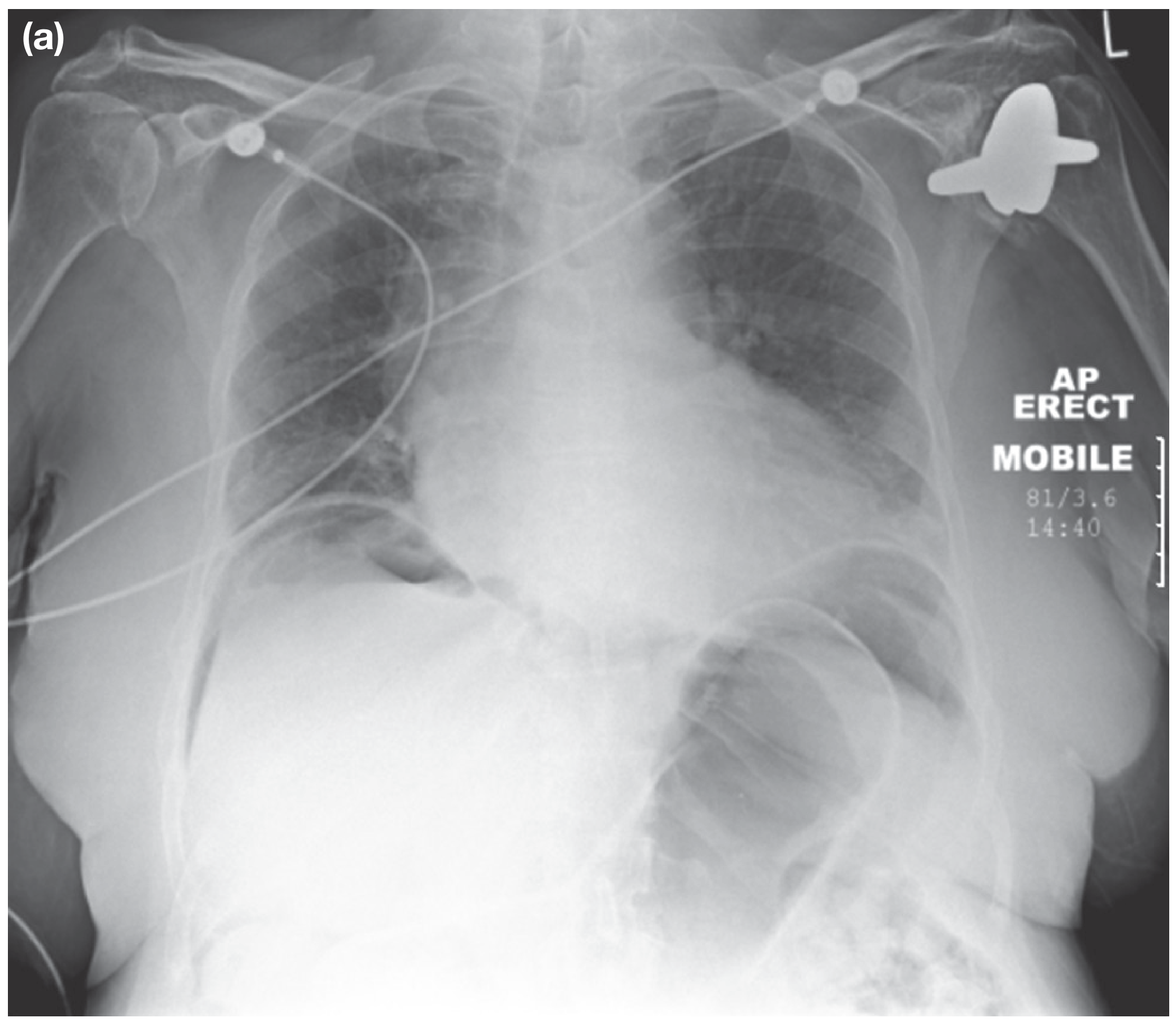
Erect CXR showing pneumoperitoneum - Bailey & Love
- Harrison's 22E, p. 1114; Bailey & Love, p. 1110
9. Treatment
A. Primary (SBP) Treatment
Empirical antibiotics (before culture results):
- Cefotaxime 2g q8h IV - first line (3rd-gen cephalosporin), covers gram-negative bacilli + gram-positive cocci
- Ceftriaxone 2g q24h IV - alternative
- Piperacillin/tazobactam 3.375g q6h IV - broad spectrum option
- Vancomycin - for prior MRSA infection/colonisation
- No need to cover anaerobes in SBP!
- Duration: minimum 5 days if rapid improvement + blood cultures negative; up to 2 weeks if bacteremia or slow improvement
Albumin infusion (mortality benefit - INICET HIGH YIELD):
- 1.5 g/kg IV within 6 hours of detection
- 1.0 g/kg IV on day 3
- Greatest benefit when: creatinine ≥1 mg/dL, BUN ≥30 mg/dL, or total bilirubin ≥5 mg/dL
- Reduces risk of hepatorenal syndrome and mortality
SBP Prophylaxis:
- Norfloxacin (long-term prophylaxis in high-risk cirrhotic patients)
- However, overuse → increased ESBL-producing organisms
B. Secondary Peritonitis Treatment (Surgical)
General (resuscitation first):
- Fluid and electrolyte correction
- Nasogastric tube insertion
- Urinary catheter
- Broad-spectrum antibiotics
- Analgesia
- Vital system support (ICU if needed)
Surgical:
- Source control - remove/exclude cause (close perforation, resect gangrenous bowel)
- Peritoneal lavage ± drainage
- Time is critical - expedient surgical intervention saves lives
Antibiotic choice for secondary peritonitis:
-
Must cover gram-negative aerobes + anaerobes (Bacteroides fragilis)
-
Options: beta-lactam/beta-lactamase inhibitor combinations, carbapenems
-
Duration: 4-5 days with adequate source control
-
Most failures = failure to achieve source control / drain abscess
-
Harrison's 22E, p. 1114-1116; Bailey & Love, p. 1110
10. Special Types (INICET MCQ Favorites)
Tuberculous Peritonitis
- Reaction penetrates deeply (unlike other peritonitis)
- Ascites, fever, weight loss, night sweats
- Laparoscopy with biopsy for diagnosis
Bile Peritonitis
- Chemical/sterile peritonitis initially
- Very irritating; usually complicated by bacterial superinfection
- From biliary system perforation/rupture
Starch Peritonitis
- Granulomatous reaction to surgical glove starch
- Type of foreign body peritonitis
Spontaneous Bacterial Peritonitis vs Secondary Peritonitis - Key Differentiator
| Feature | SBP | Secondary |
|---|---|---|
| Organisms | Single organism | Polymicrobial |
| Anaerobes | Rare | Present |
| Source | No intraabdominal source | Intraabdominal source |
| Treatment | Antibiotics alone | Surgery + antibiotics |
| Ascitic PMN | >250/μL diagnostic | Not diagnostic criterion |
Familial Mediterranean Fever
- Genetic cause of recurrent peritonitis episodes
- Autosomal recessive; mutation in MEFV gene (pyrin protein)
CAPD-associated Peritonitis
- From peritoneal dialysis catheter contamination
- Staphylococcus epidermidis, S. aureus common
11. Prognosis
- SBP: In-hospital mortality ~17.6%; 30-day mortality ~23% at tertiary centers
- Reflects advanced underlying liver disease
- Diffuse secondary peritonitis: Life-threatening; MODS/septic shock if not treated urgently
- Intraabdominal abscess: Treatment failure most often = failure to drain
12. Key INICET Points Summary
| Point | Fact |
|---|---|
| Diagnostic criterion for SBP | >250 PMNs/μL in ascitic fluid |
| Most common organism in SBP | E. coli |
| First-line antibiotic for SBP | Cefotaxime 2g q8h IV |
| Albumin dose in SBP | 1.5 g/kg at 0h + 1.0 g/kg at day 3 |
| Peritonitis that penetrates bowel wall | Tuberculous peritonitis |
| Single organism in peritonitis | Primary (SBP) |
| Polymicrobial + anaerobes | Secondary peritonitis |
| Investigation of choice | CT abdomen |
| Sign of perforation on CXR | Free air under diaphragm |
| Board-like rigidity | Diffuse peritonitis |
| "Hippocratic facies" | Diffuse peritonitis (patient lies still) |
| Referred shoulder-tip pain | Subdiaphragmatic peritonitis (C5 dermatome) |
| Morphology | Neutrophilic infiltrate + fibrinopurulent debris |
| Surface area of peritoneum | 1.8 m² |
| Starch peritonitis type | Granulomatous reaction |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 137
- Bailey and Love's Short Practice of Surgery 28th Edition, Chapter 65
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 39
- Goldman-Cecil Medicine International Edition
This is a shared conversation. Sign in to Orris to start your own chat.