Local aneasthesia for fibroadenoma how to give it
Reading File
Finding Sources
Finding Sources
Searching the Web
local anesthesia technique fibroadenoma excision breast surgery
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have comprehensive information. Let me now compile the full answer.
Local Anaesthesia for Fibroadenoma Excision
Fibroadenoma excision is well-suited to local anaesthesia (LA), particularly for small-to-moderate sized (<3-4 cm), palpable masses. Large or giant fibroadenomas may need sedation or general anaesthesia.
Agent/Drug of Choice
The standard preparation is a mixture of a short-acting and a long-acting local anaesthetic with epinephrine:
| Component | Example | Purpose |
|---|---|---|
| Short-acting LA | 1% Lidocaine (Lignocaine) | Rapid onset |
| Long-acting LA | 0.25-0.5% Bupivacaine | Prolonged postop analgesia |
| Vasoconstrictor | Epinephrine 1:100,000 - 1:200,000 | Reduces bleeding, prolongs duration |
| Alkalinising agent | 8.4% Sodium Bicarbonate (10:1 ratio) | Reduces stinging on injection |
A practical mix: 1% lidocaine with 1:100,000 epinephrine, buffered 10:1 with 8.5% NaHCO₃ (reduces pain of injection significantly).
Maximum dose: Lidocaine with epinephrine - up to 7 mg/kg (plain lidocaine - 3-4 mg/kg). Total volume for a breast lump excision is typically 10-20 mL.
Technique: Field Block (NOT direct infiltration over the mass)
The key principle is a field block / perimeter infiltration - inject around the borders of the mass, NOT directly into it. Injecting on top of the mass:
- Distorts the tissue making palpation impossible
- Spreads into the tumour potentially causing rupture
- Makes orientation and excision harder
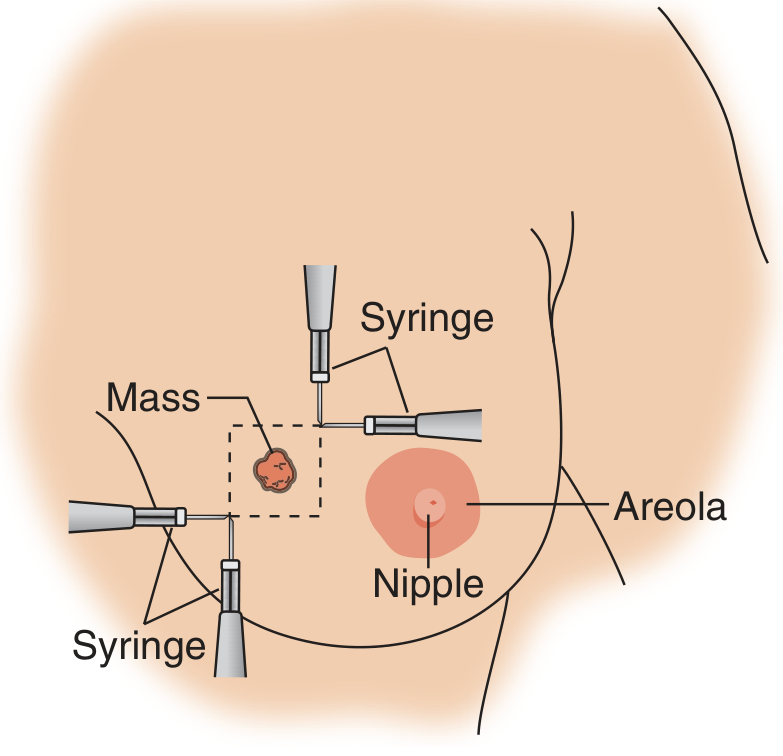
Field block technique: Inject around all 4 borders of the mass (dashed square), keeping the mass palpable in the center. - Pfenninger & Fowler's Procedures for Primary Care
Step-by-Step Injection Technique
1. Mark the mass and incision first
- With the patient awake, palpate and mark the mass borders and planned incision with a surgical marking pen before giving LA (which can distort landmarks).
2. Skin wheal at incision site
- Raise an intradermal wheal at the planned incision site using a fine 25-27G needle. This is the most painful injection - go slowly.
3. Subcutaneous infiltration along incision line
- Inject along the full length of the planned incision subcutaneously.
4. Deep perimeter block (field block)
- Using a 22G spinal or long needle, insert through the wheal and advance in the subcutaneous plane along each side of the mass border.
- Inject while withdrawing the needle (not while advancing - reduces intravascular injection risk).
- Cover all 4 sides of the mass (superior, inferior, medial, lateral), staying 1-2 cm peripheral to the mass edge.
5. Deep layer infiltration
- Infiltrate into the deeper breast parenchyma along the expected dissection plane, at the level just below the mass. This anaesthetises deeper sensory branches.
6. Wait
- Allow 3-5 minutes for the LA to take full effect before incising. Epinephrine takes 7-10 minutes for full vasoconstriction - waiting improves haemostasis.
7. Intraoperative top-up
- Additional LA can be injected into deeper layers as needed during dissection, especially as the dissection plane goes deeper around the mass.
Injection Technique Tips
- Aspirate before injecting each time - the breast has a rich vascular supply; intravascular injection of LA is dangerous.
- Warm the solution slightly to body temperature - reduces stinging.
- Use the sodium bicarbonate buffer (10 mL lidocaine : 1 mL 8.4% NaHCO₃) - significantly reduces pain.
- Inject slowly and use the smallest gauge needle tolerated.
- For periareolar incisions: also infiltrate the subareolar plane as the areola has distinct innervation.
Incision Placement (affects where you anaesthetise)
| Location of mass | Preferred incision | LA field |
|---|---|---|
| Upper breast | Curvilinear, along Langer's lines | Along Langer's lines + field block |
| Lower breast | Radial incision | Radial + deep field block |
| Any location | Periareolar (if close enough) | Circumareolar plane + field block |
When to Upgrade Anaesthesia
Consider IV sedation or GA if:
- Mass >4-5 cm (giant fibroadenoma / phyllodes)
- Deep-seated lesion near chest wall
- Patient anxiety is high
- Non-palpable lesion requiring wire/seed localisation
- Multiple lesions being excised
For very large fibroadenomas, Pecs II block or thoracic spinal anaesthesia are described regional alternatives that provide excellent coverage without GA.
Sources:
- Pfenninger & Fowler's Procedures for Primary Care, 3e, p. 926-928
- Mulholland & Greenfield's Surgery, 7e, p. 3886-3887 (Excisional Biopsy technique)
- S Das, A Manual on Clinical Surgery, 13e, p. 434
Step-by-step surgical technique for fibroadenoma excision
Finding Sources
Finding Sources
Searching the Web
fibroadenoma excision step by step surgical technique enucleation
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Excellent - I have all the images and content needed for a comprehensive answer. Here it is:
Step-by-Step Surgical Technique for Fibroadenoma Excision
Indications for Surgery
Surgical excision is indicated when the fibroadenoma is:
- Size >3 cm (most agree) or >5 cm (Bailey & Love)
- Rapid growth (>20% increase in 6 months)
- Patient age >30 years
- Suspicious features on imaging (microlobulation)
- Atypia on core biopsy
- Family history of breast cancer
- Patient preference / significant anxiety
For elderly patients, always excise with a rim of normal tissue - the mass may contain malignancy or be a phyllodes tumour. In young women with a typical fibroadenoma, simple enucleation is acceptable.
Preoperative Preparation
- Mammogram for all women >30 years before the procedure (to rule out occult synchronous lesions)
- Ultrasound to confirm the mass is solid, well-marginated, benign-appearing
- Core needle biopsy (ideally done before surgery) to confirm histology
- Mark the mass with indelible ink before sedation/LA is given, with the patient awake and in the operative position
- Obtain written informed consent
Patient Positioning
- Supine, arm on the ipsilateral side abducted to 90 degrees and padded at the elbow and wrist
- Appropriate padding of all pressure points
- Breast prepped with antiseptic and draped in sterile fashion
Step 1: Incision Planning
Choosing the right incision is critical for cosmesis and for preserving future surgical options.
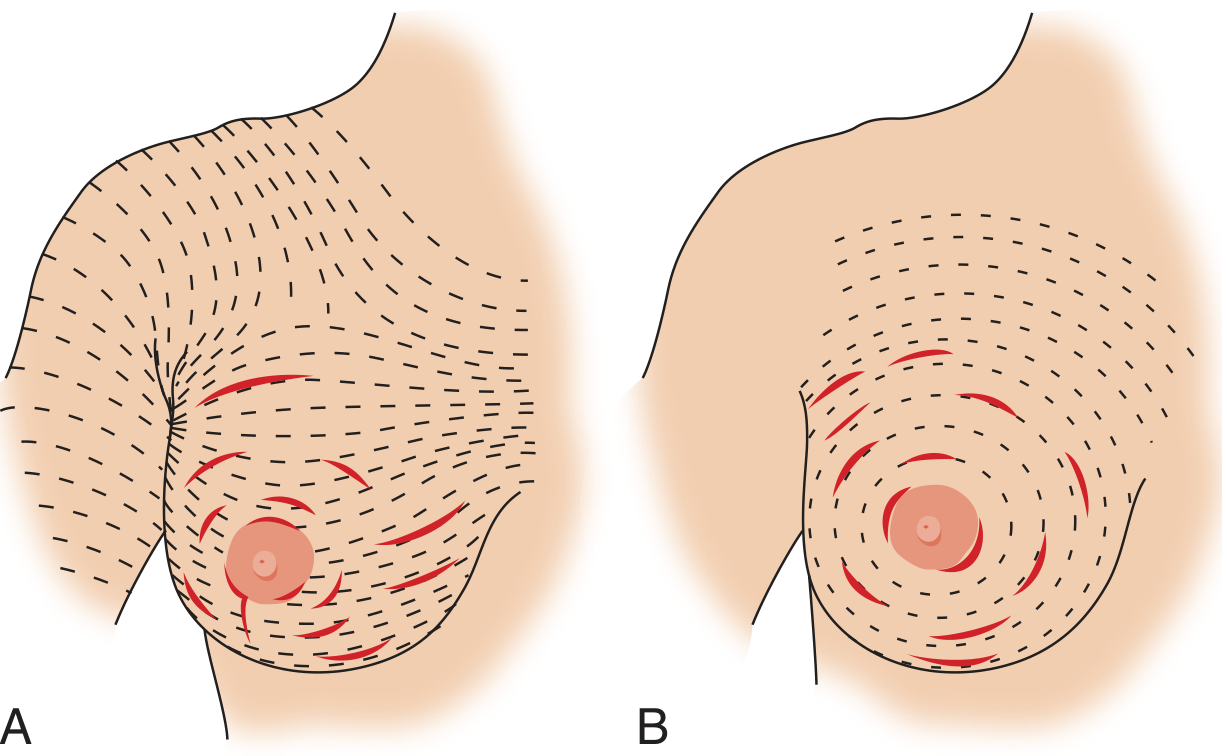
Fig A: Incisions along Langer's lines (curvilinear in upper breast). Fig B: Periareolar/circumareolar incision for masses near the nipple-areolar complex. - Pfenninger & Fowler
| Mass Location | Preferred Incision |
|---|---|
| Upper half of breast | Curvilinear / transverse along Langer's lines |
| Lower half, large mass | Radial incision (better cosmesis when removing volume) |
| Near the nipple, young patient, likely benign | Periareolar / circumareolar |
| Medial breast (in case mastectomy needed later) | Radial (easier to re-excise) |
Mark the incision line and the borders of the mass with a surgical marking pen before giving LA.
Step 2: Local Anaesthesia (Field Block)
- 1% Lidocaine + epinephrine 1:100,000, buffered 10:1 with 8.5% NaHCO₃
- Raise a dermal wheal at the planned incision site
- Infiltrate along the incision line subcutaneously
- Perform a circumferential field block around the mass borders - do NOT inject directly over the mass (distorts it, makes palpation impossible)
- Wait 5-7 minutes before incising
Step 3: Skin Incision
- Incise skin with a No. 15 blade, holding it at right angles to the skin edges (avoids bevelling, which creates uneven wound edges)
- Carry the incision down vertically to the subcutaneous layer
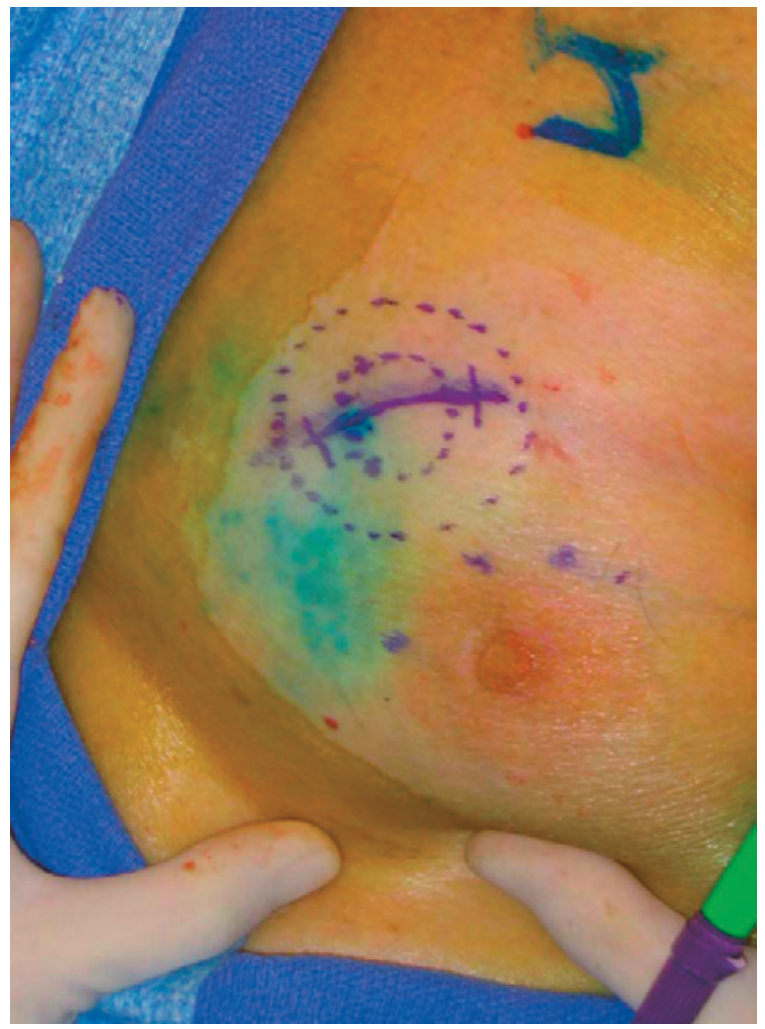
Palpable lesion marked with incision line (curvilinear) and mass border (dotted). - Pfenninger & Fowler
Step 4: Dissection Down to the Mass
- Use tissue scissors or electrocautery to dissect down through the subcutaneous fat to the level of the mass
- Develop thick flaps - as thick as possible while still being able to remove the lesion anteriorly
- Cauterise bleeders with electrocautery at each layer as you go
- Inject additional LA into deeper layers if the patient feels discomfort
Step 5: Enucleation / Excision of the Mass
This is the key step. Fibroadenoma has a well-defined capsule, which allows enucleation (shelling out) in most cases:
- Grasp the mass with an Allis clamp to provide countertraction - this lifts the mass and puts its capsule under tension, making dissection easier
- Using curved tissue scissors, a No. 15 blade, or electrocautery, dissect circumferentially along the plane just outside the capsule
- The fibroadenoma will "pop out" from its capsule when correctly dissected - this is the classic enucleation technique
- Keep dissection close to the capsule to minimise dead space and preserve breast parenchyma
- Do not morcellate the mass (do not cut it into pieces - it must come out intact for proper pathological orientation)
- Benign fibroadenomas: enucleation alone is sufficient
- Elderly patient / suspicious features: excise with a small rim of normal breast tissue (wide local excision margin)
Step 6: Specimen Orientation
- Orient the specimen with marking sutures before sending to pathology:
- Short suture = Superior margin
- Long suture = Lateral margin
- This is essential - if the lesion is found to be malignant on final histology, the pathologist can identify which margin is involved and guide re-excision
- Send all specimens for histopathological evaluation - frozen section is optional (hormone receptor analysis is done on paraffin-embedded tissue)
Step 7: Haemostasis
- Achieve meticulous haemostasis with electrocautery before closure
- Inspect the entire cavity - even small bleeders must be controlled
- Hematoma is the most common complication and can mimic recurrence
Step 8: Wound Closure
Do NOT reapproximate deep breast parenchyma ("dead space") - this is a key principle. Closing the dead space causes:
- Breast distortion and deformity
- Mammographic scarring (difficult future surveillance)
- Dimpling of overlying skin
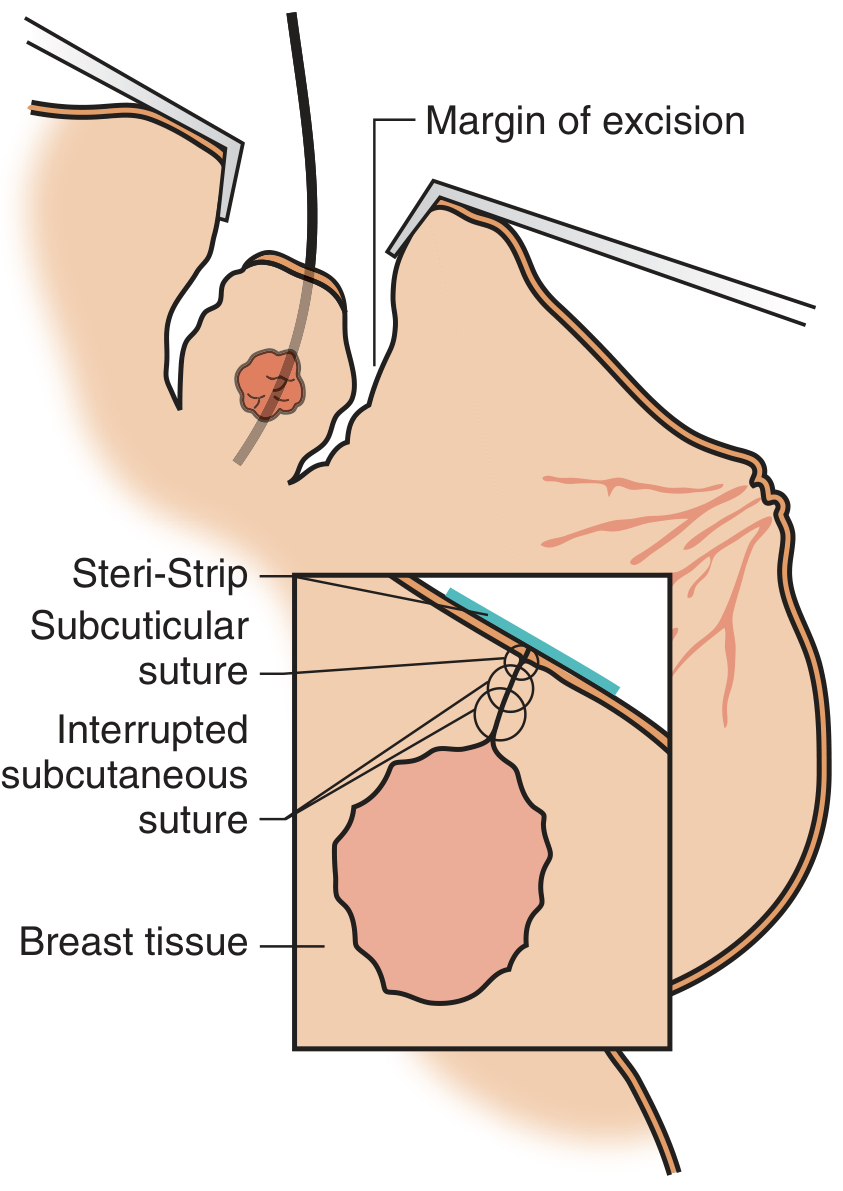
Closure layers: deep breast tissue left open; interrupted subcutaneous Vicryl sutures approximate the subdermal layer; running subcuticular suture closes the skin. - Pfenninger & Fowler
Closure layers:
| Layer | Suture | Technique |
|---|---|---|
| Superficial fascia / subdermal | 3-0 Vicryl (absorbable) | Buried interrupted - do not take large bites (causes dimpling) |
| Skin | 4-0 or 5-0 Monocryl / PDS | Running subcuticular (intracutaneous) |
| Surface | Steri-Strips | Applied across the wound |
- No drains - they are not required for a simple fibroadenoma excision
- Apply a firm supportive dressing and a well-fitting bra postoperatively
Special Case: Giant Fibroadenoma (>5 cm)
- Approach via a submammary (inframammary) incision (Gaillard Thomas incision) for large lesions
- Enucleation is still possible through this hidden incision
- Consider sedation or general anaesthesia for giant fibroadenomas
- Overlying skin may be thin and stretched - check vascularity before closure
Complications to Watch For
| Complication | Management |
|---|---|
| Haematoma | If symptomatic: return to OR, evacuate, cauterise. If small/asymptomatic: supportive bra, reassurance |
| Seroma | Aspiration (send for culture even if clear) |
| Infection | Oral antibiotics for cellulitis; incision and drainage if abscess |
| Skin dimpling | Prevented by not reapproximating deep tissue |
| Recurrence | Incomplete excision; confirm with imaging and re-excise if needed |
| Unexpected malignancy | Specimen orientation guides targeted re-excision |
Sources:
- Pfenninger & Fowler's Procedures for Primary Care, 3e, pp. 926-928
- Mulholland & Greenfield's Surgery, 7e, pp. 3886-3887
- Bailey & Love's Short Practice of Surgery, 28e, pp. 408-424
- Current Surgical Therapy, 14e, pp. 893-895
This is a shared conversation. Sign in to Orris to start your own chat.