Hypertension 20 mark question
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content I need for a comprehensive 20-mark answer on hypertension. Let me compile the answer.
Hypertension - Comprehensive 20-Mark Answer
1. Definition and Classification
Hypertension is defined as a sustained elevation of systemic arterial blood pressure (BP). The 2017 ACC/AHA guidelines define it as an average systolic BP (SBP) ≥130 mmHg and/or diastolic BP (DBP) ≥80 mmHg on two or more occasions.
| Stage | SBP (mmHg) | DBP (mmHg) |
|---|---|---|
| Normal | <120 | <80 |
| Elevated | 120-129 | <80 |
| Stage 1 Hypertension | 130-139 | 80-89 |
| Stage 2 Hypertension | ≥140 | ≥90 |
| Hypertensive Crisis | >180 | >120 |
Hypertensive Urgency: BP >180/120 mmHg without acute target organ damage - managed by gradually lowering BP over 24-48 hours.
Hypertensive Emergency: BP severely elevated WITH acute target organ damage (e.g., aortic dissection, hypertensive encephalopathy, acute pulmonary edema, HELLP syndrome) - requires IV therapy with controlled BP reduction.
(Harrison's Principles of Internal Medicine, 22E)
2. Epidemiology
- Hypertension affects approximately 1.28 billion adults worldwide and is the leading modifiable risk factor for cardiovascular disease (CVD), stroke, renal failure, and premature death.
- It carries a 2.5-fold (men) to 3.9-fold (women) age-adjusted increased risk for peripheral arterial disease.
- Prevalence increases sharply with age, obesity, dietary sodium excess, and physical inactivity.
- African Americans tend to have more severe hypertension and higher rates of target organ damage than other populations.
3. Etiology and Classification
A. Primary (Essential) Hypertension (~90-95%)
No identifiable single cause. Results from a complex interaction of:
- Genetic factors: Polygenic inheritance; multiple modest-effect alleles
- Environmental/Lifestyle factors (the six key modifiable exposures):
- Poor diet quality (low adherence to DASH-style eating)
- Excess body weight / obesity (BMI ≥30)
- Excessive dietary sodium intake
- Insufficient dietary potassium intake
- Physical inactivity (<150 min aerobic exercise/week)
- Alcohol consumption (especially binge drinking)
- Other associations: Heavy metal exposure (lead, mercury, cadmium, arsenic), air pollution (PM2.5 increases SBP by ~3-5 mmHg), high altitudes, cold climate
(Harrison's 22E)
B. Secondary Hypertension (~5-10%)
An identifiable, treatable underlying cause. Should be suspected when:
- Treatment-resistant hypertension (BP >130/80 on 3+ drugs)
- Abrupt worsening of previously controlled hypertension
- Disproportionate target organ damage for BP level
- Lab abnormalities: unprovoked hypokalemia, proteinuria, left ventricular hypertrophy
| Cause | Prevalence | Key Feature |
|---|---|---|
| Renal parenchymal disease | Most common (overall) | Most common in children; proteinuria, GFR reduction |
| Renovascular disease (RAS, FMD) | Common in elderly | Bruit, flash pulmonary edema, worsening renal function on ACEi |
| Primary hyperaldosteronism | 5-15% of resistant HTN | Hypokalemia, adrenal adenoma |
| Obstructive sleep apnea | Very common | Obesity, daytime somnolence, nocturnal HTN |
| Pheochromocytoma | Rare but dangerous | Episodic headache, sweating, palpitations |
| Cushing syndrome | Uncommon | Truncal obesity, striae, moon facies |
| Thyroid disorders | Relatively common | Both hypo- and hyperthyroidism |
| Coarctation of aorta | Young patients | Radio-femoral delay, rib notching |
| Drug-induced | Important | NSAIDs, OCPs, sympathomimetics, cocaine, steroids |
(Harrison's 22E; National Kidney Foundation Primer on Kidney Diseases, 8E)
4. Pathophysiology
Blood pressure = Cardiac Output (CO) x Total Peripheral Resistance (TPR)
Hypertension arises when either or both components are abnormally elevated. Key mechanisms:
Renin-Angiotensin-Aldosterone System (RAAS)
- Increased renin secretion → angiotensin I → angiotensin II (ACE) → vasoconstriction + aldosterone release → sodium/water retention → increased BP.
Sympathetic Nervous System Overactivity
- Enhanced adrenergic tone increases heart rate, CO, and causes arteriolar constriction.
Sodium and Volume Retention
- Impaired renal pressure-natriuresis curve: kidneys maintain sodium retention at inappropriately high BPs.
Endothelial Dysfunction
- Reduced nitric oxide (NO) production, increased endothelin, oxidative stress → decreased vasodilation.
Arterial Stiffness
- Loss of vascular compliance with aging amplifies pulse pressure; stiffened arteries contribute to isolated systolic hypertension and target organ damage.
Insulin Resistance / Metabolic Syndrome
- Associated with elevated angiotensin II, aldosterone, and sympathetic activation.
5. Target Organ Damage (Complications)
| Organ | Complication |
|---|---|
| Heart | Left ventricular hypertrophy (LVH), heart failure (HFpEF and HFrEF), ischemic heart disease, arrhythmias |
| Brain | Ischemic stroke, hemorrhagic stroke, hypertensive encephalopathy, vascular dementia |
| Kidneys | Hypertensive nephrosclerosis, proteinuria, progressive CKD, ESRD |
| Eyes | Hypertensive retinopathy (arteriovenous nicking, flame hemorrhages, papilledema in grade IV) |
| Aorta / Vessels | Aortic dissection, aortic aneurysm, peripheral arterial disease |
6. Clinical Features and Evaluation
Hypertension is largely asymptomatic ("silent killer"). Symptoms, when present, include:
- Headache (typically occipital, worse in the morning)
- Dizziness, tinnitus, epistaxis (less specific)
- Hypertensive urgency/emergency: severe headache, visual disturbance, confusion, chest pain, dyspnea
Evaluation goals:
- Confirm diagnosis (BP measured correctly; two readings at two visits)
- Identify secondary causes
- Assess cardiovascular risk profile and comorbidities
- Identify target organ damage
7. Investigations
| Investigation | Purpose |
|---|---|
| Urinalysis, urine albumin/creatinine ratio | Renal parenchymal disease |
| Serum creatinine, eGFR, electrolytes | Renal function; hypokalemia → hyperaldosteronism |
| Fasting glucose, lipid profile | Cardiovascular risk |
| ECG | LVH, ischemia, arrhythmia |
| Echocardiography | LVH, diastolic dysfunction |
| Fundoscopy | Hypertensive retinopathy grading |
| Thyroid function tests | Thyroid disease as secondary cause |
| Plasma aldosterone/renin ratio | Primary hyperaldosteronism |
| 24-hour urine metanephrines | Pheochromocytoma |
| Renal doppler / CT angiography | Renovascular HTN |
| Serum cortisol, 1 mg overnight DST | Cushing syndrome |
| Ambulatory BP monitoring (ABPM) | White coat HTN, masked HTN, nocturnal dipping pattern |
8. Treatment
A. Non-Pharmacologic (Lifestyle Modifications) - First-line for ALL patients
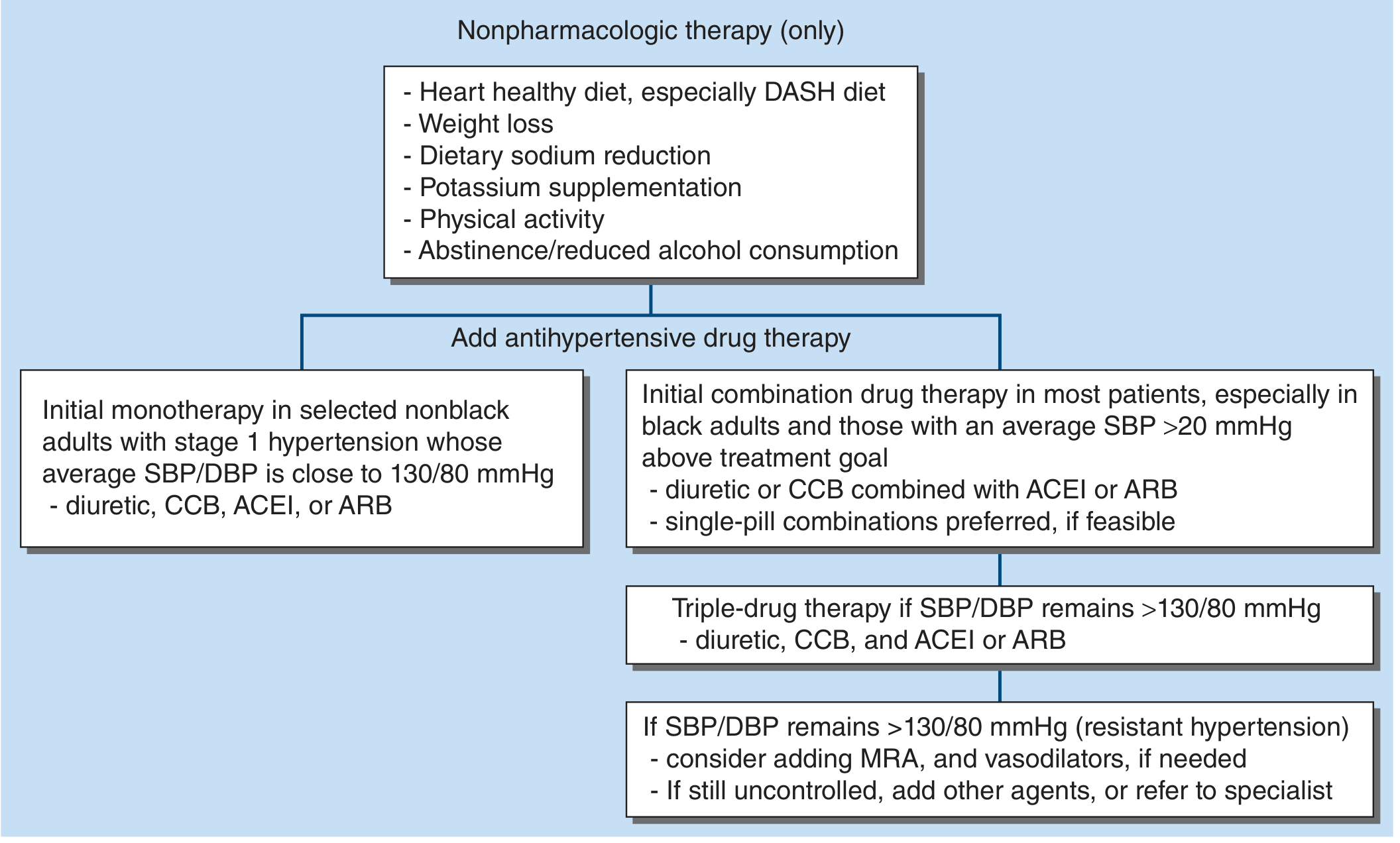
Treatment algorithm for hypertension in adults - Harrison's Principles of Internal Medicine, 22E
- DASH diet (high fruits, vegetables, low saturated fat) - reduces SBP by 8-14 mmHg
- Weight loss (each kg lost lowers SBP by ~1 mmHg)
- Dietary sodium reduction to <2.3 g/day (SBP ↓ 2-8 mmHg)
- Potassium supplementation (3500-5000 mg/day through diet)
- Physical activity ≥150 min/week of moderate aerobic exercise (SBP ↓ 4-9 mmHg)
- Alcohol reduction to ≤2 drinks/day in men, ≤1 in women
B. Pharmacologic Therapy
BP Goal: <130/80 mmHg for most adults (2017 ACC/AHA).
Step 1 - Monotherapy: For Stage 1, non-Black adults with SBP close to 130/80 mmHg.
Step 2 - Initial combination therapy: For most patients, especially Black adults and those with SBP >20 mmHg above goal - diuretic or CCB + ACEi or ARB.
Step 3 - Triple therapy: Diuretic + CCB + ACEi or ARB.
Step 4 - Resistant hypertension: Add mineralocorticoid receptor antagonist (MRA, e.g., spironolactone) + vasodilators.
i. Thiazide Diuretics (e.g., hydrochlorothiazide, chlorthalidone)
- Mechanism: Inhibit NaCl reabsorption in the distal convoluted tubule → ↓ intravascular volume initially → long-term ↓ peripheral vascular resistance
- Use: First-line; useful in combination with most other agents
- Adverse effects: Hypokalemia, hyperuricemia, hyperglycemia, hypercalcemia, hyponatremia
- Caution: Not effective when eGFR <30 mL/min (use loop diuretics instead)
ii. ACE Inhibitors (e.g., enalapril, lisinopril, ramipril)
- Mechanism: Block conversion of angiotensin I → angiotensin II → ↓ vasoconstriction, ↓ aldosterone, ↓ sodium retention
- Compelling indications: CKD with proteinuria, heart failure with reduced EF (HFrEF), post-MI, diabetes with nephropathy
- Adverse effects: Dry cough (most common; 10-15%), angioedema (rare but serious), hyperkalemia, teratogenic (class D/X in pregnancy)
- Contraindications: Pregnancy, bilateral renal artery stenosis, history of angioedema
iii. Angiotensin Receptor Blockers - ARBs (e.g., losartan, valsartan, telmisartan)
- Mechanism: Block AT1 receptors → same effect as ACEi without cough (no bradykinin accumulation)
- Use: Alternative when ACEi not tolerated; same compelling indications
- Adverse effects: Hyperkalemia, angioedema (rare), teratogenic
iv. Calcium Channel Blockers - CCBs
- Dihydropyridines (amlodipine, nifedipine): Selective vascular smooth muscle → vasodilation → ↓ TPR; minimal cardiac effects; long half-life of amlodipine (30-50 hours) allows once-daily dosing
- Non-dihydropyridines - Verapamil and Diltiazem: Both vascular and cardiac effects (negative chronotropy, dromotropy, inotropy); used in AF rate control; avoid in HFrEF
- Adverse effects (DHPs): Peripheral edema, reflex tachycardia, flushing
- Adverse effects (non-DHPs): AV block, constipation (verapamil), bradycardia
- Useful in: Asthma, diabetes, peripheral vascular disease (where beta-blockers are problematic)
v. Beta-Blockers (e.g., metoprolol, atenolol, carvedilol, nebivolol)
- Mechanism: ↓ CO via reduced heart rate and contractility; ↓ renin release → ↓ angiotensin II; ↓ central sympathetic outflow
- Compelling indications: Post-MI, HFrEF (carvedilol, metoprolol succinate, bisoprolol), stable angina
- 3rd generation (nebivolol, carvedilol): Vasodilatory properties (via NO and alpha-blockade respectively)
- Adverse effects: Fatigue, sexual dysfunction, masking of hypoglycemia, bradycardia
- Contraindications: High-degree AV block, non-selective beta-blockers in asthma; caution in diabetes
vi. Mineralocorticoid Receptor Antagonists (e.g., spironolactone, eplerenone)
- Mechanism: Antagonize aldosterone at collecting duct → natriuresis + potassium retention
- Use: Resistant hypertension (evidence-based add-on); also in primary hyperaldosteronism, HFrEF
- Adverse effects: Hyperkalemia, gynecomastia (spironolactone), menstrual irregularities
vii. Alpha-1 Blockers (e.g., doxazosin, prazosin)
- Mechanism: Block alpha-1 receptors → vasodilation
- Additional benefit: Improve benign prostatic hyperplasia (BPH) symptoms
- Caution: First-dose orthostatic hypotension; less recommended as monotherapy
C. Special Situations and Compelling Indications
| Condition | Preferred Drug(s) | Avoid |
|---|---|---|
| CKD / proteinuria | ACEi or ARB | NSAIDs |
| Post-MI | Beta-blocker, ACEi, MRA | - |
| HFrEF | ACEi/ARB, beta-blocker (carvedilol, metoprolol succinate), MRA | Non-DHP CCBs |
| Stable angina | Beta-blocker, CCB | - |
| Atrial fibrillation | Verapamil, diltiazem, beta-blocker | - |
| Diabetes | ACEi/ARB (renoprotective) | - |
| Asthma / COPD | CCB, thiazide, ACEi/ARB | Non-selective beta-blockers |
| Pregnancy | Labetalol, methyldopa, nifedipine | ACEi, ARB |
| Primary aldosteronism | Spironolactone | - |
| Recurrent stroke prevention | Thiazide + ACEi | - |
| Black adults | Thiazide + CCB (less RAAS responsive) | ACEi/ARB monotherapy |
(Lippincott Illustrated Reviews: Pharmacology; Harrison's 22E)
D. Hypertensive Emergency Management
- Goal: Reduce MAP by no more than 25% within the first hour, then to 160/100 mmHg over the next 2-6 hours, then normalize over 24-48 hours (too-rapid reduction risks ischemia due to impaired cerebral autoregulation)
- IV agents:
- Sodium nitroprusside: Arterial and venous dilator; instant onset/offset; use in most emergencies (risk: cyanide toxicity with prolonged infusion)
- Labetalol IV: Alpha + beta blockade; avoid in decompensated HF, asthma
- Nicardipine IV: DHP-CCB; useful in perioperative or stroke hypertension
- Hydralazine IV/IM: Used in hypertensive emergencies in pregnancy
- Clevidipine IV: Ultrashort-acting DHP-CCB
- Esmolol IV: Ultrashort beta-blocker; aortic dissection, perioperative HTN
- Phentolamine: Alpha-blocker; drug of choice in pheochromocytoma crisis
9. Resistant Hypertension
Defined as BP >130/80 mmHg despite use of ≥3 antihypertensives at optimal doses, including a diuretic. Important considerations:
- Exclude pseudo-resistance: poor medication adherence, white coat effect, incorrect BP measurement, suboptimal regimen
- Evidence-based add-on: spironolactone (mineralocorticoid receptor antagonist)
- Consider secondary causes in all resistant hypertension cases
(National Kidney Foundation Primer on Kidney Diseases, 8E; Goldman-Cecil Medicine)
10. Hypertension in Special Populations
| Population | Key Considerations |
|---|---|
| Elderly | Isolated systolic HTN common (↑ arterial stiffness); start low, go slow; caution with orthostasis |
| CKD | ACEi/ARB first-line; target <130/80; monitor potassium and creatinine |
| Diabetes | BP <130/80 mmHg; ACEi/ARB for nephropathy protection |
| Pregnancy | Pre-eclampsia: HTN + proteinuria ≥20 wks gestation; labetalol, methyldopa, or nifedipine; MgSO4 for seizure prophylaxis |
| Children | Increasingly primary; secondary causes (renal, coarctation) must be excluded first |
| Black adults | Higher prevalence and severity; better response to thiazides and CCBs than ACEi/ARB monotherapy; APOL1 risk alleles contribute to nephropathy |
Summary Points for Exam
- Hypertension = "silent killer"; defined as SBP/DBP ≥130/80 mmHg (ACC/AHA 2017)
- Primary (essential) in 90-95%; secondary in 5-10% - always screen for secondary causes in resistant/refractory cases
- Pathophysiology: abnormal CO and/or TPR, RAAS activation, SNS overactivity, sodium retention, endothelial dysfunction
- Complications: cardiac (LVH, HF, IHD), neurological (stroke, encephalopathy), renal (nephrosclerosis, CKD), retinopathy, aortic dissection
- Treatment: lifestyle first; pharmacologically use thiazide, CCB, ACEi, or ARB as first-line; combination preferred over high-dose monotherapy
- Match drug to comorbidity (compelling indications)
- Hypertensive emergency: reduce MAP by max 25% in 1st hour with IV agents
- Resistant hypertension: add spironolactone; rule out secondary causes
Sources: Harrison's Principles of Internal Medicine, 22E | Lippincott Illustrated Reviews: Pharmacology | National Kidney Foundation Primer on Kidney Diseases, 8E | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.