Allantois remnant and omphalomesenric remnant
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the complete answer:
Allantois Remnant and Omphalomesenteric (Vitelline) Duct Remnant
PART 1: ALLANTOIS REMNANT - The Urachus
Embryology
The allantois is a diverticulum arising from the caudal end of the yolk sac that grows into the umbilical cord. During fetal development, it forms the cephalad attachment of the cloaca. As the bladder descends into its pelvic position, the proximal portion of the allantois persists as the urachus, which connects the dome of the bladder to the umbilicus. Normally, the urachus closes and becomes fibrosed, forming the median umbilical ligament. Failure to close results in urachal anomalies.
- Campbell-Walsh-Wein Urology, Urachal Abnormalities section
- Schwartz's Principles of Surgery, 11th ed.
- Robbins & Cotran Pathologic Basis of Disease
Spectrum of Urachal Anomalies
Depending on the extent and location of failure to close, four types of anomaly result:
| Anomaly | Description | Presentation |
|---|---|---|
| Patent urachus (urachal fistula) | Entire urachus remains open | Urine leaking from umbilicus in newborn |
| Urachal cyst | Only the central segment remains patent (both ends close) | Painful infraumbilical/periumbilical fluctuant mass; often due to secondary infection |
| Urachal sinus | Urachus opens at umbilicus but not into bladder | Umbilical discharge |
| Vesicourachal diverticulum | Urachus opens into bladder but not at umbilicus | Hematuria, mucinuria, recurrent UTIs |
Clinical Features
- Most urachal anomalies are asymptomatic and incidentally found on imaging
- When symptomatic: fever, abdominal pain, peri-umbilical fluctuant mass, hematuria, mucinuria, or urine leakage from the umbilicus
- Less often, a calculus may form within the urachus
- The gravest concern is malignant transformation: urachal cysts are lined by urothelial or metaplastic glandular epithelium and carry risk of adenocarcinoma. These account for only 0.1-0.3% of bladder cancers overall but constitute 20-40% of all bladder adenocarcinomas
Robbins & Cotran Pathologic Basis of Disease, p. 885
Investigations
- Ultrasound (initial modality of choice)
- CT scan - best for defining anatomy and extent
- VCUG or sinogram - to evaluate communication with bladder
- Cystoscopy - to inspect the bladder dome for suspicious lesions
Treatment
- Symptomatic/infected: antibiotics (oral or IV); incision and drainage if fluctuant
- Recurrent infection or persistent anomaly: surgical excision (complete urachal excision with bladder dome closure)
- Asymptomatic, incidentally found: excision should be discussed with the family given the risk of malignant transformation in adulthood
PART 2: OMPHALOMESENTERIC (VITELLINE) DUCT REMNANT
Embryology
The omphalomesenteric duct (also called the vitelline duct) is the fetal connection between the midgut and the yolk sac. It passes through the umbilical ring alongside the allantois. Normally, it involutes by weeks 5-9 of gestation (the intestinal attachment is lost by ~6 weeks). Failure of regression - at any point along its course from the ileum to the umbilicus - produces a spectrum of anomalies.
The failure involves a lack of expression of the homeobox gene CDX2, which has been implicated in pathogenesis.
- Schwartz's Principles of Surgery, 11th ed.
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Spectrum of Omphalomesenteric Remnants
The pattern of anomaly depends on where and how much of the duct persists:
| Anomaly | Pathology | Features |
|---|---|---|
| Meckel's diverticulum | Vitelline remnant at the ileal border | Most common; true diverticulum with all bowel layers |
| Omphalomesenteric fistula | Total persistence - both ends remain open | Intestinal contents drain at umbilicus |
| Omphalomesenteric cyst | Partial closure - mid-segment remains cystic | Intra-abdominal or external (umbilical polyp) |
| Fibrous cord | Duct obliterated but a fibrous band persists from ileum to umbilicus | Predisposes to bowel obstruction; volvulus |
| Umbilical sinus | Only the umbilical end remains patent | Umbilical discharge |
Meckel's Diverticulum - "Rule of 2s"
Meckel's diverticulum is the most common congenital anomaly of the GI tract, occurring in ~2% of the population.
The classic Rule of 2s:
- 2% incidence in the population
- 2 feet (60 cm) from the ileocecal valve (on the antimesenteric border)
- 2 inches (~5 cm) in length
- Usually symptomatic by 2 years of age
- 2 types of heterotopic mucosa (gastric - >70% of symptomatic cases; pancreatic - ~5%)
Clinical Complications:
- Hemorrhage - most common presentation in children under 5; painless, massive, lower GI bleeding caused by acid secretion from ectopic gastric mucosa eroding the adjacent ileal mucosa
- Intestinal obstruction - from intussusception, volvulus around a fibrous band, or incarceration in a hernia
- Meckel's diverticulitis - mimics acute appendicitis
- Perforation
Diagnosis:
- 99mTc-pertechnetate (Meckel's) scan - detects ectopic gastric mucosa; sensitivity ~85% in children (lower in adults)
- Ultrasound and CT for complications
- Lateral contrast radiography for persistent vitelline duct remnants
Treatment:
- Symptomatic Meckel's: surgical resection (segmental ileal resection preferred when bleeding, as the bleeding point is typically on the mesenteric side, opposite the diverticulum opening; simple diverticulectomy is acceptable if not bleeding)
- Incidentally found, asymptomatic: generally left alone
- Laparoscopic diverticulectomy is now widely accepted
Histopathology of Omphalomesenteric Duct Remnants
Remnants are characterized by ectopic gastrointestinal mucosa (gastric mucosa being the most common). This must be distinguished from umbilical metastases of gastrointestinal adenocarcinomas (Sister Mary Joseph nodule).
In postmenarcheal females: cutaneous endometriosis at the umbilicus is an important differential for umbilical remnant cysts.
- Dermatology 2-Volume Set, 5th ed.
Comparison: Allantois vs Omphalomesenteric Remnant
| Feature | Allantois Remnant (Urachus) | Omphalomesenteric Remnant |
|---|---|---|
| Structure of origin | Allantois (cloaca diverticulum) | Vitelline/omphalomesenteric duct |
| Normal obliterated structure | Median umbilical ligament | Obliterated vitelline duct |
| Connects | Bladder dome to umbilicus | Ileum to umbilicus |
| Location of main remnant | Midline, prevesical | Antimesenteric border of ileum |
| Most common remnant | Urachal cyst | Meckel's diverticulum |
| Heterotopic tissue | Urothelial/glandular epithelium | Gastric mucosa (most common), pancreatic tissue |
| Key complication | Adenocarcinoma (bladder) | Hemorrhage, obstruction, diverticulitis |
| Key investigation | Ultrasound / CT; VCUG | 99mTc-pertechnetate scan |
| Malignant risk | Yes - urachal adenocarcinoma | Lower; mainly complications from ectopic mucosa |
Here is a clinical image showing omphalomesenteric remnants and Meckel's diverticulum from Sabiston Textbook of Surgery:
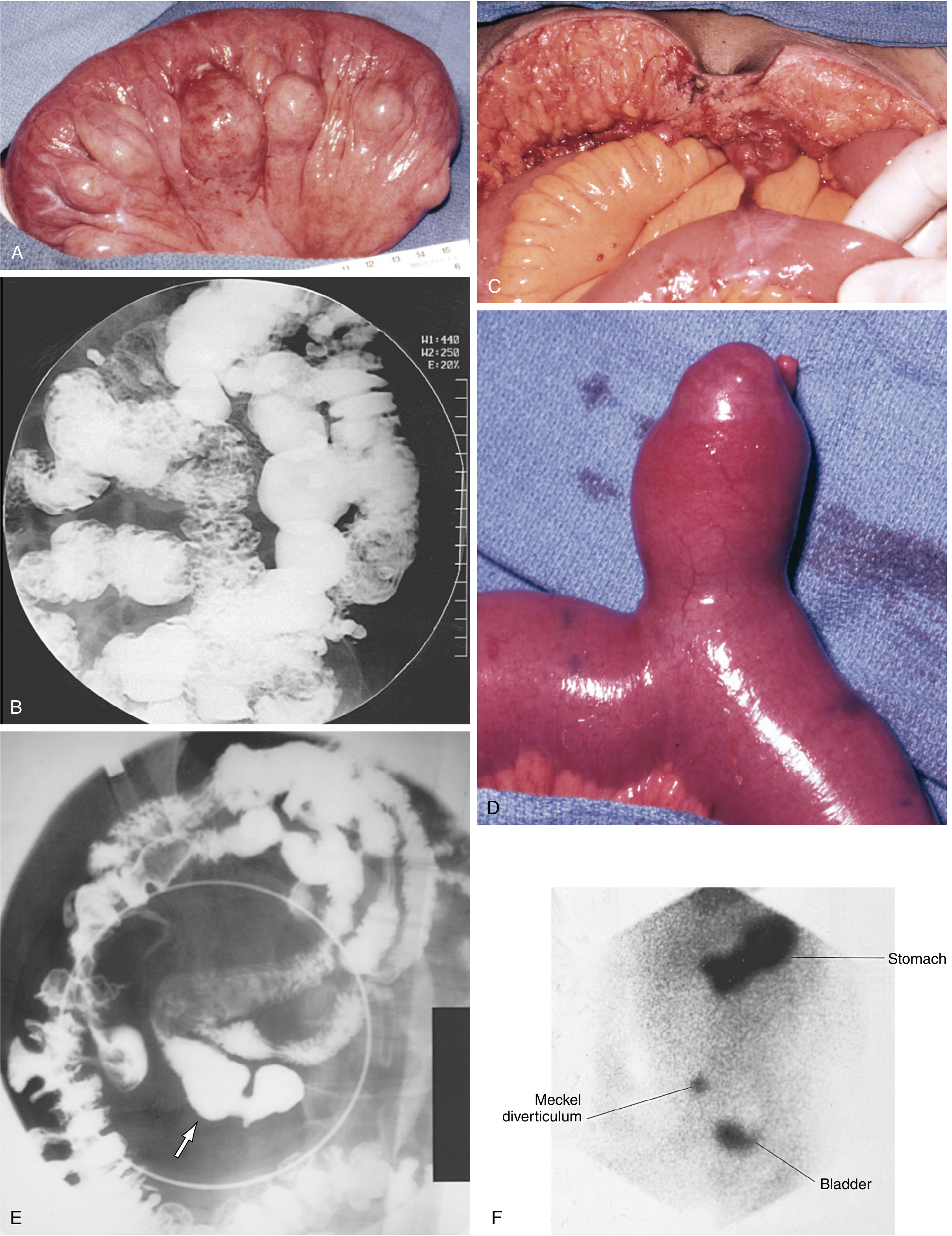
Panel C: Persistent omphalomesenteric remnant as a fibrous cord from ileum to umbilicus. Panel D: Meckel's diverticulum projecting from the antimesenteric border of ileum. Panel F: Tc-99m pertechnetate scintigram showing Meckel's diverticulum distinct from stomach and bladder. (Sabiston Textbook of Surgery)
Key Memory Points:
- Allantois → urachus → median umbilical ligament (if normal); urachal cyst/fistula/sinus if anomalous
- Omphalomesenteric duct → obliterated by week 5-9; Meckel's diverticulum if persists at ileal end
- Meckel's = Rule of 2s; bleeds due to ectopic gastric mucosa; diagnosed with Tc-99 scan
- Urachal anomalies carry risk of adenocarcinoma; omphalomesenteric fistula causes intestinal drainage at umbilicus
This is a shared conversation. Sign in to Orris to start your own chat.