55 yr old male presents with hemoptysis for 1st time. Enumerate the causes of hemoptysis and the approach to the diagnosis management of this patient
causes etiology hemoptysis classification
hemoptysis diagnosis investigation management approach
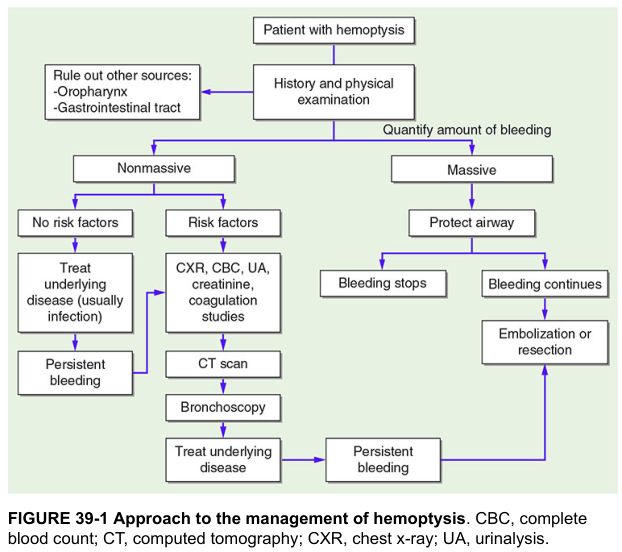
hemoptysis diagnostic algorithm approach
Hemoptysis in a 55-Year-Old Male: Causes, Diagnosis & Management
Definition & Initial Framing
- Pseudohemoptysis: blood from oropharynx, nasopharynx, or sinuses
- Hematemesis: vomiting blood from the GI tract (usually dark, mixed with food, preceded by nausea)
Causes of Hemoptysis
Classified by Frequency / Category
| Category | Specific Causes |
|---|---|
| Infectious (most common overall) | Bronchitis (acute/chronic), Pneumonia, Lung abscess, Tuberculosis (active or old fibrotic), Bronchiectasis, Aspergilloma ("fungus ball"), Necrotizing pneumonia, Parasitic (e.g., paragonimiasis, hydatid) |
| Malignancy | Primary lung carcinoma (squamous cell > others), Bronchial carcinoid tumour, Metastatic tumours to lung |
| Cardiovascular / Vascular | Pulmonary embolism with infarction, Left heart failure / mitral stenosis ("pink frothy sputum"), AV malformations, Aortic aneurysm eroding bronchus, Pulmonary arterial hypertension |
| Airway disease | Chronic bronchitis (most common cause of mild hemoptysis), Bronchiectasis, Tracheobronchial trauma, Foreign body |
| Parenchymal / Diffuse lung disease | Goodpasture's syndrome, Granulomatosis with polyangiitis (Wegener's), Systemic lupus (pulmonary hemorrhage), Idiopathic pulmonary hemosiderosis |
| Coagulopathy / Iatrogenic | Anticoagulant therapy, Thrombocytopenia, DIC, Post-bronchoscopy or biopsy |
| Miscellaneous | Catamenial hemoptysis (endometriosis — not applicable here), Cryptogenic (20–30% after full workup) |
In a 55-year-old male smoker, the top three to prioritize are: Lung carcinoma, TB/post-TB sequelae, and Chronic bronchitis/bronchiectasis.
Approach to Diagnosis
Step 1 — History
| Feature | Significance |
|---|---|
| Quantity | Scant/streaky vs. frank blood vs. massive (>600 mL/24h or >100 mL/h) |
| Duration & onset | Acute vs. chronic/recurrent |
| Smoking history | Pack-years → lung cancer risk |
| Constitutional symptoms | Weight loss, anorexia, night sweats → malignancy or TB |
| Fever, purulent sputum | Infection (bronchitis, pneumonia, abscess) |
| Preceding URI | Acute bronchitis |
| Chronic productive cough | Bronchiectasis |
| TB contact / travel | Endemic area exposure |
| Leg swelling / DVT symptoms | Pulmonary embolism |
| Cardiac history | Mitral stenosis, heart failure |
| Drug history | Anticoagulants, antiplatelets |
| Occupational exposure | Asbestos (mesothelioma), silica |
| Family history | Lung cancer, bleeding disorders |
Step 2 — Physical Examination
| Finding | Suggests |
|---|---|
| Cachexia, lymphadenopathy | Malignancy |
| Clubbing | Lung cancer, bronchiectasis, abscess |
| Localized wheeze / monophonic wheeze | Endobronchial lesion (tumour) |
| Crackles | Pneumonia, bronchiectasis |
| Dullness to percussion | Consolidation, effusion |
| Mitral facies, diastolic murmur | Mitral stenosis |
| DVT signs | PE |
| Oral/nasal lesions | Pseudohemoptysis |
Step 3 — Investigations
Immediate (All Patients)
| Test | Purpose |
|---|---|
| Chest X-ray (CXR) | First-line; may show mass, consolidation, cavitation, hilar enlargement |
| CBC | Anaemia (chronicity), thrombocytopenia |
| Coagulation profile (PT, aPTT, INR) | Coagulopathy |
| Serum creatinine, urinalysis | Pulmonary-renal syndromes (Goodpasture's, Wegener's) |
| Sputum (AFB smear × 3, culture, cytology) | TB, malignancy |
| Pulse oximetry / ABG | Respiratory compromise |
| ECG | Mitral stenosis, right heart strain (PE) |
Second Line (Based on Initial Results)
| Test | Indication |
|---|---|
| CT Chest (HRCT/contrast) | Single most important test — identifies mass, AVM, bronchiectasis, PE (CTPA); mandatory in >40 yr male with hemoptysis |
| Bronchoscopy (flexible) | Localizes bleeding source, allows biopsy of endobronchial lesion, BAL for cytology/culture |
| CT Pulmonary Angiography (CTPA) | Suspected PE |
| Echocardiography | Suspected cardiac cause (mitral stenosis, LV failure) |
| ANCA, anti-GBM antibodies | Suspected vasculitis / Goodpasture's |
| Bronchial arteriography | Preoperative for massive hemoptysis or when embolization is planned |
| PET-CT | Staging of confirmed lung malignancy |
Diagnostic Algorithm
Management
A. Non-Massive Hemoptysis (Majority of Cases)
- Treat the underlying cause (e.g., antibiotics for infection, antitubercular therapy for TB)
- Investigate fully — CT chest is mandatory; bronchoscopy if CT equivocal or mass suspected
- Risk stratify — even "minor" hemoptysis in a 55-year-old male must have malignancy excluded
- Avoid cough suppressants that could cause clot retention
- Follow-up CXR / CT in 6–8 weeks if initial workup inconclusive
B. Massive Hemoptysis (Life-Threatening Emergency)
Massive = >600 mL/24h or any amount causing hemodynamic instability or airway compromise. Death is from asphyxiation, not exsanguination.
| Priority | Action |
|---|---|
| Airway | Position bleeding side DOWN; consider intubation with large-bore ETT (8.0 mm) for airway protection |
| IV Access & Resuscitation | Large-bore IV lines, IV fluids, blood products, type & crossmatch |
| Oxygen | High-flow O₂ |
| ICU admission | Monitoring and escalation |
| Urgent rigid bronchoscopy | Best for visualization + therapeutic intervention (tamponade, laser, electrocautery) |
| Bronchial artery embolization (BAE) | Preferred definitive intervention — effective in >90% of cases acutely |
| Surgical resection | Reserved for BAE failure, AVM, or iatrogenic trauma; requires adequate pulmonary reserve |
| Temporizing measures | Endobronchial blockers, cold saline lavage, topical thrombin via bronchoscope |
Summary for This Patient
| Priority | Action |
|---|---|
| 1 | Quantify bleeding; rule out pseudohemoptysis and hematemesis |
| 2 | Detailed history: smoking, constitutional symptoms, TB exposure, cardiac history |
| 3 | CXR, CBC, coagulation studies, sputum (AFB + cytology), creatinine/UA |
| 4 | CT chest with contrast — mandatory in this age group |
| 5 | Flexible bronchoscopy if CT shows lesion or bleeding source unidentified |
| 6 | If massive: airway protection → ICU → rigid bronchoscopy / bronchial artery embolization |
| 7 | Lung cancer workup must be completed regardless of other positive findings |

Answer all of them
generalized edema etiology history physical examination findings
ascites diagnosis management treatment
effective circulatory volume definition increased decreased states management
| Q | Topic | Key Takeaway |
|---|---|---|
| Q1 | Generalized edema (etiology/H&P) + Ascites (Dx/Mx) | SAAG ≥1.1 = portal HTN; spironolactone + furosemide in 5:2 ratio; albumin with LVP |
| Q2 | Effective Circulatory Volume — ↑/↓ states | ECV is a functional concept; CHF/cirrhosis/nephrotic = ↓ ECV despite excess Na⁺; nephritic/Conn's = ↑ ECV |
| Q3 | Pathogenesis & clinical features of edema + drug causes | 4 Starling mechanisms; CCBs, NSAIDs, TZDs, steroids are the most high-yield drug causes |
| Q4 | Transcellular water + anasarca pathogenesis | 1–2% TBW; disease-specific mechanisms (overflow vs. underfill vs. splanchnic vasodilation) |
| Q5 | ECV %, nephritic vs nephrotic | Nephritic = ↑ ECV (overflow/hypertension); Nephrotic = ↓ ECV (underfill/hypoalbuminemia) — a classic exam comparison |
Algorithm for evaluation of suspected dysphagia
dysphagia evaluation algorithm diagnosis approach
dysphagia algorithm flowchart evaluation
Algorithm for Evaluation of Suspected Dysphagia
Step 1 — Confirm It Is Dysphagia
- Odynophagia — painful swallowing (not difficulty)
- Globus sensation — constant feeling of a lump in the throat, not related to swallowing
- Phagophobia — fear of swallowing (psychiatric)
Step 2 — Localise: Oropharyngeal vs. Esophageal
| Feature | Oropharyngeal | Esophageal |
|---|---|---|
| Symptom onset | Immediately on swallowing (0–1 sec) | 2–10 seconds after initiating swallow |
| Location pointed by patient | Throat / neck | Chest / substernal |
| Associated symptoms | Nasal regurgitation, coughing/choking on swallowing, drooling, dysarthria, aspiration | Regurgitation of undigested food, heartburn, chest pain |
| Neurological symptoms | Often present (dysarthria, diplopia, limb weakness) | Usually absent |
| Solids vs. liquids | Often worse with liquids initially (neuromuscular) | Solids first (mechanical obstruction), or both (motility) |
Step 3 — Diagnostic Algorithm
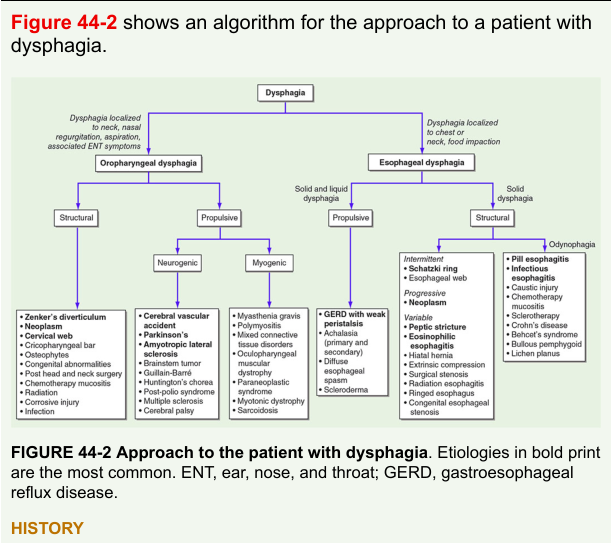
Branch A — Oropharyngeal Dysphagia
Sub-classify: Structural vs. Propulsive (Neuromuscular)
Structural Causes
| Cause | Notes |
|---|---|
| Zenker's diverticulum | Posterior pharyngeal pouch; regurgitation of undigested food, gurgling neck |
| Neoplasm (pharynx / larynx) | Weight loss, hoarseness — must exclude urgently |
| Cervical web (Plummer-Vinson) | Iron deficiency anaemia + dysphagia in females |
| Cricopharyngeal bar | Hypertrophied cricopharyngeus muscle |
| Cervical osteophytes | Elderly, anterior compression |
| Post-surgery / radiation / corrosive injury | History will clarify |
Propulsive (Neurogenic) Causes
| Neurogenic | Myogenic |
|---|---|
| CVA (most common) | Polymyositis / dermatomyositis |
| Parkinson's disease | Myasthenia gravis |
| ALS / motor neuron disease | Muscular dystrophies (oculopharyngeal MD) |
| Brainstem tumour | Myotonic dystrophy |
| Multiple sclerosis | Thyroid myopathy |
| Guillain-Barré syndrome | |
| Huntington's chorea |
Investigations for Oropharyngeal Dysphagia
- Videofluoroscopic swallow study (modified barium swallow) — procedure of choice; evaluates all phases of swallowing in real time
- Fiberoptic endoscopic evaluation of swallowing (FEES) — bedside, no radiation, excellent for aspiration detection
- Otolaryngoscopy — direct visualisation of pharynx and larynx
- Neurological evaluation — MRI brain/brainstem, nerve conduction studies, EMG
- Manometry — rarely needed; used when cricopharyngeal dysfunction suspected
Branch B — Esophageal Dysphagia
Sub-classify by Bolus Type and Pattern
| Pattern | Suggests |
|---|---|
| Solids only | Mechanical / structural obstruction |
| Solids AND liquids from onset | Motility disorder |
| Solids initially → progresses to liquids | Progressive mechanical obstruction (malignancy) |
| Intermittent, solids only, no weight loss | Lower esophageal ring (Schatzki's ring) |
| Progressive, with weight loss | Carcinoma of esophagus |
| Intermittent, solids + liquids, chest pain | Esophageal spasm / motility disorder |
| Solids + liquids + regurgitation + odynophagia | Achalasia |
Structural (Mechanical) Causes
| Cause | Key Feature |
|---|---|
| Carcinoma of esophagus | Progressive, weight loss, >50 yrs, alcohol/smoking |
| Peptic stricture | Longstanding GERD, heartburn history |
| Schatzki's ring | Intermittent dysphagia to solids, "steakhouse syndrome" |
| Eosinophilic esophagitis | Young male, food impaction, atopy |
| Extrinsic compression | Mediastinal lymphoma, lung CA, aortic aneurysm, goitre |
| Foreign body | Acute onset |
Motility (Propulsive) Causes
| Cause | Key Feature |
|---|---|
| Achalasia | Solids + liquids, regurgitation, weight loss, chest pain; "bird's beak" on barium |
| Diffuse esophageal spasm | Intermittent, chest pain, "corkscrew" on barium |
| Hypercontractile ("jackhammer") esophagus | Severe chest pain, high-amplitude contractions on manometry |
| Scleroderma | Raynaud's, skin changes; hypomotility + GERD |
| Ineffective esophageal motility | Associated with GERD; low-amplitude contractions |
Investigations for Esophageal Dysphagia
| Investigation | Role |
|---|---|
| Upper GI endoscopy (OGD) | First-line and most important — visualises mucosa, biopsies structural lesions (cancer, EoE, stricture), allows dilation |
| Barium swallow / esophagram | Functional assessment; shows webs, rings, "bird's beak" (achalasia), "corkscrew" (spasm); complements endoscopy |
| High-resolution esophageal manometry (HRM) | Gold standard for motility disorders — achalasia (types I/II/III), spasm, scleroderma, jackhammer esophagus |
| CT chest / abdomen | Extrinsic compression, staging of esophageal malignancy |
| pH-impedance monitoring | If GERD-related dysphagia suspected |
| Endoscopic ultrasound (EUS) | Staging esophageal carcinoma (T and N staging) |
| PET-CT | Staging malignancy |
Summary Algorithm
DYSPHAGIA
│
├─ Oropharyngeal (transfer dysphagia, neck, immediate, liquids worse)
│ │
│ ├─ Structural → Videofluoroscopic swallow study
│ │ + ENT evaluation + CT neck
│ │
│ └─ Neuromuscular → Neurological workup (MRI brain)
│ + FEES + EMG/NCS
│
└─ Esophageal (substernal, 2–10 sec after swallow)
│
├─ Solids ONLY → Mechanical obstruction
│ ├─ Progressive + weight loss → OGD + CT (rule out cancer)
│ ├─ Intermittent, no weight loss → Barium (ring/web) + OGD
│ └─ Young + atopy + food impaction → OGD + biopsy (EoE)
│
└─ Solids + Liquids → Motility disorder
├─ Regurgitation + weight loss → Barium + HRM (achalasia)
├─ Chest pain + intermittent → HRM (spasm/jackhammer)
└─ Raynaud's + GERD → HRM (scleroderma)
Key Clinical Pearls
- Upper endoscopy is the single most useful test for esophageal dysphagia (Harrison's, p. 1209)
- Videofluoroscopy is the procedure of choice for oropharyngeal dysphagia
- Manometry is reserved for when endoscopy and barium are normal (motility disorders)
- Any progressive dysphagia with weight loss in a patient >50 years = malignancy until proven otherwise
- Dysphagia to both solids and liquids from the start always indicates a motility disorder, never a structural one
Summarise Harrison's chapter 46 diarrhoea, point wise clear cut
diarrhea definition classification acute chronic pathophysiology Harrison chapter 46
diarrhea etiology causes infectious inflammatory osmotic secretory
acute diarrhea evaluation treatment management approach
chronic diarrhea diagnosis workup investigations causes malabsorption
Harrison's Chapter 46 — Diarrhoea: Point-wise Summary
1. DEFINITIONS
- Diarrhoea: Passage of abnormally liquid or unformed stools at increased frequency; stool weight >200 g/day in adults on a Western diet
- Acute diarrhoea: < 2 weeks
- Persistent diarrhoea: 2–4 weeks
- Chronic diarrhoea: > 4 weeks
Distinguish from:
- Pseudodiarrhoea: Frequent passage of small volumes (<200 g/day) of stool — seen in IBS, proctitis, rectal neoplasm; urgency with tenesmus
- Faecal incontinence: Involuntary passage of rectal contents — neurological or sphincter pathology; not true diarrhoea
2. ACUTE DIARRHOEA
A. Aetiology
Infectious (Most Common)
| Route | Organisms |
|---|---|
| Viral | Norovirus (most common worldwide), Rotavirus (children), Astrovirus, Adenovirus |
| Bacterial toxin (preformed) | S. aureus, B. cereus (emetic) — rapid onset within 6 hrs, vomiting-predominant |
| Bacterial toxin (enterotoxin) | E. coli (ETEC), V. cholerae, C. perfringens — watery, profuse; no mucosal invasion |
| Bacterial invasive | Salmonella, Shigella, Campylobacter, EIEC, Yersinia, C. difficile — dysentery, fever, bloody stools |
| Parasitic | Giardia, Cryptosporidium, E. histolytica — subacute, travel-related |
Non-Infectious
- Drugs: antibiotics, laxatives, antacids (Mg-containing), colchicine, NSAIDs, metformin, digoxin
- Food allergy / intolerance
- Ischaemic colitis
- Diverticulitis
- First presentation of IBD
B. Evaluation of Acute Diarrhoea
Step 1 — Identify patients needing investigation (most resolve spontaneously):
- Profuse watery diarrhoea with signs of dehydration
- Passage of many small-volume bloody stools
- Temperature >38.5°C
- Duration >48 hours without improvement
- Severe abdominal pain
- Elderly (>70 years) or immunocompromised
- Recent antibiotic use (C. difficile)
- Hospital-acquired or nosocomial diarrhoea
- Recent travel to endemic area
Step 2 — Investigations
- Stool routine & microscopy: WBCs (invasive), RBCs, ova, cysts, parasites
- Stool culture & sensitivity
- C. difficile toxin (A + B PCR or EIA) if antibiotic-associated
- Stool for rotavirus / norovirus antigen (in outbreak settings)
- CBC: leucocytosis (bacterial), eosinophilia (parasitic)
- Electrolytes, renal function: dehydration assessment
- Sigmoidoscopy/colonoscopy: if bloody diarrhoea persists or C. difficile suspected but toxin negative
C. Management of Acute Diarrhoea
1. Rehydration (Most Important)
- Mild–moderate: Oral Rehydration Solution (ORS) — WHO formula: Na 75, K 20, Cl 65, citrate 10, glucose 75 mmol/L
- Severe / unable to tolerate orally: IV fluids (Ringer's Lactate or Normal Saline)
- Avoid fruit juices, sodas (hyperosmolar, worsen diarrhoea)
2. Diet
- Early refeeding encouraged — BRAT diet (Bananas, Rice, Applesauce, Toast) or any easily digestible food
- Avoid lactose-containing foods temporarily
3. Symptomatic Agents
- Loperamide: First-line antimotility agent; reduces frequency; avoid in bloody diarrhoea or suspected invasive infection (risk of toxic megacolon)
- Bismuth subsalicylate: Mild antisecretory + antimicrobial effect
- Racecadotril: Enkephalinase inhibitor; antisecretory; safer than loperamide in children
4. Antibiotics
- NOT routinely indicated — most acute diarrhoea is viral and self-limiting
- Indicated when:
| Indication | Drug |
|---|---|
| Traveller's diarrhoea (moderate–severe) | Azithromycin (preferred), Ciprofloxacin, Rifaximin |
| Shigella / invasive bacterial diarrhoea | Azithromycin or Ciprofloxacin |
| C. difficile | Vancomycin (oral) or Fidaxomicin (first-line); Metronidazole (mild cases only) |
| Cholera | Doxycycline (single dose) |
| Giardia | Metronidazole or Tinidazole |
| E. histolytica | Metronidazole + Diloxanide furoate |
| Immunocompromised patients | Lower threshold for antibiotics |
- Avoid antibiotics in EHEC (E. coli O157:H7) — increases risk of HUS
3. CHRONIC DIARRHOEA (>4 WEEKS)
A. Pathophysiological Classification
1. Secretory Diarrhoea
- Mechanism: Active ion secretion or inhibition of ion absorption by enterotoxins, hormones, or laxatives → net intestinal fluid secretion
- Hallmarks:
- Large volume (>1 L/day), watery
- Persists with fasting (does NOT stop with fasting)
- Osmotic gap <50 mOsm/kg (stool osmolality ≈ 2 × [Na + K])
- Causes:
- Microscopic colitis (collagenous / lymphocytic colitis)
- Bile acid malabsorption (post-cholecystectomy, ileal disease)
- Peptide-secreting tumours: VIPoma (WDHA syndrome), Zollinger-Ellison, Carcinoid, Gastrinoma, Medullary thyroid carcinoma
- Congenital chloride diarrhoea
- Chronic laxative abuse (stimulant laxatives — senna, bisacodyl)
- Addison's disease
2. Osmotic Diarrhoea
- Mechanism: Poorly absorbable solutes retain water in lumen → exceed colonic reabsorptive capacity
- Hallmarks:
- Stops with fasting or when causative agent stopped
- Osmotic gap >125 mOsm/kg
- Stool pH <6 (carbohydrate fermentation)
- Causes:
- Lactase deficiency (lactose intolerance)
- Sorbitol, mannitol ingestion (sugar-free gum, diabetic foods)
- Lactulose, Mg-containing antacids
- Malabsorption syndromes (coeliac disease, SIBO, pancreatic exocrine insufficiency)
- Osmotic laxative abuse (Mg sulphate, lactulose)
3. Inflammatory / Exudative Diarrhoea
- Mechanism: Mucosal inflammation, ulceration, exudation of blood, pus, proteins
- Hallmarks:
- Bloody or mucoid stools
- Fever, systemic symptoms
- Faecal lactoferrin/calprotectin elevated
- Causes:
- IBD: Crohn's disease, Ulcerative colitis
- Infectious colitis: CMV, C. difficile, E. histolytica, Shigella, TB
- Ischaemic colitis
- Radiation enterocolitis
- Colonic neoplasm
- Diverticular disease
4. Malabsorptive Diarrhoea (Fat / Carbohydrate Malabsorption)
- Mechanism: Defective mucosal digestion or absorption → osmotic effect + fatty acid irritation of colon
- Hallmarks:
- Steatorrhoea — pale, bulky, greasy, offensive, floating stools
- Weight loss, nutritional deficiencies (fat-soluble vitamins A, D, E, K)
- Sudan stain: fat globules in stool
- Causes:
- Mucosal: Coeliac disease, tropical sprue, Whipple's disease, giardiasis, short bowel syndrome, intestinal lymphoma
- Pancreatic: Chronic pancreatitis, cystic fibrosis, pancreatic cancer
- Luminal: Bile acid deficiency (cholestatic liver disease, ileal resection), SIBO
5. Motility-Related Diarrhoea
- Mechanism: Rapid intestinal transit → reduced contact time for absorption
- Causes:
- IBS-D (Irritable Bowel Syndrome — diarrhoea predominant)
- Post-vagotomy, post-gastrectomy (dumping syndrome)
- Hyperthyroidism
- Diabetic autonomic neuropathy
- Systemic sclerosis (scleroderma)
B. Evaluation of Chronic Diarrhoea
Step 1 — History
| Feature | Significance |
|---|---|
| Stool characteristics (volume, consistency, blood, mucus, fat) | Classify type |
| Onset, duration, pattern (continuous vs. intermittent) | Inflammatory vs. functional |
| Nocturnal diarrhoea | Organic disease (wakes patient from sleep) — IBS does NOT cause nocturnal diarrhoea |
| Relationship to fasting | Osmotic (stops) vs. secretory (continues) |
| Weight loss, fever, rectal bleeding | Organic / serious pathology |
| Dietary history (lactose, sorbitol, gluten) | Osmotic / intolerance |
| Drug history | Drug-induced |
| Travel, sexual history | Infectious, HIV-related |
| Family history | IBD, coeliac, colorectal cancer |
| Surgery history | Post-surgical diarrhoea |
| Systemic symptoms | Thyroid, diabetes, autoimmune |
Step 2 — Physical Examination
- Assess hydration, nutritional status, weight
- Abdominal mass, tenderness, distension
- Perianal disease (fistula, skin tags) → Crohn's
- Dermatitis herpetiformis → coeliac
- Skin pigmentation → Addison's / Whipple's
- Flushing → carcinoid
- Thyroid enlargement → hyperthyroidism
- Peripheral neuropathy / postural hypotension → diabetic autonomic neuropathy
Step 3 — Initial Investigations (All Patients)
| Test | Purpose |
|---|---|
| CBC with differential | Anaemia, eosinophilia, leucocytosis |
| ESR, CRP | Inflammation |
| LFTs, serum albumin | Nutritional status, liver disease |
| Serum electrolytes, creatinine | Dehydration |
| Thyroid function (TSH) | Hyperthyroidism |
| Stool routine, culture, ova & parasites | Infectious cause |
| Faecal calprotectin | Differentiates IBD (elevated) from IBS (normal) |
| Faecal occult blood | Mucosal disease, neoplasm |
| Stool fat (72-hr collection or Sudan stain) | Steatorrhoea |
Step 4 — Second-Line Investigations (Directed)
| Suspected Diagnosis | Investigation |
|---|---|
| Coeliac disease | Anti-tTG IgA + total IgA; confirmed by duodenal biopsy |
| IBD | Colonoscopy + ileoscopy + biopsy; MRI enterography (Crohn's) |
| Microscopic colitis | Colonoscopy (normal macroscopically) + mucosal biopsy (diagnostic) |
| Malabsorption / SIBO | Hydrogen breath test; D-xylose absorption test |
| Pancreatic insufficiency | Faecal elastase-1 (low); CT pancreas |
| Bile acid malabsorption | SeHCAT scan; empirical cholestyramine trial |
| Secretory tumour (VIPoma, carcinoid, gastrinoma) | Serum VIP, gastrin, 5-HIAA (urine), chromogranin A; CT/MRI abdomen; octreotide scan |
| Microscopic / functional | Colonoscopy + biopsy; pH-impedance; Rome IV criteria for IBS |
| Immunodeficiency | HIV test, serum immunoglobulins |
C. Management of Chronic Diarrhoea
General
- Always treat the underlying cause — symptomatic treatment alone is insufficient
- Correct nutritional deficiencies (iron, B12, folate, vitamins A/D/E/K, zinc)
- Monitor weight and hydration
Disease-Specific
| Condition | Treatment |
|---|---|
| Coeliac disease | Strict gluten-free diet (lifelong) |
| IBD — UC | 5-ASA, steroids, azathioprine, biologics (infliximab, vedolizumab) |
| IBD — Crohn's | Steroids, azathioprine, methotrexate, anti-TNF agents; surgery if indicated |
| Microscopic colitis | Budesonide (first-line); stop NSAIDs/PPIs/SSRIs |
| Lactose intolerance | Lactose-free diet; lactase enzyme supplements |
| Pancreatic insufficiency | Pancreatic enzyme replacement therapy (PERT) with meals |
| SIBO | Rifaximin (non-absorbable antibiotic); treat underlying cause |
| Bile acid malabsorption | Cholestyramine (bile acid sequestrant) |
| VIPoma / carcinoid | Octreotide (somatostatin analogue); tumour resection |
| Hyperthyroidism | Antithyroid drugs / radioiodine |
| IBS-D | Low-FODMAP diet; antispasmodics; loperamide; low-dose TCA; rifaximin (non-constipating antibiotic); eluxadoline |
| Microscopic colitis | Bismuth subsalicylate; budesonide |
Symptomatic / Antidiarrhoeal Agents
| Drug | Mechanism | Use |
|---|---|---|
| Loperamide | μ-opioid receptor agonist → ↓ motility, ↑ sphincter tone | IBS-D, functional diarrhoea |
| Cholestyramine | Bile acid sequestrant | Bile acid malabsorption, post-ileal resection |
| Octreotide | Somatostatin analogue → ↓ secretion | VIPoma, carcinoid, chemotherapy diarrhoea |
| Bismuth subsalicylate | Antisecretory + antimicrobial | Traveller's diarrhoea, microscopic colitis |
| Codeine phosphate | Opioid → ↓ motility | Refractory diarrhoea (short-term) |
| Clonidine | α₂-agonist → ↑ ion absorption | Diabetic autonomic diarrhoea |
4. SPECIAL SITUATIONS
Traveller's Diarrhoea
- Most common in travel to Asia, Africa, Latin America
- Commonest cause: ETEC; also Campylobacter, Shigella, Salmonella, norovirus
- Self-limiting (3–5 days)
- Treatment: ORS + Loperamide + Azithromycin (if severe); Rifaximin for non-invasive (watery) traveller's diarrhoea
Diarrhoea in Immunocompromised / HIV
- Organisms not typically seen in immunocompetent hosts:
- CD4 <200: Cryptosporidium, Microsporidium, Isospora (Cystoisospora) belli, MAC (Mycobacterium avium complex), CMV colitis
- CD4 <50: Disseminated MAC, CMV enteritis
- Treatment: Antiretroviral therapy to restore immunity + organism-specific therapy
C. difficile Colitis
- Risk: Recent antibiotics (clindamycin, fluoroquinolones, cephalosporins, broad-spectrum PCN), hospitalisation, age >65, PPI use
- Diagnosis: Stool PCR for C. difficile toxin genes (most sensitive) or GDH + toxin EIA
- Treatment:
- Mild–moderate: Oral Vancomycin 125 mg QID × 10 days or Fidaxomicin 200 mg BD × 10 days (lower recurrence rate)
- Severe (WBC >15,000, Cr >1.5×baseline): Vancomycin (oral) + IV Metronidazole
- Fulminant (ileus, megacolon, hypotension): Vancomycin (oral + per-rectal) + IV Metronidazole; surgical colectomy if refractory
- Recurrent: Fidaxomicin > Vancomycin; Faecal microbiota transplant (FMT) for ≥3rd recurrence
5. KEY DIFFERENTIATING POINTS AT A GLANCE
| Feature | Osmotic | Secretory | Inflammatory | Malabsorptive |
|---|---|---|---|---|
| Volume | Moderate | Large (>1 L/day) | Moderate | Moderate–large |
| Blood/pus | No | No | Yes | No |
| Fasting effect | Stops | Continues | Continues | Stops |
| Osmotic gap | >125 mOsm | <50 mOsm | Variable | >125 mOsm |
| Stool fat | Normal | Normal | Normal | Elevated |
| Key feature | pH <6, stops with fasting | Nocturnal, large volume | Fever, blood, CRP↑ | Steatorrhoea, weight loss |
6. ALARM FEATURES (ALWAYS INVESTIGATE)
- Rectal bleeding
- Nocturnal diarrhoea
- Weight loss >5 kg
- Fever
- Age >50 with new-onset change in bowel habit
- Family history of colorectal cancer or IBD
- Palpable abdominal or rectal mass
- Elevated CRP / calprotectin
- Anaemia or hypoalbuminaemia
Harrison's ch 47 unintentional weight loss summary with flowcharts and tables
unintentional weight loss definition etiology causes evaluation Harrison chapter 47
unintentional weight loss algorithm flowchart evaluation
unintentional weight loss malignancy psychiatric social causes diagnosis investigation management
weight loss causes categories organic non-organic table
weight loss history physical examination laboratory tests approach workup
unintentional weight loss diagnostic approach evaluation figure
Harrison's Chapter 47: Unintentional Weight Loss (UWL)
Clear summary with flowcharts and tables
1) Definition and clinical significance
- Unintentional weight loss (UWL) = involuntary loss of weight, often insidious
- Clinically significant when:
- >4.5 kg (10 lb) or
- >5% body weight in 6 to 12 months
- Common in OPD and especially older adults
- Up to 25% may remain without a clear diagnosis after evaluation
- A substantial fraction has serious underlying disease (including malignancy)
2) Major etiologic categories (high-yield)
| Category | Typical conditions |
|---|---|
| 1. Malignancy | GI, lung, pancreas, lymphoma, hematologic cancers |
| 2. Chronic inflammatory/infectious | TB, HIV, chronic infections, rheumatologic/inflammatory disease |
| 3. Metabolic/endocrine | Hyperthyroidism, diabetes mellitus, adrenal disease |
| 4. Psychiatric | Depression, dementia, anxiety, eating disorders, substance use |
- Medications (anorexia, nausea, dysgeusia)
- Social causes (poverty, isolation, inability to cook/feed)
- Dental/oral issues, dysphagia, malabsorption, chronic organ failure (cardiac/renal/hepatic/pulmonary)
3) Pathophysiologic framework
| Mechanism | Clues |
|---|---|
| Reduced intake | Anorexia, depression, dysphagia, oral pain, social neglect |
| Malabsorption | Diarrhea, steatorrhea, micronutrient deficiency |
| Increased metabolic demand | Fever, hyperthyroidism, malignancy, chronic infection |
| Excess nutrient loss | Uncontrolled DM (glycosuria), protein-losing enteropathy, nephrotic protein loss |
| Cachexia pathway | Cytokine-driven catabolism (TNF, IL-1, IL-6), muscle wasting despite intake |
4) Red flags ("alarm features")
| Red flag | Why important |
|---|---|
| Age >50 with new UWL | Higher probability of malignancy |
| Smoking history | Raises occult cancer risk |
| Fever/night sweats | TB, lymphoma, chronic infection |
| Persistent pain or organ-specific symptoms | Localizing clue for organic disease |
| GI bleeding/change in bowel habit | GI malignancy/inflammatory disease |
| Lymphadenopathy/hepatosplenomegaly | Hematologic or systemic disease |
| Abnormal baseline labs | Increases likelihood of serious organic cause |
5) History: focused diagnostic questions
| Domain | What to ask |
|---|---|
| Weight trajectory | Amount, duration, measured vs perceived, appetite |
| Dietary intake | Quantity/quality, chewing/swallowing issues |
| GI symptoms | Dysphagia, nausea, vomiting, diarrhea, steatorrhea, pain, blood loss |
| Constitutional symptoms | Fever, night sweats, fatigue |
| Endocrine symptoms | Heat intolerance, palpitations, polyuria/polydipsia |
| Respiratory symptoms | Cough, hemoptysis, dyspnea |
| Psychiatric/cognitive | Mood, anhedonia, memory, behavior change |
| Medication/substance | New drugs, alcohol, tobacco, stimulants |
| Social factors | Isolation, food insecurity, functional dependence |
6) Physical examination checklist
- Vitals, BMI, temporal muscle wasting, sarcopenia
- Oral cavity and dentition
- Thyroid, lymph nodes
- Chest exam
- Abdominal mass/organomegaly
- Rectal exam (if indicated)
- Neurologic and cognitive screen
- Mood assessment
7) Baseline investigations (first-line panel)
| Test | Utility |
|---|---|
| CBC | anemia, infection, hematologic disease |
| ESR/CRP | inflammatory burden |
| CMP (LFT, RFT, electrolytes) | organ dysfunction |
| Glucose/HbA1c | diabetes |
| TSH | hyperthyroidism/hypothyroidism |
| Urinalysis | renal/systemic clues |
| Chest X-ray | occult pulmonary disease/cancer/TB |
| HIV/TB testing (risk-based) | chronic infection screen |
| Stool occult blood (as indicated) | GI blood loss |
- CT chest/abdomen/pelvis
- Endoscopy/colonoscopy
- Malabsorption workup
- Autoimmune panel
- Bone marrow or biopsy (if hematologic concern)
8) Evaluation algorithm (flowchart)
Patient with suspected UWL
|
v
Confirm true loss?
(>5% body weight in 6-12 months; serial measured weights)
|
+--> No -> Reassure, nutrition counseling, follow-up weight checks
|
v
Detailed history + exam
(localizing symptoms? psychiatric/social factors? medications?)
|
v
Baseline investigations
(CBC, ESR/CRP, CMP, TSH, glucose, UA, CXR ± age/risk-appropriate screening)
|
+--> Abnormal/localizing findings present
| |
| v
| Targeted diagnostics
| (CT/endoscopy/biopsy/infection/endocrine/rheumatology workup)
| |
| v
| Treat specific cause
|
+--> No clear cause after initial workup
|
v
Reassess for:
- Depression/dementia/substance use
- Medication adverse effects
- Social and functional barriers
- Occult malignancy risk
|
v
Nutritional intervention + close follow-up (1-3 months)
|
+--> Ongoing loss / new red flags -> expanded imaging and specialist referral
+--> Stabilization/improvement -> continue supportive management
9) Differential diagnosis table by pattern
| Clinical pattern | Likely etiologies |
|---|---|
| Good appetite + weight loss | Hyperthyroidism, uncontrolled diabetes, malabsorption |
| Poor appetite + low mood | Depression, malignancy, chronic inflammatory disease |
| Fever/night sweats + weight loss | TB, lymphoma, chronic infection, endocarditis |
| Chronic cough + smoking + weight loss | Lung malignancy, TB, COPD-related cachexia |
| Diarrhea/steatorrhea | Malabsorption, pancreatic insufficiency, celiac disease |
| Early satiety + abdominal fullness | Gastric/pancreatic/hepatosplenic pathology |
| Elderly, isolated, frail | Multifactorial: social + depression + dental + medication |
10) Management principles
A. Treat the cause
- Malignancy, endocrine disease, infection, inflammatory disease, GI disorder, etc.
B. Nutritional rehabilitation
- Calorie and protein targets individualized
- Small frequent meals, oral nutrition supplements
- Micronutrient correction
- Dietitian involvement early
C. Address reversible contributors
- Deprescribe anorexigenic drugs when possible
- Treat pain, nausea, constipation, dysphagia
- Dental care, swallowing therapy if needed
- Treat depression/substance use
- Social support and meal access
D. Monitoring
- Serial weight (same scale/time), functional status, muscle mass trend
- Watch for frailty, falls, recurrent hospitalization
11) Elderly-specific notes (very high yield)
- Causes are often multifactorial, not single-diagnosis
- Common hidden drivers: depression, cognitive decline, polypharmacy, social isolation, poor dentition
- UWL in older adults predicts morbidity, mortality, and functional decline
- Early multidisciplinary care improves outcomes
12) Exam-ready ultra-short summary
| Ask in exam | One-line answer |
|---|---|
| Definition | >5% body weight (or >4.5 kg) in 6-12 months, involuntary |
| Main categories | Malignancy, chronic inflammatory/infectious, metabolic/endocrine, psychiatric |
| First workup | Focused history/exam + CBC, ESR/CRP, CMP, TSH, glucose, UA, CXR |
| Most important principle | Confirm true loss, search for localizing clues, then targeted tests |
| If no cause found initially | Reassess psychosocial/medications, provide nutrition support, close follow-up, re-investigate if persistent |
Approach to a patient with fever and jaundice. Harrisons chapter 49 based
fever jaundice approach evaluation causes Harrison chapter 49
fever jaundice diagnostic algorithm flowchart
jaundice classification prehepatic hepatic posthepatic bilirubin metabolism
jaundice history physical examination laboratory investigation approach diagnosis
Approach to a Patient with Fever and Jaundice
Based on Harrison's Principles of Internal Medicine, 21st Ed. — Chapter 49
1. DEFINITIONS
- Jaundice (Icterus): Yellow discolouration of skin, sclerae, and mucous membranes due to elevated serum bilirubin
- Clinically visible when serum bilirubin >2.5–3 mg/dL
- Normal serum bilirubin: 0.3–1.2 mg/dL
- Fever + Jaundice: A clinically important combination — always suggests a serious underlying condition (infection, sepsis, liver disease, haemolytic disorder)
2. BILIRUBIN METABOLISM (Physiology Basis)
RBCs destroyed (85%) + ineffective erythropoiesis (15%)
|
v
Haem → Biliverdin → UNCONJUGATED bilirubin
(indirect, lipid-soluble, albumin-bound, NOT excreted in urine)
|
v
Liver uptake (OATP1B1/3 transporters)
|
v
UGT1A1 enzyme → CONJUGATED bilirubin
(direct, water-soluble, excreted in bile)
|
v
Bile → Intestine → Urobilinogen → Stercobilin (stool colour)
↓
Reabsorbed → Urobilin (in urine)
3. CLASSIFICATION OF JAUNDICE
| Type | Mechanism | Bilirubin Fraction | Examples |
|---|---|---|---|
| Pre-hepatic | Excess bilirubin production (haemolysis) overwhelms hepatic uptake | Unconjugated (Indirect) ↑ | Haemolytic anaemia, G6PD deficiency, sickle cell, malaria, transfusion reactions |
| Hepatic (Hepatocellular) | Defective uptake, conjugation, or excretion within liver cells | Mixed (both ↑) | Viral hepatitis, alcoholic hepatitis, drug-induced liver injury, cirrhosis, autoimmune hepatitis, leptospirosis |
| Post-hepatic (Cholestatic/Obstructive) | Obstruction of biliary outflow — intrahepatic or extrahepatic | Conjugated (Direct) ↑ | Choledocholithiasis, cholangitis, pancreatic cancer, PSC, PBC, biliary stricture |
4. CAUSES OF FEVER WITH JAUNDICE
A. Infectious Causes (Leading Cause in Developing Countries)
| Category | Diseases |
|---|---|
| Viral hepatitis | Hepatitis A, B, C, D, E; EBV; CMV; HSV hepatitis |
| Parasitic | Malaria (most important worldwide), Babesiosis |
| Bacterial | Leptospirosis (Weil's disease), Typhoid fever, Cholangitis (ascending), Liver abscess, Brucellosis, Q fever, Syphilis |
| Mycobacterial | TB (hepatic), M. avium complex (HIV) |
| Fungal | Hepatosplenic candidiasis, Histoplasmosis, Cryptococcosis |
| Helminthic | Schistosomiasis, Fascioliasis, Clonorchiasis, Echinococcosis, Ascariasis |
| Rickettsial/Other | Ehrlichiosis, Yellow fever, Dengue, Viral haemorrhagic fevers (Ebola) |
| Sepsis | Cholestasis of sepsis — bacteria anywhere in body cause intrahepatic cholestasis |
B. Non-Infectious Causes
| Category | Examples |
|---|---|
| Biliary obstruction + superinfection | Choledocholithiasis + ascending cholangitis (Charcot's triad) |
| Drug-induced liver injury (DILI) | Paracetamol overdose, ATT drugs (INH, rifampicin, PZA), statins, antibiotics |
| Alcoholic hepatitis | Fever, jaundice, tender hepatomegaly in heavy drinkers |
| Autoimmune hepatitis | Fever in flare |
| Haematological | Haemolytic crisis (sickle cell, G6PD, thalassaemia, TTP/HUS) |
| Malignancy | Hepatocellular carcinoma (HCC) with necrosis, lymphoma with liver involvement |
| Wilson's disease | Acute liver failure + haemolytic anaemia + fever |
5. HISTORY: KEY POINTS TO ELICIT
| Domain | Questions | Clue |
|---|---|---|
| Onset | Acute vs. gradual | Acute = viral/haemolytic; Gradual = chronic liver disease, malignancy |
| Fever pattern | Intermittent spike, quotidian, hectic | Quotidian (daily) spikes → malaria/abscess |
| Colour of urine | Dark (cola-coloured) | Conjugated hyperbilirubinuria |
| Colour of stool | Pale/clay-coloured | Obstructive jaundice (absence of stercobilin) |
| RUQ/abdominal pain | Colicky vs. constant | Biliary colic vs. hepatic stretch |
| Pruritus | Present | Obstructive/cholestatic jaundice (bile salts in skin) |
| Travel history | Endemic areas | Malaria, viral hepatitis A/E, typhoid, leptospirosis |
| Occupational/contact | Farmers, abattoir, rodent exposure | Leptospirosis, Q fever, brucellosis |
| Sexual history/IV drug use | Risky behaviour | Hepatitis B, C, HIV |
| Alcohol | Units/day, duration | Alcoholic hepatitis, cirrhosis |
| Drug history | Prescription, OTC, herbal | DILI (paracetamol, ATT, statins, herbal) |
| Blood transfusion | Previous | Haemolytic, hepatitis B/C |
| Family history | Haemolytic disorders | G6PD, thalassaemia, sickle cell, hereditary spherocytosis |
6. PHYSICAL EXAMINATION: SYSTEMATIC APPROACH
| System | Finding | Significance |
|---|---|---|
| General | Pallor | Haemolysis |
| Cachexia | Malignancy, chronic liver disease | |
| Tattoos, IV track marks | Hepatitis B/C | |
| Skin | Scratch marks | Pruritus → obstructive jaundice |
| Jaundice depth | Mild (haemolysis/hepatitis) vs. deep greenish (prolonged obstruction) | |
| Rash, petechiae, conjunctival haemorrhage | Dengue, leptospirosis, viral haemorrhagic fever | |
| Spider naevi, palmar erythema, leukonychia, caput medusae | Chronic liver disease/cirrhosis | |
| Eyes | Scleral icterus | Earliest visible sign of jaundice |
| Kayser-Fleischer rings | Wilson's disease | |
| Abdomen | Tender hepatomegaly | Hepatitis, hepatic abscess, leptospirosis, malaria |
| Non-tender hepatomegaly | Biliary obstruction, malignancy | |
| Splenomegaly | Malaria, haemolysis, portal hypertension, lymphoma | |
| Palpable gallbladder (Courvoisier's sign) | Painless jaundice → pancreatic/periampullary carcinoma | |
| Ascites | Portal hypertension, malignancy | |
| RUQ tenderness + Murphy's sign | Acute cholecystitis | |
| Other | Lymphadenopathy | Lymphoma, infectious mononucleosis, TB |
| Splenomegaly + anaemia | Haemolytic disorders, malaria | |
| Rigors/chills with fever spikes | Malaria, ascending cholangitis, liver abscess | |
| CNS features (encephalopathy, flap) | Acute liver failure |
7. KEY CLINICAL SYNDROMES TO RECOGNISE
| Syndrome | Features | Diagnosis |
|---|---|---|
| Weil's disease (Leptospirosis) | Fever + jaundice + AKI + conjunctival suffusion + myalgia + thrombocytopenia | Serology (MAT), PCR |
| Ascending cholangitis | Charcot's triad: Fever + RUQ pain + Jaundice; Reynolds' pentad adds shock + altered sensorium | ERCP + antibiotics |
| Falciparum malaria | Fever (quotidian) + jaundice + anaemia + thrombocytopenia + splenomegaly + cerebral malaria | Peripheral smear, RDT, PCR |
| Acute viral hepatitis A/E | Acute onset, fever (resolves as jaundice develops), tender hepatomegaly, dark urine, travel/food exposure | Anti-HAV IgM, Anti-HEV IgM |
| Alcoholic hepatitis | Heavy alcohol use + fever + tender hepatomegaly + jaundice + AST:ALT >2:1 + high bilirubin | Maddrey's discriminant function |
| Dengue with hepatitis | Fever + rash + myalgia + thrombocytopenia + raised ALT/AST ± jaundice | NS1 antigen, dengue IgM |
| Haemolytic crisis | Fever (from crisis) + jaundice + severe anaemia + splenomegaly; urine urobilinogen ↑, no bilirubinuria | Peripheral smear, Coombs, G6PD assay |
| Liver abscess (amoebic/pyogenic) | High fever + RUQ pain + hepatomegaly + raised diaphragm on CXR | USG/CT, serology |
| Acute liver failure | Jaundice + coagulopathy + encephalopathy within 26 weeks | INR, EEG, transplant assessment |
8. INVESTIGATIONS: STEPWISE APPROACH
Step 1 — Initial Laboratory Panel
| Test | What it tells you |
|---|---|
| Total and direct bilirubin (fractionation) | Conjugated (direct) vs. unconjugated (indirect) — determines type |
| AST, ALT | Hepatocellular damage (viral, alcoholic, drug-induced) |
| ALP, GGT | Cholestatic/obstructive pattern |
| PT/INR | Hepatic synthetic function |
| Serum albumin | Chronic hepatic insufficiency |
| CBC | Anaemia (haemolytic), thrombocytopenia (malaria, dengue, DIC), leucocytosis (bacterial) |
| Peripheral blood smear | Haemolysis morphology, malaria parasites |
| Urine bilirubin + urobilinogen | Bilirubinuria = conjugated ↑; Urobilinogen ↑ = haemolysis/hepatocellular |
| Renal function, electrolytes | Leptospirosis, acute liver failure |
| Reticulocyte count | Haemolysis |
| LDH, haptoglobin | Haemolysis |
| Blood cultures | Bacterial sepsis, cholangitis |
Step 2 — Pattern Interpretation (LFT Pattern)
| Pattern | AST/ALT | ALP/GGT | Bilirubin | Think of |
|---|---|---|---|---|
| Hepatocellular | Very high (>1000 in viral/drug) | Mildly ↑ | Mixed ↑ | Viral hepatitis, DILI, ischaemic hepatitis |
| Cholestatic/Obstructive | Mildly ↑ | Very high (>3× normal) | Conjugated ↑ | Choledocholithiasis, cholangitis, pancreatic CA, PBC, PSC |
| Haemolytic | Normal | Normal | Unconjugated ↑ | Malaria, haemolytic anaemia, G6PD crisis |
| Mixed | Moderately ↑ | Moderately ↑ | Mixed ↑ | Sepsis, alcoholic hepatitis, leptospirosis |
AST:ALT ratio >2:1 — strongly suggests alcoholic hepatitis ALT >1000 IU/L — think viral hepatitis, DILI, ischaemic hepatitis (shock liver)
Step 3 — Imaging
| Modality | Indication | Findings |
|---|---|---|
| USG abdomen | First-line imaging in all patients with jaundice | Bile duct dilatation, gallstones, hepatomegaly, liver abscess, ascites |
| CT abdomen (contrast) | Obstructive/malignant jaundice, liver abscess | Level and cause of obstruction, pancreatic mass, abscess |
| MRCP | Non-invasive bile duct imaging | Choledocholithiasis, PSC (beading), biliary stricture |
| ERCP | Therapeutic in obstructive jaundice | Stone extraction, stenting, brush cytology |
| Liver biopsy | When diagnosis remains unclear after non-invasive workup | Hepatitis histology, cirrhosis grading, granulomas (TB) |
Step 4 — Specific Serological/Microbiological Tests
| Suspected Diagnosis | Specific Test |
|---|---|
| Hepatitis A | Anti-HAV IgM |
| Hepatitis B (acute) | HBsAg, Anti-HBc IgM |
| Hepatitis C | Anti-HCV antibody, HCV RNA PCR |
| Hepatitis E | Anti-HEV IgM (especially in pregnancy) |
| EBV / CMV | Monospot test, EBV VCA IgM, CMV IgM/PCR |
| Leptospirosis | MAT (Microscopic Agglutination Test), IgM ELISA, PCR |
| Malaria | Thick/thin peripheral smear, Rapid Diagnostic Test (HRP-2), PCR |
| Typhoid | Blood culture (gold standard), Widal (limited), PCR |
| Dengue | NS1 antigen (day 1–5), IgM antibody (after day 5) |
| Amoebic liver abscess | Serology (Entamoeba histolytica IgG), USG |
| Autoimmune hepatitis | ANA, ASMA, anti-LKM1, IgG levels |
| Wilson's disease | Serum ceruloplasmin (↓), 24-hr urine copper (↑), slit-lamp |
| PBC | Anti-mitochondrial antibody (AMA-M2) |
| PSC | p-ANCA, MRCP (beading of bile ducts) |
9. DIAGNOSTIC ALGORITHM
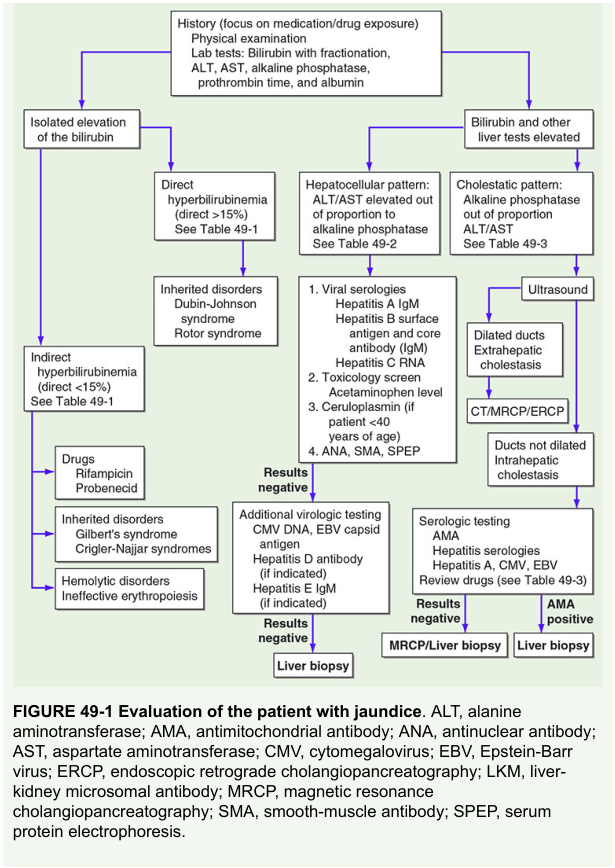
FEVER + JAUNDICE
|
v
History + Physical Examination
|
v
LFTs: Bilirubin fractionation + AST/ALT/ALP/GGT + PT/INR + CBC
|
+---> Unconjugated bilirubin ↑ (direct <15%)
| |
| +--> Haemolytic: Peripheral smear, reticulocyte count,
| Coombs test, LDH, haptoglobin
| Malaria smear/RDT, G6PD screen
|
+---> Conjugated bilirubin ↑ + Hepatocellular pattern
| (AST/ALT very high, ALP mildly ↑)
| |
| +--> Viral serology (HAV, HBV, HCV, HEV, EBV, CMV)
| Drug/alcohol history
| Leptospirosis serology, malaria smear
| Autoimmune hepatitis panel
| USG abdomen
|
+---> Conjugated bilirubin ↑ + Cholestatic pattern
(ALP/GGT very high, AST/ALT mildly ↑)
|
+--> USG abdomen: Bile duct dilated?
|
YES (Extrahepatic obstruction) NO (Intrahepatic cholestasis)
MRCP / CT → stone/stricture/tumour Drugs, PBC, PSC, sepsis,
ERCP if therapeutic needed infiltrative disease
Liver biopsy if needed
10. MANAGEMENT PRINCIPLES
| Category | Management |
|---|---|
| Supportive | IV fluids, antipyretics (avoid paracetamol in hepatic failure), nutrition |
| Haemolytic crisis | Treat precipitant; transfuse if severe anaemia; steroids in autoimmune |
| Viral hepatitis A/E | Supportive; no specific antiviral; monitor for acute liver failure |
| Hepatitis B (acute severe) | Tenofovir/Entecavir if severe; transplant listing if acute liver failure |
| Hepatitis C | Direct-acting antivirals (DAAs) |
| Malaria | Artemisinin combination therapy (uncomplicated); IV Artesunate (severe/cerebral) |
| Leptospirosis | IV Penicillin G or Ceftriaxone; Doxycycline (mild) |
| Ascending cholangitis | IV antibiotics (piperacillin-tazobactam / cefuroxime + metronidazole) + ERCP for decompression |
| Liver abscess | IV antibiotics (amoebic: metronidazole; pyogenic: broad-spectrum) ± percutaneous drainage |
| Alcoholic hepatitis | Abstinence, corticosteroids (prednisolone) if Maddrey's DF >32; N-acetylcysteine; nutrition |
| DILI | Stop offending drug immediately; N-acetylcysteine for paracetamol toxicity |
| Acute liver failure | ICU management, N-acetylcysteine, lactulose, coagulation support, liver transplant evaluation |
| Malignant obstruction | ERCP + stenting; surgery/chemotherapy per staging |
11. EXAM SUMMARY TABLE
| Ask | Answer |
|---|---|
| Earliest sign of jaundice | Scleral icterus (bilirubin >2.5 mg/dL) |
| Fever + RUQ pain + Jaundice | Charcot's triad → Ascending cholangitis |
| Add shock + confusion to above | Reynolds' pentad → Emergency biliary decompression |
| Fever + jaundice + conjunctival suffusion + AKI | Weil's disease (Leptospirosis) |
| Fever + jaundice + anaemia + splenomegaly | Malaria |
| Painless jaundice + palpable gallbladder | Courvoisier's sign → Periampullary/pancreatic carcinoma |
| AST:ALT >2:1 | Alcoholic hepatitis |
| ALT >1000 | Viral hepatitis, ischaemic hepatitis, DILI |
| Best first imaging | Ultrasound abdomen |
| Gold standard for bile ducts | MRCP (non-invasive); ERCP (therapeutic) |
| Jaundice + ANA/ASMA | Autoimmune hepatitis |
| Jaundice + AMA | Primary Biliary Cholangitis (PBC) |
| Jaundice + K-F rings + haemolysis | Wilson's disease |
Forced alkaline diuresis
forced alkaline diuresis mechanism indications technique poisoning
forced alkaline diuresis urine alkalinization poisoning protocol
salicylate poisoning treatment urinary alkalinization ion trapping weak acid
forced diuresis complications contraindications phenobarbital poisoning management
Forced Alkaline Diuresis (Urinary Alkalinization)
Definition
Principle (Ion Trapping)
- Weak acids (HA) become ionized (A⁻) in alkaline urine
- Ionized form is less reabsorbed in renal tubules
- Net effect: increased renal clearance of toxin
Main Indications (high yield)
- Salicylate poisoning (most important indication)
- Phenobarbital poisoning (selected cases)
- Occasionally with other weak acids where evidence supports use
Standard Regimen (practical)
- Correct volume depletion first (isotonic fluids)
- Give IV sodium bicarbonate:
- Common prep: 150 mEq NaHCO₃ in 1 L D5W
- Infuse at rate to maintain urine alkalinity and good urine output
- Targets:
- Urine pH: 7.5 to 8
- Serum pH: avoid severe alkalemia
- Adequate urine output (around 1-2 mL/kg/h)
- Potassium replacement is crucial
- Hypokalemia prevents effective urinary alkalinization
- Frequent monitoring:
- ABG/VBG, serum electrolytes (K⁺, Na⁺, HCO₃⁻), creatinine
- Urine pH hourly initially
Role of Acetazolamide
Complications
- Volume overload/pulmonary edema
- Metabolic alkalosis
- Hypokalemia
- Hypernatremia
- Hypocalcemia (rare symptomatic)
- Worsening in renal failure if not monitored
Contraindications / Relative Contraindications
- Severe renal failure/anuria (ineffective)
- Pulmonary edema or uncompensated heart failure
- Significant alkalemia
- Severe hypokalemia not corrected
- Hemodynamic instability without resuscitation
When to prefer Hemodialysis (especially in salicylate poisoning)
- Severe clinical toxicity (CNS symptoms, pulmonary edema, refractory acidosis)
- Renal failure
- Rising salicylate levels despite treatment
- Inability to alkalinize urine safely