Hhow to interpret chest x ray
Reading File
Finding Sources
Searching the Web
systematic approach chest x-ray interpretation radiology
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Loading Image
Excellent - I have a great lateral chest anatomy diagram and comprehensive textbook content. Now I have everything needed for a thorough, well-structured answer.
How to Interpret a Chest X-Ray (CXR)
A systematic approach ensures nothing is missed. The steps below follow the framework from Pfenninger and Fowler's Procedures for Primary Care with clinical pearls throughout.
Step 1: Before You Interpret - Check Technical Quality (RIP)
Always assess these three factors first. A technically flawed film can mimic or hide pathology.
| Factor | How to Check | What it Means |
|---|---|---|
| R - Rotation | Measure distance from spinous processes to medial clavicular heads on each side. Should be equal (< 2-3 mm difference is acceptable). | Rotation shifts the mediastinum and distorts cardiac silhouette |
| I - Inspiration | Count posterior ribs where they join the spine. A minimally adequate inspiration shows 9 ribs. | Poor inspiration causes apparent opacities that mimic pulmonary edema (CHF) |
| P - Penetration/Exposure | Intervertebral spaces should disappear within the cardiac shadow and NOT be visible below the diaphragm. | Overexposed = film too black (misses lung lesions); Underexposed = film too white (false opacities) |
Always note technique limitations before interpreting - these introduce disclaimers that protect both the patient and clinician.
Step 2: PA vs AP vs Portable
- PA (Posteroanterior) - standard view; beam travels back-to-front; patient stands upright, takes a deep breath. Most accurate for cardiac size.
- AP (Anteroposterior) - portable/bedside; beam travels front-to-back. Cardiomegaly definitions differ - AP views magnify the heart, so don't apply PA cardiac size criteria.
- Lateral view - essential in ambulatory adults. Reveals retrocardiac and retrosternal (anterior clear space) lesions that the PA view misses.
Step 3: Systematic Review - ABCDE Approach
A - Airway
- Is the trachea midline? Deviation suggests tension pneumothorax, large effusion (pushes trachea away), or fibrosis/collapse (pulls trachea toward).
- Check the carina - normally the angle of bifurcation is <70°. Widening (>70°) suggests left atrial enlargement.
- Are the main bronchi visible and symmetric?
B - Breathing / Lungs
This is the most content-rich step. Use a "ping-pong" left-right comparison to detect asymmetries.
Hila:
- In 70% of normals, left hilum is higher than the right. The right hilum is never normally higher than the left.
- Bilateral hilar enlargement = sarcoid, lymphoma, TB, primary pulmonary hypertension.
- Unilateral enlargement = malignancy, TB, infection.
Lung parenchyma:
- Vascular markings normally stop 3-5 mm short of the chest wall.
- Cephalization of flow (enlarged upper lobe vessels) = early CHF.
- Silhouette sign: when a lesion shares the same density as an adjacent border (heart, aorta, diaphragm), that border is "erased." This localizes the lesion:
- Right heart border erased → right middle lobe pathology
- Left heart border erased → lingula pathology
- Diaphragm border erased → lower lobe pathology
Nodules vs Masses:
- Nodule = 5-30 mm diameter
- Mass = >30 mm diameter
- Small lesions 2-10 mm are usually benign calcified granulomas; follow with serial imaging
Pleura:
- Pneumothorax: absent vascular markings extending to the inner thoracic wall (no lung markings reaching the rib edges)
- Pleural effusion: blunting of costophrenic angles; the meniscus sign. Causes include infection, malignancy, CHF, renal failure, hypoalbuminemia, pancreatitis, subphrenic abscess.
- Untreated chronic effusions can loculate and form adhesions.
C - Cardiac Silhouette
Size:
- Cardiothoracic (CT) ratio on PA view: cardiac transverse diameter / thoracic diameter at the same level. Normal = <0.5 (50%).
- If >0.5 on a true PA view = cardiomegaly. (Note: AP views make the heart appear larger - do not use the same cutoff.)
- A "thin heart" in COPD (hyperinflation flattens and elongates it) is not pathological.
Specific findings:
- Enlarged pulmonary artery segment = extra hump on left cardiac border → suggests pulmonary hypertension
- Pneumopericardium = black line around the heart border
- On the lateral view: left ventricular enlargement casts a shadow >2 cm posterior to the inferior vena cava shadow
Borders to identify:
- Right heart border = right atrium
- Left heart border = left ventricle (superior portion = left atrial appendage)
D - Diaphragm
- Right diaphragm is normally higher than left by 2-20 mm (liver pushes it up; gastric bubble is under the left).
- Abnormal elevation of a hemidiaphragm: atelectasis, phrenic nerve palsy, effusion, post-lobectomy.
- Air under the diaphragm (free intraperitoneal air) = surgical emergency until proven otherwise (perforated viscus).
- Check costophrenic angles - should be sharp. Blunting = ~200-300 mL of pleural fluid.
E - Everything Else (Bones, Soft Tissues, Mediastinum, Devices)
Mediastinum:
- Normal width = <8 cm in adults (measured at aortic knob level). If >25% of thoracic diameter at the carina = widened.
- Widened mediastinum: aortic dissection, pericardial tamponade, lymphoma, thymoma, germ cell tumor, thyroid mass.
- "Thin" mediastinum has no clinical significance.
- Note: children <5 years normally have a wide-looking mediastinum and large thymic shadow.
Bones:
- Ribs - fractures, metastatic lesions, notching (coarctation of aorta causes rib notching on the inferior rib margins, 3rd-8th ribs bilaterally)
- Vertebrae - compression fractures, lytic/sclerotic lesions
- Clavicles and shoulder joints
Soft tissues:
- Subcutaneous emphysema
- Breast shadows (can mimic lung opacification)
- Foreign bodies, implanted devices
Lines and tubes (on ICU/portable films):
- ETT tip: should be 3-5 cm above the carina
- Central venous catheter: tip at the SVC-RA junction
- NGT: below the diaphragm, midline
- Chest drains: in the pleural space
Step 4: The Lateral View
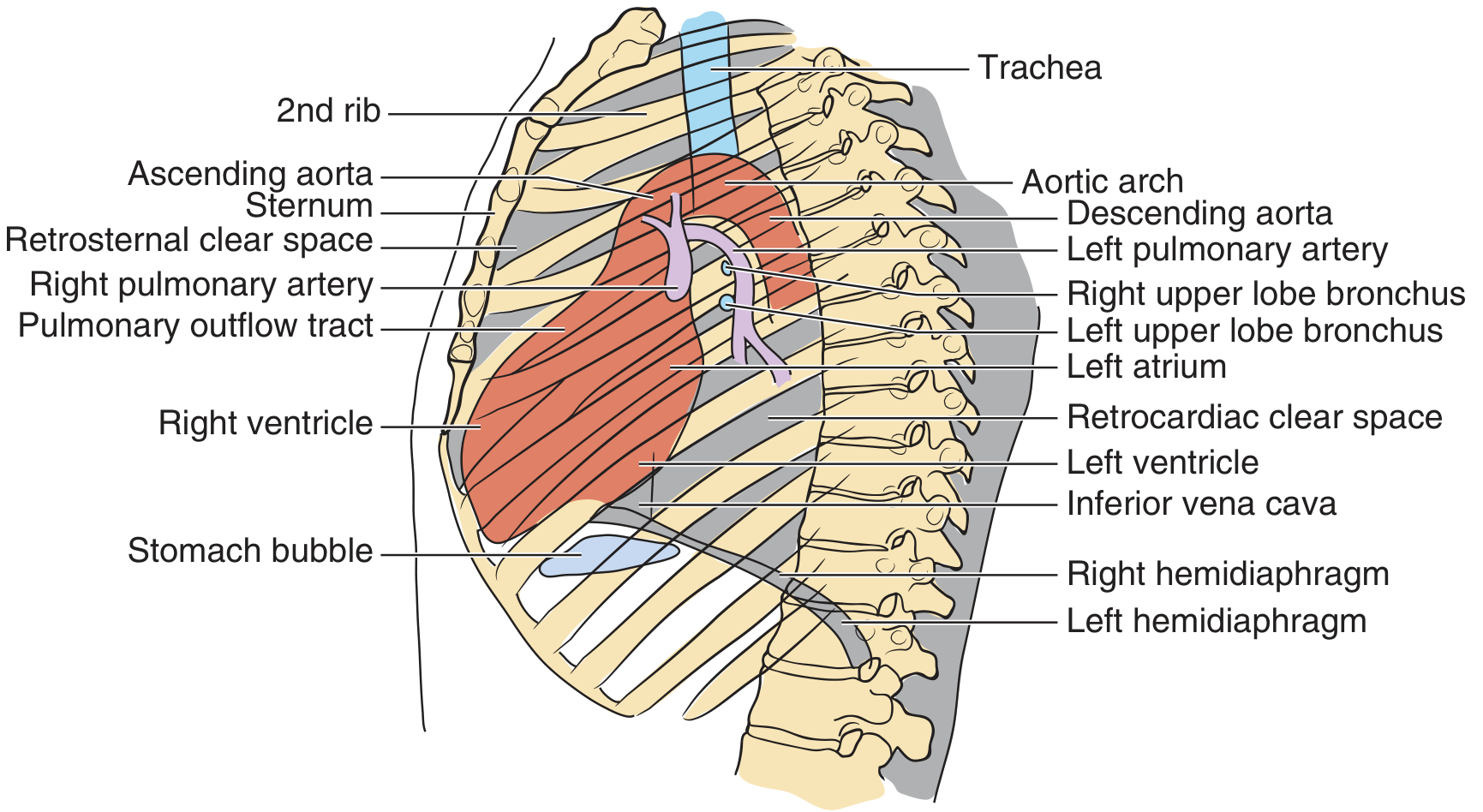
Check four key areas on the lateral:
- Spine - disc spaces, vertebral body density. Normally the vertebrae should appear progressively darker (more lucent) as you go inferiorly. If they get whiter toward the base = posterior lung pathology (e.g., lower lobe consolidation).
- Diaphragms - both should be visible separately. Loss of posterior diaphragm contour = lower lobe consolidation.
- Anterior clear space (retrosternal) - should be clear. Fullness = anterior mediastinal mass (thymoma, teratoma, thyroid, terrible lymphoma - "4 T's").
- Retrocardiac space - should be clear. Opacification = left lower lobe consolidation or effusion.
Step 5: Top 10 "Normal" Benchmarks to Memorize
From Pfenninger & Fowler's Procedures for Primary Care:
- Integrate history and physical - always correlate clinically
- Clavicular heads equidistant from spinous processes (no rotation)
- At least 9 posterior ribs visible on good inspiration
- Intervertebral spaces NOT visible below the diaphragm
- Before age 5, a large thymus can widen the mediastinum normally
- Adults: mediastinum ≤ 8 cm wide
- Left hilum higher than right (normal in 70%)
- Right diaphragm higher than left
- Lesions >10 mm may benefit from a second opinion or CT
- "Chance favors the prepared mind" - experience + pattern recognition builds skill
Common CXR Patterns and Their Diagnoses
| Pattern | Key Features | Think of... |
|---|---|---|
| Consolidation (lobar) | Homogeneous opacity, air bronchograms, silhouette sign | Pneumonia, pulmonary infarction |
| Bilateral perihilar ("bat-wing") haziness | Central opacities, cephalization | Pulmonary edema (CHF) |
| Reticulonodular pattern | Fine "net-like" or nodular shadows | Interstitial lung disease, sarcoid, TB miliary |
| Unilateral whiteout | Entire hemithorax opaque | Massive effusion, collapse, pneumonia |
| Hyperinflation + flat diaphragms | Low flat diaphragms, increased AP diameter | COPD, acute asthma |
| Pneumothorax | Absent lung markings at periphery, visible visceral pleural edge | Trauma, spontaneous, iatrogenic |
| Hilar enlargement | Bilateral symmetric | Sarcoid; unilateral = malignancy/TB |
Summary Workflow
1. Clinical context (symptoms, old films)
2. RIP - check Rotation, Inspiration, Penetration
3. PA + Lateral views both assessed
4. ABCDE: Airway → Breathing → Cardiac → Diaphragm → Everything else
5. Ping-pong comparison: left vs right lung fields
6. Apply silhouette sign to localize lesions
7. Final interpretation: normal / probably insignificant / questionable / abnormal
8. Plan: CT, repeat film, consultation, or immediate action
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Edition, Chapter 231
This is a shared conversation. Sign in to Orris to start your own chat.