Essay on face muscles
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have rich content from multiple authoritative sources. Let me compose the essay.
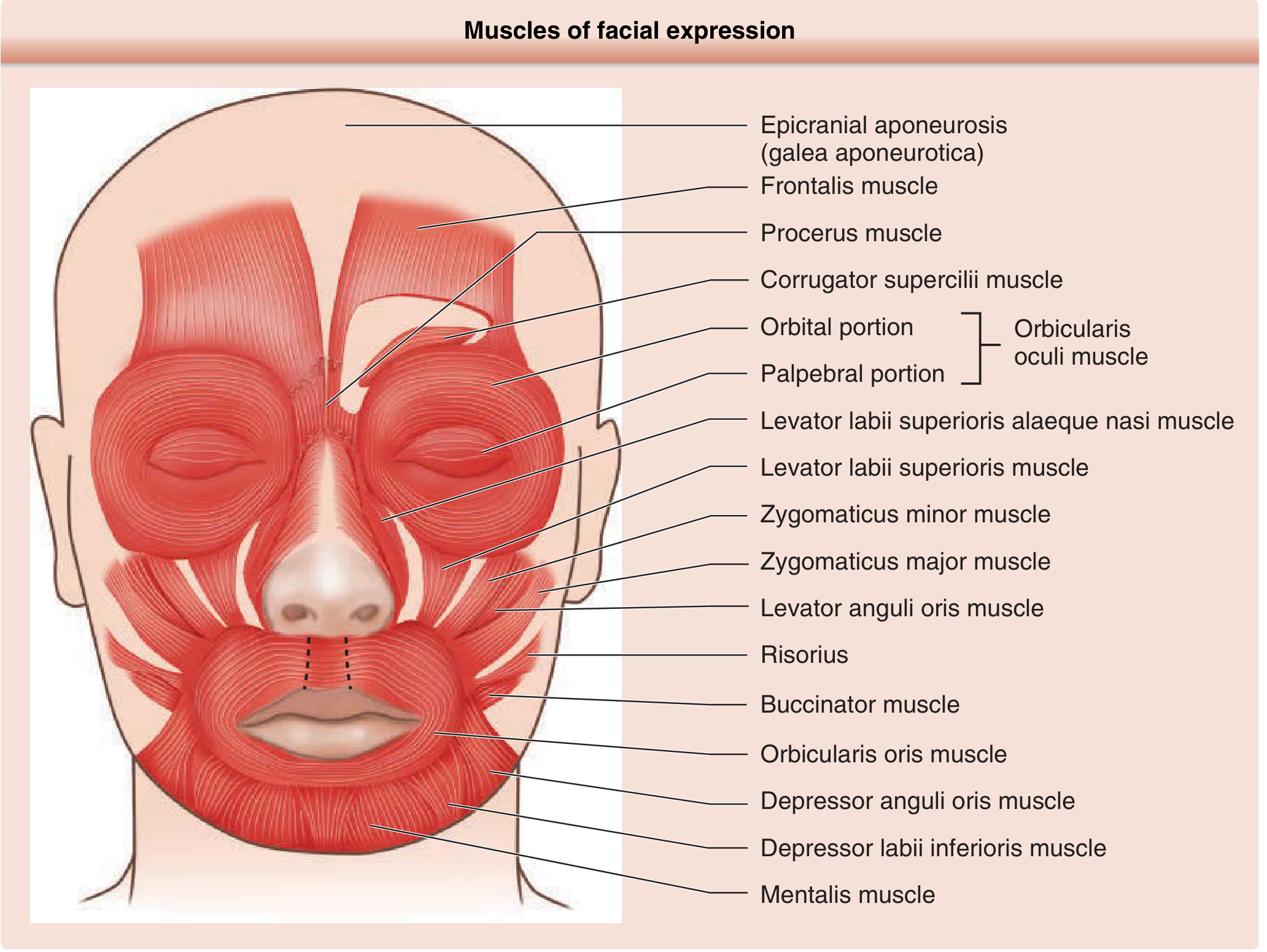
The Muscles of Facial Expression
Origin and Overview
The muscles of facial expression are a unique group of skeletal muscles that arise embryologically from the second branchial arch (hyoid arch). Unlike most skeletal muscles, which attach between two bony points, facial muscles typically have one bony or fascial origin and insert directly into the overlying skin or into adjacent muscle groups. This skin insertion is what gives them the ability to move the integument and produce the subtle gradations of human expression.
All muscles of facial expression are innervated by cranial nerve VII, the facial nerve. They are concentrated in the central facial region and interact closely with the SMAS (superficial musculoaponeurotic system), a fibromuscular sheet that connects the deeper facial skeleton to the superficial skin. Fluidity of facial movement is orchestrated through this SMAS interaction. - Dermatology 2-Volume Set 5e
Innervation: The Facial Nerve (CN VII)
The motor division of the facial nerve arises from the facial motor nucleus in the ventrolateral caudal pontine tegmentum. This nucleus is organized into four subnuclei:
- Dorsomedial group - auricular and occipital muscles
- Intermediate group - frontalis and corrugator muscles
- Ventromedial group - platysma
- Lateral group - buccinator and buccolabial muscles
The facial nerve exits the pons at the cerebellopontine angle, traverses the internal auditory canal, passes through the petrous bone (where it gives off the greater petrosal nerve and chorda tympani), exits via the stylomastoid foramen, and then fans out through the parotid gland into five major peripheral branches:
- Temporal branch
- Zygomatic branch
- Buccal branch
- Marginal mandibular branch
- Cervical branch
An important clinical consideration is supranuclear control: the upper face (frontalis, orbicularis oculi) receives bilateral corticobulbar input, while the lower face receives predominantly crossed (contralateral) input. This explains why a central (upper motor neuron) lesion spares the forehead but causes lower facial weakness contralateral to the lesion, whereas a peripheral (lower motor neuron) lesion causes complete ipsilateral hemifacial palsy. - Localization in Clinical Neurology, 8e
The Muscles by Region
Scalp and Forehead
Epicranius (Occipitofrontalis): The scalp muscles form a functional unit consisting of the frontalis (anterior belly) and the occipitalis (posterior belly), connected across the top of the skull by the galea aponeurotica. Contraction of these muscles allows the scalp skin to slide. Humans have largely lost voluntary control of the posterior occipitalis, which is innervated by the posterior auricular branch of CN VII.
Frontalis: Begins at the anterior hairline and inserts into the forehead skin and eyebrows. It connects with the procerus, orbicularis oculi, and corrugator supercilii. Its primary action is to raise the eyebrows, producing horizontal forehead creases. The two frontalis bellies are separated by a midline gap, which accounts for the vertical creases seen between them. Innervated by the temporal branch.
Corrugator Supercilii: Located over the medial upper orbital rim. It draws the brows medially and downward, producing the characteristic furrowed, "scowling" expression - the vertical glabellar lines. Innervated by the temporal branch.
Procerus: Lies between the two corrugator supercilii muscles. It pulls the medial forehead skin inferiorly, producing horizontal creases at the root of the nose ("bunny lines"). Innervated by the zygomatic branch.
Periorbital Region
Orbicularis Oculi: The major muscle complex acting on the eyelid and periorbital skin. It encircles the entire eye region and has two portions:
- Palpebral portion - overlies the tarsal plate and orbital septum; produces gentle eye closure and blinking (both reflex and voluntary)
- Orbital portion - the outer ring; produces forceful, tight closure (voluntary)
It also functions in tear drainage by helping pump the lacrimal sac. The upper portion is innervated by the temporal branch; the lower portion by the zygomatic branch. Loss causes inability to close the eye (lagophthalmos), threatening corneal exposure and desiccation.
Small Periauricular Muscles (Temporoparietalis group): Arise from the superficial temporalis fascia and lateral galea. They draw back the temporal skin and are innervated by the posterior ramus of the temporal branch. - Dermatology 2-Volume Set 5e
Nasal Region
Nasalis: Has two portions - the transverse portion (compresses the ala) and the alar portion (flares the nostril). Innervated by the zygomatic branch.
Depressor Septi Nasi: Pulls the columella down toward the upper lip, effectively lengthening the nose and narrowing the nostril during facial animation. Innervated by the buccal branch.
Perioral Region - Lip Elevators
Orbicularis Oris: The central sphincter-like muscle surrounding the mouth. It has no bony origin - it is formed by interlacing fibers from all the other perioral muscles plus its own intrinsic fibers. It pursues the lips (for whistling, kissing, and articulation of labial consonants) and provides lip seal. Innervated by both buccal and marginal mandibular branches.
Zygomaticus Major: The principal smile muscle. Runs from the zygomatic bone down to the angle of the mouth, elevating and retracting the lip corners. Innervated by zygomatic and buccal branches.
Zygomaticus Minor: Elevates the upper lip slightly medial to the major, contributing to the "lip curl" component of smiling. Innervated by the buccal branch.
Levator Labii Superioris: Elevates the upper lip directly, contributing to the snarl expression. Innervated by the buccal branch.
Levator Labii Superioris Alaeque Nasi: The longest-named muscle in the human body. Originates from the frontal process of the maxilla and splits to insert into both the upper lip (elevating it) and the alar cartilage (flaring the nostril). Innervated by the buccal branch.
Levator Anguli Oris (Caninus): Deep to the other elevators, originates from the canine fossa of the maxilla. Elevates and retracts the mouth corner. Innervated by zygomatic and buccal branches.
Risorius: A thin, inconstant muscle that runs horizontally from the parotid fascia to the angle of the mouth. Retracts the corner of the mouth to create a tense, "stretched" smile (as opposed to the upward smile of zygomaticus major). Innervated by buccal and/or marginal mandibular branches. Loss causes an asymmetric "crooked" smile at rest.
Perioral Region - Lip Depressors
Depressor Anguli Oris (Triangularis): Pulls the mouth corners downward, contributing to the expression of sadness or displeasure. Innervated by the marginal mandibular branch.
Depressor Labii Inferioris: Pulls the lower lip down and laterally, as in the expression of distaste. Innervated by the marginal mandibular branch.
Mentalis: A paired muscle on the chin that wrinkles the chin skin and everts the lower lip (the "pouting" muscle). Innervated by the marginal mandibular branch.
Cheek
Buccinator: The primary muscle of the cheek, forming most of its wall. Though technically a muscle of facial expression (CN VII innervation - buccal branch), it also plays a role in mastication by keeping food between the teeth. Its key actions are to:
- Appose the cheek against the teeth and gingiva
- Prevent cheek ballooning during high intraoral pressure
- Enable whistling and blowing
Loss of buccinator function causes food to accumulate in the buccal sulcus between the cheek and teeth.
Neck
Platysma: A broad, thin sheet of muscle in the subcutaneous tissue of the neck. While strictly a neck muscle, it is considered a muscle of facial expression because it arises from the second branchial arch, inserts into the lower face and mandible, and contributes to downward pulling of the lower lip and face (expressing distress or strain). Innervated by the cervical branch of CN VII.
Summary Table of Key Muscles
| Muscle | CN VII Branch | Primary Action |
|---|---|---|
| Frontalis | Temporal | Raises eyebrows |
| Corrugator supercilii | Temporal | Scowl - draws brows medially down |
| Orbicularis oculi (upper) | Temporal | Eye closure, blinking |
| Procerus | Zygomatic | Shortens nose, "bunny lines" |
| Orbicularis oculi (lower) | Zygomatic | Lower lid closure |
| Nasalis (alar) | Zygomatic | Nostril flaring |
| Levator anguli oris | Zygomatic + Buccal | Elevates mouth corner |
| Zygomaticus major | Zygomatic + Buccal | Smile - elevates + retracts lip corner |
| Zygomaticus minor | Buccal | Upper lip elevation |
| Levator labii superioris | Buccal | Elevates upper lip |
| Buccinator | Buccal | Cheek apposition, whistling |
| Orbicularis oris | Buccal + Marginal mandibular | Lip purse, lip seal |
| Risorius | Buccal + Marginal mandibular | Retracts mouth corner |
| Depressor anguli oris | Marginal mandibular | Pulls mouth corner down |
| Depressor labii inferioris | Marginal mandibular | Pulls lower lip down |
| Mentalis | Marginal mandibular | Pouts, wrinkles chin |
| Platysma | Cervical | Pulls lower face/lip down |
Skin Tension Lines and Clinical Relevance
The facial muscles contribute directly to relaxed skin tension lines (RSTLs) and eventually to wrinkles. Since skin creases form perpendicular to the direction of muscle fiber pull, knowing muscle orientation predicts crease location:
- Frontalis fibers run vertically → horizontal forehead lines
- Corrugator fibers run obliquely/horizontally → vertical glabellar lines
- Orbicularis oculi fibers run circumferentially around the eye → radial "crow's feet" lines
This anatomical knowledge is foundational for:
- Surgical incision planning (incisions along RSTLs heal with minimal scarring)
- Botulinum toxin injections (targeting specific muscles to reduce dynamic wrinkles)
- Reconstructive and aesthetic surgery (understanding SMAS layers, danger zones for nerve injury)
- Neurological examination (localizing facial nerve lesions to peripheral branch vs. central origin)
Clinical Conditions Affecting Face Muscles
Bell's Palsy: Idiopathic peripheral CN VII palsy causing complete unilateral loss of all facial muscle function - the entire ipsilateral face, including the forehead (distinguishing it from a central lesion). Complications include lagophthalmos (exposure keratopathy), food pooling in the buccal sulcus, and drooling from orbicularis oris weakness.
Upper Motor Neuron (Central) Facial Palsy: Stroke or other supranuclear lesions cause contralateral lower facial weakness with relative sparing of the upper face, because the dorsal facial nucleus (innervating frontalis and orbicularis oculi) receives bilateral corticobulbar input.
Hemifacial Spasm: Involuntary, unilateral, intermittent contractions of facial expression muscles, typically starting around the orbicularis oculi, caused by vascular compression of CN VII at the root entry zone.
Sources
- Dermatology 2-Volume Set 5e - Chapter 142 (Surgical Anatomy of the Face) and Chapter 201
- Fitzpatrick's Dermatology, Vol. 1-2
- Localization in Clinical Neurology, 8e
- Netter's Atlas of Human Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.