
What is the disease and give appropriate treatment for the same
hyperkeratosis foot callus treatment
Diagnosis: Plantar Wart (Verruca Plantaris) with Hyperkeratotic Callus
- Thick white/yellow keratotic buildup over the toe
- Dry, cracked, scaly surface with a rough texture
- Localized to a pressure/friction point
Treatment
Step 1 - General Measures (for all patients)
- Soak the lesion in warm water, then pare/debride the callus with a pumice stone or blade before any treatment - this improves penetration of all agents
- Eat a diet rich in fruits and vegetables; supplement with folic acid 1 mg
- Avoid smoking (reduces skin immunity via Langerhans cell depletion)
- Enhance immune function as much as possible
Step 2 - First-Line: Over-the-Counter Topicals (mild/early lesions)
- Salicylic acid 17-40% (Compound-W, Dr. Scholl's, Mediplast, Occlusal, DuoFilm)
- After soaking and paring, apply every 48 hours under occlusion
- Remove dead tissue between applications with pumice or paring
- Continue for 4-6 weeks with consistent daily use
- Non-scarring; effective but requires compulsive adherence
Step 3 - Physician-Applied Options
| Treatment | Details |
|---|---|
| Cryotherapy (liquid nitrogen) | First-line office treatment; does not cause scarring; highly effective for plantar warts; preferred over surgery |
| Bichloracetic or Trichloroacetic Acid (50-85%) | Applied by physician after paring; caustic - not for home use |
| Cantharidin 0.7% | Applied in office, causes blister formation; effective |
| 5-Fluorouracil 5% cream | Topical antimetabolite |
| Imiquimod (Aldara) | Immunomodulator; pare callus first, rub in thoroughly |
| Tretinoin 0.05-0.1% | Can be used adjunctively |
Important: Avoid surgical excision on the plantar surface/toes - scar tissue is often permanently painful, like a pebble in a shoe.
Step 4 - Preferred for Large or Persistent Lesions: Candida Antigen Injection
- Candida antigen (Candin 1:500) is now the first-line approach for all but the simplest cases
- Mix 1:1 with 1-2% lidocaine without epinephrine; inject 0.1-0.3 mL intralesionally with a 30-gauge needle
- Repeat at 1-month intervals x 3 sessions
- Expected efficacy: 65-75% with first injection; 80-85% after three treatments
- Advantages: Minimal scarring, no "downtime," rare adverse reactions, immune activation can clear all warts (not just injected ones)
Step 5 - Refractory Cases: Bleomycin
- Bleomycin 1 U/mL injected intralesionally at 1-month intervals x 3
- Reserved for failure of Candida antigen or other methods
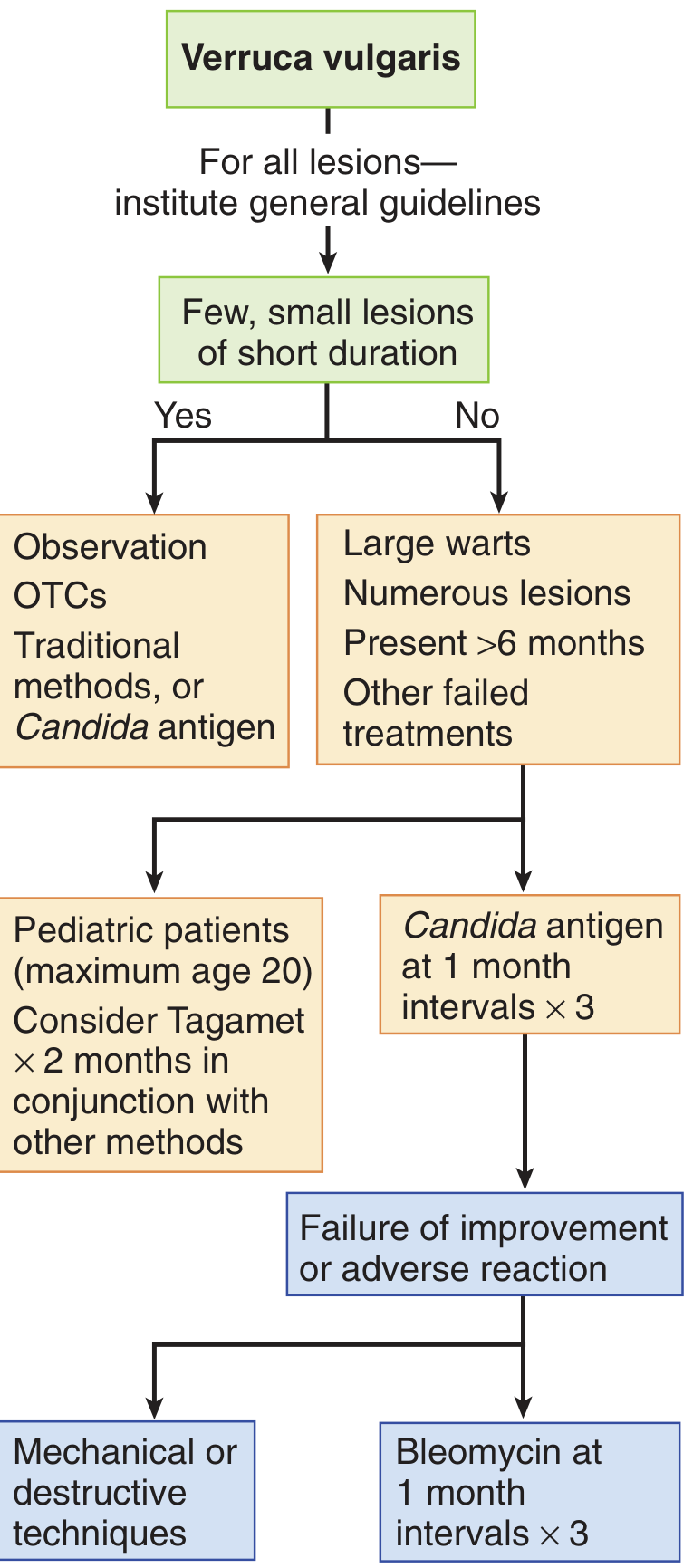
Treatment Algorithm (from Pfenninger and Fowler's Procedures for Primary Care)
Key Points
- 60% of warts resolve spontaneously over time, so watchful waiting is reasonable in mild, asymptomatic cases
- Recurrence rates with all treatments are 30% or higher - this is expected
- The virus is never fully eliminated; the immune system keeps it in remission
- If the diagnosis is uncertain (wart vs. callus vs. other), obtain a shave biopsy before treating
- In immunosuppressed patients, success rates are significantly lower and HPV-associated malignancy risk is elevated
Disclaimer: This information is for educational purposes. Please consult a dermatologist or podiatrist for diagnosis confirmation and individualized treatment.
Create a patient education handout on plantar wart causes and home care
ls -la /home/daytona/workspace/ && ls /home/daytona/skills/docx/
mkdir -p /home/daytona/workspace/plantar-wart-handout
~/plantar-wart-handout/create_handout.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
VerticalAlign, UnderlineType, PageNumber, Footer, Header
} = require('docx');
const fs = require('fs');
// ── colour palette ────────────────────────────────────────────────────────────
const TEAL = "006D77"; // headings / accent
const TEAL_PALE = "E8F4F6"; // shaded box backgrounds
const RED = "C0392B"; // warning text
const DARK_GREY = "2C3E50"; // body text
const WHITE = "FFFFFF";
const TEAL_MED = "83C5BE"; // table header bg
// ── helper: bold teal heading paragraph ──────────────────────────────────────
function sectionHeading(text) {
return new Paragraph({
spacing: { before: 240, after: 80 },
children: [
new TextRun({
text,
bold: true,
size: 28, // 14 pt
color: TEAL,
font: "Calibri",
}),
],
border: {
bottom: { color: TEAL, size: 6, style: BorderStyle.SINGLE, space: 4 },
},
});
}
// ── helper: body paragraph ───────────────────────────────────────────────────
function bodyPara(text, { bold = false, color = DARK_GREY, size = 22, indent = 0, spaceAfter = 100 } = {}) {
return new Paragraph({
spacing: { after: spaceAfter },
indent: indent ? { left: indent } : undefined,
children: [
new TextRun({ text, bold, color, size, font: "Calibri" }),
],
});
}
// ── helper: bullet ───────────────────────────────────────────────────────────
function bullet(text, { bold = false, color = DARK_GREY } = {}) {
return new Paragraph({
bullet: { level: 0 },
spacing: { after: 80 },
children: [
new TextRun({ text, bold, color, size: 22, font: "Calibri" }),
],
});
}
// ── helper: sub-bullet ───────────────────────────────────────────────────────
function subBullet(text) {
return new Paragraph({
bullet: { level: 1 },
spacing: { after: 60 },
children: [
new TextRun({ text, size: 21, color: DARK_GREY, font: "Calibri" }),
],
});
}
// ── helper: shaded info box ───────────────────────────────────────────────────
function infoBox(lines, { bgColor = TEAL_PALE, labelColor = TEAL, bodyColor = DARK_GREY } = {}) {
const rows = lines.map((line, i) =>
new TableRow({
children: [
new TableCell({
shading: { fill: bgColor, type: ShadingType.CLEAR },
margins: { top: 80, bottom: 80, left: 160, right: 160 },
borders: {
top: { style: i === 0 ? BorderStyle.SINGLE : BorderStyle.NONE, color: TEAL, size: 8 },
bottom: { style: i === lines.length - 1 ? BorderStyle.SINGLE : BorderStyle.NONE, color: TEAL, size: 8 },
left: { style: BorderStyle.THICK, color: TEAL, size: 12 },
right: { style: BorderStyle.SINGLE, color: TEAL, size: 8 },
},
children: [
new Paragraph({
spacing: { after: 40 },
children: [
new TextRun({
text: line.label ? `${line.label} ` : "",
bold: true,
color: labelColor,
size: 22,
font: "Calibri",
}),
new TextRun({
text: line.text,
color: bodyColor,
size: 22,
font: "Calibri",
}),
],
}),
],
}),
],
})
);
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows,
margins: { top: 160, bottom: 160 },
});
}
// ── helper: two-column table ─────────────────────────────────────────────────
function twoColTable(headers, rows) {
const headerRow = new TableRow({
tableHeader: true,
children: headers.map(h =>
new TableCell({
shading: { fill: TEAL, type: ShadingType.CLEAR },
verticalAlign: VerticalAlign.CENTER,
margins: { top: 100, bottom: 100, left: 160, right: 160 },
children: [
new Paragraph({
alignment: AlignmentType.CENTER,
children: [new TextRun({ text: h, bold: true, color: WHITE, size: 22, font: "Calibri" })],
}),
],
})
),
});
const dataRows = rows.map((row, ri) =>
new TableRow({
children: row.map(cell =>
new TableCell({
shading: { fill: ri % 2 === 0 ? WHITE : TEAL_PALE, type: ShadingType.CLEAR },
margins: { top: 80, bottom: 80, left: 160, right: 160 },
children: [
new Paragraph({
children: [new TextRun({ text: cell, size: 21, color: DARK_GREY, font: "Calibri" })],
}),
],
})
),
})
);
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
rows: [headerRow, ...dataRows],
});
}
// ── warning box ───────────────────────────────────────────────────────────────
function warningBox(lines) {
return infoBox(lines, { bgColor: "FFF3CD", labelColor: "856404", bodyColor: "856404" });
}
// ── spacer paragraph ─────────────────────────────────────────────────────────
function spacer(size = 120) {
return new Paragraph({ spacing: { after: size }, children: [] });
}
// ─────────────────────────────────────────────────────────────────────────────
// DOCUMENT BUILD
// ─────────────────────────────────────────────────────────────────────────────
const doc = new Document({
styles: {
default: {
document: {
run: { font: "Calibri", size: 22, color: DARK_GREY },
},
},
},
sections: [
{
properties: {
page: {
margin: { top: 720, bottom: 720, left: 900, right: 900 },
},
},
headers: {
default: new Header({
children: [
new Paragraph({
alignment: AlignmentType.CENTER,
shading: { fill: TEAL, type: ShadingType.CLEAR },
spacing: { before: 0, after: 0 },
border: { bottom: { color: TEAL_MED, size: 6, style: BorderStyle.SINGLE } },
children: [
new TextRun({ text: "PATIENT EDUCATION HANDOUT", bold: true, color: WHITE, size: 22, font: "Calibri", allCaps: true }),
],
}),
],
}),
},
footers: {
default: new Footer({
children: [
new Paragraph({
alignment: AlignmentType.CENTER,
border: { top: { color: TEAL, size: 6, style: BorderStyle.SINGLE } },
children: [
new TextRun({ text: "This handout is for educational purposes only. Always follow your doctor's instructions. | Page ", size: 18, color: "888888", font: "Calibri" }),
new TextRun({ children: [PageNumber.CURRENT], size: 18, color: "888888", font: "Calibri" }),
],
}),
],
}),
},
children: [
// ── TITLE BLOCK ──────────────────────────────────────────────────────
spacer(200),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { after: 60 },
children: [
new TextRun({ text: "Plantar Warts", bold: true, size: 56, color: TEAL, font: "Calibri" }),
],
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { after: 40 },
children: [
new TextRun({ text: "Verruca Plantaris", italics: true, size: 28, color: "888888", font: "Calibri" }),
],
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { after: 280 },
children: [
new TextRun({ text: "Understanding Your Condition & Caring for It at Home", size: 24, color: DARK_GREY, font: "Calibri" }),
],
}),
// ── WHAT IS A PLANTAR WART? ──────────────────────────────────────────
sectionHeading("What Is a Plantar Wart?"),
bodyPara(
"A plantar wart is a non-cancerous (benign) skin growth that appears on the sole, heel, or toes of the foot. " +
"Unlike warts on other parts of the body, plantar warts are often pushed inward by the pressure of walking and standing, " +
"which can make them feel like a small pebble stuck in your shoe."
),
spacer(80),
infoBox([
{ label: "Medical name:", text: "Verruca Plantaris" },
{ label: "Caused by:", text: "Human Papillomavirus (HPV) — types 1, 2, and 4" },
{ label: "Who gets it:", text: "Anyone, but most common in children, teenagers, and adults who walk barefoot in shared spaces" },
{ label: "Is it cancer?", text: "No. Plantar warts are benign skin growths." },
]),
spacer(160),
// ── HOW DO YOU RECOGNISE ONE? ─────────────────────────────────────────
sectionHeading("How Do You Recognise a Plantar Wart?"),
bodyPara("Look for these signs on the bottom of your foot or toes:"),
bullet("A rough, grainy, thickened patch of skin — often with a yellowish-white colour"),
bullet("Tiny black dots within the lesion (these are small clotted blood vessels, often called \"wart seeds\")"),
bullet("Pain or tenderness when you press the wart sideways (squeezing), rather than directly downward"),
bullet("Skin lines (fingerprint ridges) that appear interrupted or displaced around the area"),
bullet("A flat, hard area with a callus-like covering — the wart may be buried beneath it"),
spacer(100),
warningBox([
{ label: "Key difference from a callus:", text: "When the top layer of a wart is gently pared away, tiny pinpoint bleeding spots appear. A simple callus does NOT bleed when pared. If you are unsure, see your doctor." },
]),
spacer(160),
// ── CAUSES & HOW IT SPREADS ───────────────────────────────────────────
sectionHeading("Causes & How It Spreads"),
bodyPara(
"Plantar warts are caused by HPV, a common virus that enters the skin through tiny cuts, " +
"breaks, or areas of soft (macerated) skin on the sole of the foot. HPV thrives in warm, moist environments."
),
spacer(80),
bodyPara("Common ways plantar warts spread:", { bold: true, color: TEAL }),
bullet("Walking barefoot in communal areas: swimming pools, locker rooms, gym showers, hotel rooms"),
bullet("Direct contact with another person's wart"),
bullet("Touching your own wart and then touching another area of skin (self-spread / autoinoculation)"),
bullet("Sharing towels, socks, shoes, or nail files with someone who has a wart"),
spacer(80),
bodyPara("Factors that increase your risk:", { bold: true, color: TEAL }),
bullet("Cuts, scrapes, or blisters on the foot that let the virus enter"),
bullet("Sweaty feet — moisture weakens the skin barrier"),
bullet("A weakened immune system (e.g., diabetes, steroid medications, HIV)"),
bullet("Children and teenagers (their immune systems have not yet encountered HPV)"),
bullet("Previous warts — the virus can remain dormant and reactivate"),
spacer(160),
// ── HOME CARE STEP BY STEP ────────────────────────────────────────────
sectionHeading("Home Care: Step-by-Step"),
bodyPara(
"Most mild plantar warts can be treated at home with over-the-counter salicylic acid products " +
"(e.g., Compound-W, Dr. Scholl's Clear Away, Mediplast). Treatment requires patience — it typically " +
"takes 4 to 8 weeks of consistent daily care."
),
spacer(80),
// numbered steps via table
twoColTable(
["Step", "What to Do"],
[
["1. Soak", "Soak your foot in warm water for 10–15 minutes to soften the skin. This allows the treatment to penetrate more deeply."],
["2. Pare / File", "Gently rub the wart surface with a pumice stone, emery board, or disposable nail file. Remove only the white, dead skin on top. Stop if you see pink skin or feel any pain. Wash your hands and the tool afterwards — do not share the file."],
["3. Dry", "Pat the area completely dry before applying any treatment."],
["4. Apply salicylic acid", "Apply the salicylic acid product (liquid, gel, or pad) directly onto the wart only. Avoid surrounding healthy skin. Many products include an applicator for precision."],
["5. Cover", "Cover the wart with a small adhesive bandage or medical tape after applying the product. Occlusion (covering) improves results."],
["6. Repeat", "Repeat every 24–48 hours. Before each session, re-soak and re-file to remove the dead tissue that has built up."],
]
),
spacer(160),
// ── OVER-THE-COUNTER PRODUCTS ──────────────────────────────────────────
sectionHeading("Over-the-Counter Products to Use"),
twoColTable(
["Product Type", "Examples / Strength"],
[
["Salicylic acid liquid/gel", "Compound-W, Occlusal, Wart-Off (17%)"],
["Salicylic acid pads", "Compound-W Maximum Strength Pads, Dr. Scholl's Clear Away Strips (40%)"],
["Salicylic acid plasters", "Mediplast, Sal-Plant Gel (40%)"],
["Duct tape occlusion", "Plain grey duct tape — cover for 6 days, soak and file on day 7, leave uncovered overnight, repeat. Low-risk adjunct therapy."],
]
),
spacer(100),
infoBox([
{ label: "Tip:", text: "Higher-strength 40% salicylic acid pads are more effective for thick, callused plantar warts. Apply every 48 hours." },
]),
spacer(160),
// ── GENERAL HEALTH TIPS ───────────────────────────────────────────────
sectionHeading("General Health Tips to Support Recovery"),
bodyPara("Your immune system is your best weapon against HPV. Support it by:"),
bullet("Eating plenty of fruits and vegetables rich in vitamins A, C, and E"),
bullet("Taking a daily multivitamin that includes folic acid (1 mg)"),
subBullet("Folic acid supports skin cell repair and immune response"),
bullet("Staying well-hydrated"),
bullet("Avoiding smoking — smoking reduces the number of immune cells (Langerhans cells) in your skin and makes warts harder to treat"),
bullet("Getting adequate sleep and managing stress"),
spacer(160),
// ── PREVENTING SPREAD ─────────────────────────────────────────────────
sectionHeading("Preventing Spread to Others (and Yourself)"),
bullet("Always wear flip-flops or sandals in communal showers, pools, and changing rooms"),
bullet("Do NOT share towels, socks, shoes, or any files/tools used on the wart"),
bullet("Wash your hands thoroughly after touching the wart or applying treatment"),
bullet("Keep the wart covered with a bandage or waterproof plaster, especially in shared spaces"),
bullet("Do not scratch, pick, or bite the wart — this can spread HPV to other parts of your body or to other people"),
bullet("If you have a cut or open sore on your foot, keep it clean and covered"),
spacer(160),
// ── WHAT NOT TO DO ────────────────────────────────────────────────────
sectionHeading("What NOT to Do at Home"),
warningBox([
{ label: "Do NOT:", text: "Try to cut, scrape off, or burn the wart yourself with sharp tools or household chemicals. This can cause infection and scarring." },
{ label: "Do NOT:", text: "Apply salicylic acid to healthy surrounding skin, broken skin, or on the face. Use petroleum jelly (Vaseline) around the wart to protect the healthy skin nearby." },
{ label: "Do NOT:", text: "Ignore warts that grow rapidly, multiply, or change in appearance — see a doctor." },
{ label: "Do NOT:", text: "Walk barefoot while actively treating a wart, especially around others." },
]),
spacer(160),
// ── WHEN TO SEE YOUR DOCTOR ───────────────────────────────────────────
sectionHeading("When to See Your Doctor"),
bodyPara("Home treatment is not always enough. Book an appointment if:"),
bullet("The wart has not improved after 4–6 weeks of consistent home treatment"),
bullet("The wart is growing larger, multiplying, or spreading to other toes"),
bullet("You have significant pain that affects your walking"),
bullet("You are diabetic or have poor circulation in your feet — do NOT attempt home treatment without medical advice"),
bullet("The wart is in an unusual location (on the nail, around the nail, or on a child under 12)"),
bullet("You are unsure whether it is a wart or something else"),
bullet("You are immunocompromised (on steroids, chemotherapy, or have HIV)"),
spacer(80),
infoBox([
{ label: "Doctor's treatments available:", text: "Cryotherapy (freezing), trichloroacetic acid, Candida antigen injection, cantharidin, bleomycin injection, and more — all performed safely in a clinic." },
]),
spacer(160),
// ── FREQUENTLY ASKED QUESTIONS ────────────────────────────────────────
sectionHeading("Frequently Asked Questions"),
bodyPara("Will my wart go away on its own?", { bold: true, color: TEAL }),
bodyPara(
"Yes — about 60% of plantar warts resolve on their own within 2 years, especially in children. " +
"However, they may persist or multiply in adults and those with a weakened immune system. " +
"Treatment speeds up resolution and reduces the chance of spread."
),
bodyPara("Will the wart come back after treatment?", { bold: true, color: TEAL }),
bodyPara(
"Possibly. Recurrence rates are 30% or higher with all treatment methods. " +
"The HPV virus is never fully eliminated from the body — the immune system keeps it in remission, " +
"similar to how herpes virus behaves. Maintaining a strong immune system helps prevent recurrence."
),
bodyPara("Is it safe to exercise or swim with a plantar wart?", { bold: true, color: TEAL }),
bodyPara(
"Yes, but keep the wart covered with a waterproof bandage or plantar wart pad. " +
"This protects others from exposure and prevents the wart from picking up new HPV strains."
),
bodyPara("Can my child go to school with a plantar wart?", { bold: true, color: TEAL }),
bodyPara(
"Yes. Children do not need to be kept home from school. Simply keep the wart covered, " +
"have them wear footwear in changing rooms, and avoid sharing shoes or socks."
),
spacer(200),
// ── DISCLAIMER ────────────────────────────────────────────────────────
new Paragraph({
spacing: { after: 0 },
border: {
top: { color: TEAL, size: 6, style: BorderStyle.SINGLE, space: 6 },
},
children: [
new TextRun({
text: "This handout provides general health information only and is not a substitute for professional medical advice, diagnosis, or treatment. " +
"Always consult your healthcare provider before starting or changing any treatment.",
size: 18,
color: "888888",
italics: true,
font: "Calibri",
}),
],
}),
],
},
],
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync("/home/daytona/workspace/plantar-wart-handout/Plantar_Wart_Patient_Handout.docx", buffer);
console.log("Done: Plantar_Wart_Patient_Handout.docx created.");
}).catch(err => {
console.error("Error:", err);
process.exit(1);
});
cd /home/daytona/workspace/plantar-wart-handout && node create_handout.js 2>&1
python /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/workspace/plantar-wart-handout/Plantar_Wart_Patient_Handout.docx 2>&1
python3 -c " import zipfile, sys path = '/home/daytona/workspace/plantar-wart-handout/Plantar_Wart_Patient_Handout.docx' try: with zipfile.ZipFile(path) as z: names = z.namelist() print('Valid ZIP. Files:', names[:10]) content = z.read('word/document.xml') print('document.xml size:', len(content), 'bytes') print('First 300 chars:', content[:300].decode('utf-8', errors='replace')) except Exception as e: print('Error:', e) "
Plantar Wart Patient Handout
Word Document · DOCX
| Section | Content |
|---|---|
| What Is a Plantar Wart? | Plain-language definition, medical name, HPV types, benign nature |
| How to Recognise One | Key visual signs including the "black dots" and wart vs. callus distinction |
| Causes & How It Spreads | HPV mechanism, common transmission routes, risk factors |
| Home Care Step-by-Step | 6-step illustrated table: soak → pare → dry → apply → cover → repeat |
| OTC Products to Use | Named products by type and strength (17% vs. 40% salicylic acid, duct tape method) |
| General Health Tips | Diet, folic acid, smoking cessation, immune support |
| Preventing Spread | Footwear, hygiene, not sharing tools, keeping wart covered |
| What NOT to Do | Highlighted warning boxes for dangerous home remedies |
| When to See Your Doctor | Clear red-flag criteria including diabetes, rapid growth, failed home treatment |
| FAQ | Spontaneous resolution, recurrence, exercising safely, school attendance |
Make pdf
python /home/daytona/skills/docx/scripts/office/soffice.py --headless --convert-to pdf /home/daytona/workspace/plantar-wart-handout/Plantar_Wart_Patient_Handout.docx --outdir /home/daytona/workspace/plantar-wart-handout/ 2>&1
ls -la /home/daytona/workspace/plantar-wart-handout/ && libreoffice --headless --convert-to pdf /home/daytona/workspace/plantar-wart-handout/Plantar_Wart_Patient_Handout.docx --outdir /home/daytona/workspace/plantar-wart-handout/ 2>&1
cp /home/daytona/workspace/plantar-wart-handout/Plantar_Wart_Patient_Handout.docx /tmp/pwh.docx && libreoffice --headless --convert-to pdf /tmp/pwh.docx --outdir /tmp/ 2>&1 && ls -lh /tmp/pwh.pdf
cp /tmp/pwh.pdf /home/daytona/workspace/plantar-wart-handout/Plantar_Wart_Patient_Handout.pdf && ls -lh /home/daytona/workspace/plantar-wart-handout/
Plantar Wart Patient Handout
PDF Document · PDF
Plantar Wart Patient Handout
Word Document · DOCX