Hernia of stomach
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hiatal hernia" management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Let me compile a thorough answer.
Hernia of the Stomach (Hiatal Hernia)
A hiatal hernia is the herniation of viscera - most commonly the stomach - into the mediastinum through the esophageal hiatus of the diaphragm. It is the most clinically important hernia of the stomach.
Classification (4 Types)
| Type | Name | Description |
|---|---|---|
| I | Sliding hernia | The esophagogastric junction (EGJ) AND gastric cardia herniate above the diaphragm; stomach axis is unchanged. Accounts for ~90-95% of all hiatal hernias. |
| II | True paraesophageal hernia | Fundus of stomach herniates alongside the esophagus while the EGJ stays normally positioned below the diaphragm. |
| III | Mixed (combined) hernia | Both the EGJ is above the hiatus AND a portion of the stomach is folded alongside the esophagus. Most "paraesophageal" hernias in practice are this type. |
| IV | Complex hernia | Additional intra-abdominal organs (colon, omentum, spleen) also herniate through the hiatus. |
Types II, III, and IV are collectively called paraesophageal hernias (PEH).
Anatomy & Pathophysiology
The phrenoesophageal ligament (membrane) normally anchors the EGJ to the diaphragm at the hiatus. Hiatal hernias result from:
- Age-related deterioration of this membrane
- Dilatation of the diaphragmatic hiatus
- Chronic elevated intra-abdominal pressure (obesity, pregnancy, chronic straining)
- Esophageal traction pulling the stomach cephalad during swallowing
Type I hernias are essentially "wear and tear" hernias - they enlarge with increased intra-abdominal pressure, swallowing, and respiration.
With types II and III, the stomach progressively inverts as it herniates - large PEH can lead to an "upside-down stomach" and gastric volvulus.
- Harrison's Principles of Internal Medicine 22E, p. 2549
- Sleisenger and Fordtran's GI and Liver Disease
Epidemiology
- Prevalence varies widely (14-84%) depending on population and diagnostic method
- More frequent in patients with GERD
- Incidence increases with age
- Symptomatic PEH most commonly presents in middle-aged to older adults
Clinical Features
Type I (Sliding) Hernia
- Often asymptomatic when small
- Main significance: predisposition to GERD (heartburn, regurgitation)
- Large hernias may cause dysphagia, chest or upper abdominal discomfort
- Cameron lesions (linear erosions at lesser curve at the diaphragmatic hiatus level) occur in ~5% of hiatal hernia patients, up to ~30% in large PEH - can cause iron deficiency anemia
Types II, III, IV (Paraesophageal Hernias)
Rarely fully asymptomatic; symptoms include:
- Early satiety and postprandial fullness
- Dysphagia and chest pain
- Shortness of breath (post-prandial) from intrathoracic stomach
- Iron deficiency anemia (30-40%) from chronic GI blood loss via Cameron lesions
- Weight loss and vomiting
- Risk of gastric volvulus - a potentially life-threatening complication presenting with acute pain and retching, progressing to strangulation and perforation
Investigations
| Test | Findings |
|---|---|
| Chest X-ray | Soft tissue density or air-fluid level in retrocardiac area |
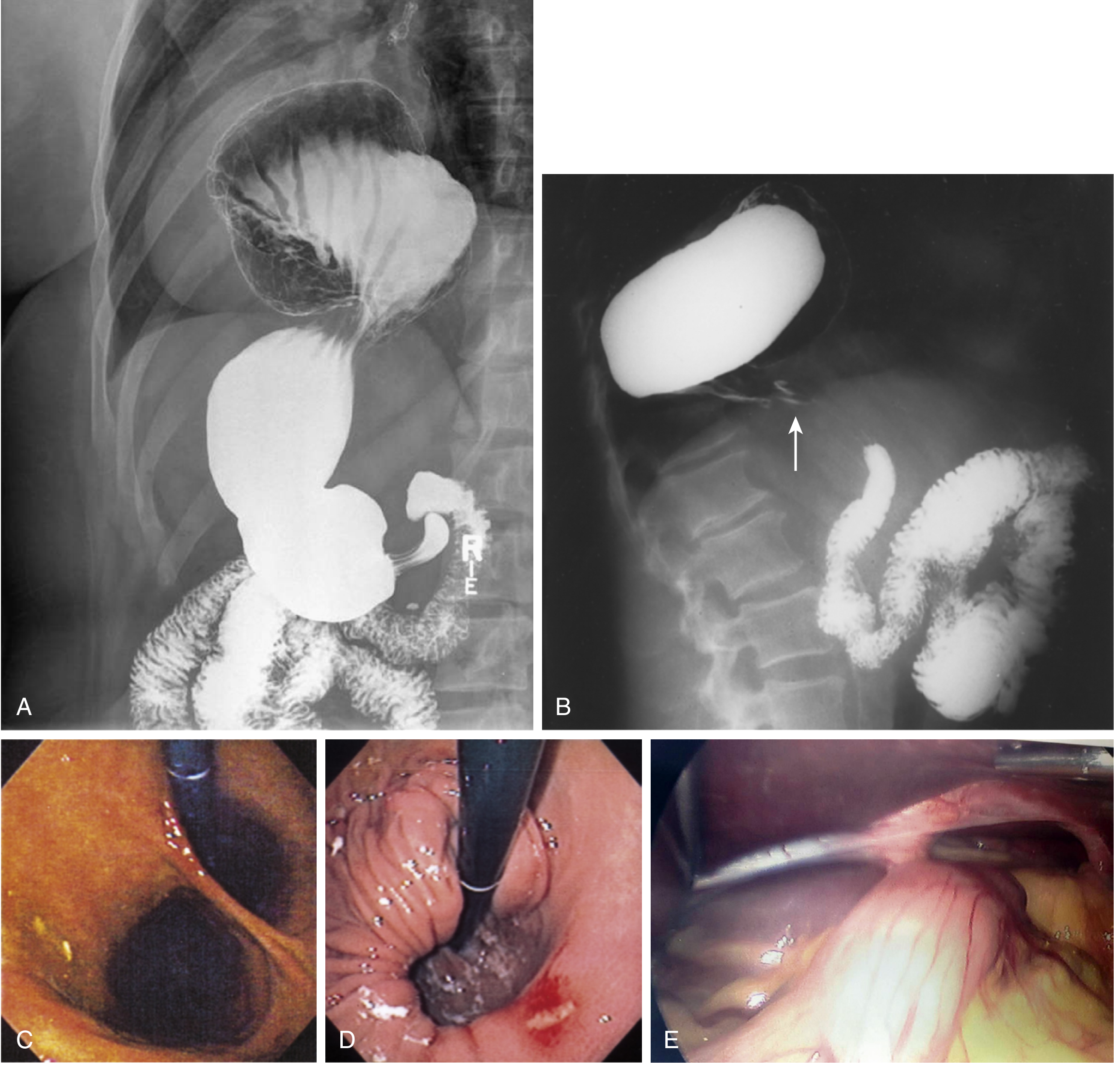
| Barium swallow (UGI) | Best initial test - shows stomach above diaphragm, type of hernia, presence of volvulus |
| CT scan | Excellent for type IV - delineates anatomy, identifies organs herniated (colon, spleen, pancreas) |
| Upper endoscopy | Confirms diagnosis; detects esophagitis, gastritis, Cameron lesions, malignancy |
| Esophageal manometry | Assesses motility disorders; guides fundoplication choice |
| 24-hr pH/impedance | Confirms GERD, quantifies acid exposure |
Treatment
Medical (Type I / Asymptomatic)
- Simple sliding hernias do not require treatment unless symptomatic from reflux
- Proton pump inhibitors (PPIs) for GERD management
- Lifestyle modifications (weight loss, head-of-bed elevation, dietary changes)
Surgical Indications
Surgery is offered when:
- Symptomatic PEH (types II, III, IV) - postprandial pain, dysphagia, weight loss, anemia
- Gastric volvulus or strangulation (emergency)
- Cameron lesions with significant blood loss
- Failed medical management of reflux
Elective repair is preferred; emergency risk is lower than historically believed. Most experts advocate repair for symptomatic PEH; some advocate repair for all PEH due to complication risk.
Principles of Surgical Repair (4 Key Steps)
- Reduction of the hernia from the mediastinum/chest with excision of the hernia sac
- Reconstruction of the diaphragmatic hiatus - posterior crural closure with or without prosthetic mesh
- Fundoplication (partial or complete wrap) - prevents post-op reflux, provides bulk at hiatus
- Gastropexy or gastrostomy tube - additional fixation of the stomach intra-abdominally, reduces recurrence
Surgical Approaches
- Laparoscopic (preferred) - minimally invasive, lower morbidity
- Open upper midline laparotomy - for reoperative or complex cases where laparoscopic approach is unsafe
- Left thoracotomy - historical standard; now reserved for select complex cases
A Nissen (360°) or Toupet (270° posterior) fundoplication is typically added. If esophageal shortening is present, a Collis gastroplasty may be needed to create adequate intra-abdominal esophageal length.
- Current Surgical Therapy 14e
- Sleisenger and Fordtran's GI and Liver Disease
Complications of Untreated PEH
- Gastric volvulus (organoaxial or mesenteroaxial)
- Gastric incarceration and strangulation
- Perforation
- Obstructive symptoms (dysphagia, obstruction)
- Chronic hemorrhage (Cameron lesions)
Recent Evidence
Recent systematic reviews (2024-2025) have addressed surgical nuances:
- Ligamentum teres augmentation for hiatal repair after bariatric surgery shows favorable outcomes (PMID: 38946644)
- Transoral incisionless fundoplication + hiatal repair shows efficacy for refractory GERD with hiatal hernia (PMID: 39271515)
- Mesh vs. no mesh for recurrent hiatal hernia repair - meta-analysis 2025 comparing reinforcement strategies (PMID: 40459749)
Key clinical pearl: A type I hernia is benign in most cases - treat the GERD, not the hernia. A large type III or IV paraesophageal hernia with symptoms is a surgical lesion; delay risks catastrophic volvulus and strangulation.
This is a shared conversation. Sign in to Orris to start your own chat.