Surgical anatomy of parotid gland
Surgical Anatomy of the Parotid Gland
1. Overview
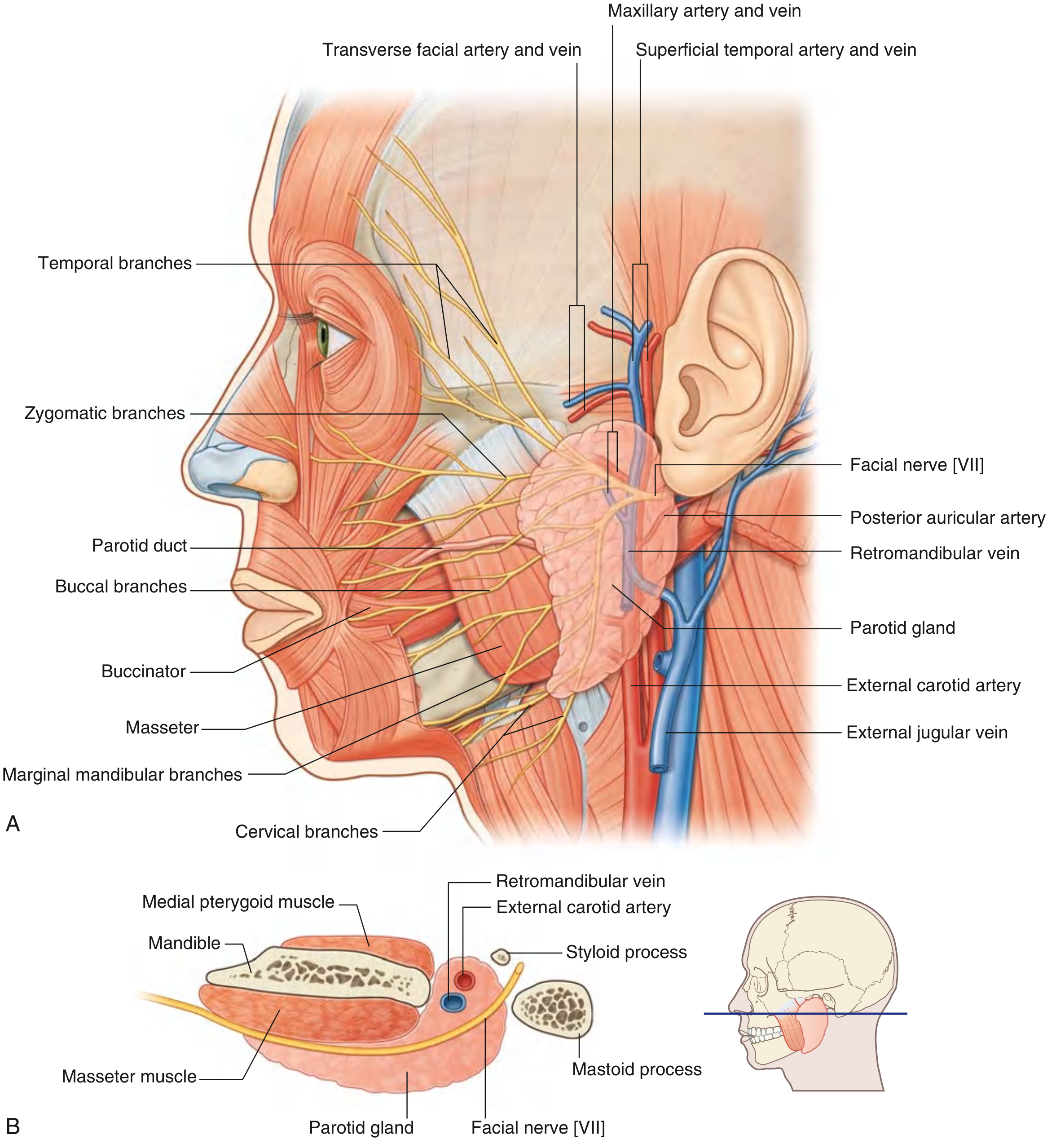
2. Location and Borders
| Border | Structure |
|---|---|
| Anterior | Masseter muscle |
| Superior | Zygomatic arch |
| Posterior | Tragal cartilage and sternocleidomastoid muscle |
| Inferior ("tail") | Between the ramus of mandible and SCM, overlying the digastric muscle |
| Deep | Prestyloid compartment of the parapharyngeal space |
- Attaches to the root of the zygoma superiorly
- Attaches firmly to the mastoid process posteriorly
- Is thicker anteriorly and inferiorly, separating the parotid from the submandibular gland
3. Lobes and the Facial Nerve Plane
- The superficial lobe accounts for approximately 80% of the parotid parenchyma and lies lateral to the facial nerve plane. It contains the majority of the intraglandular lymph nodes.
- The deep lobe is medial to the facial nerve and extends posteriorly into the prestyloid compartment of the parapharyngeal space.
- This division is primarily a surgical construct rather than a true anatomical separation, as there is no fascial plane between the two lobes.
4. Structures Passing Through the Gland
- Facial nerve (CN VII) - most superficial
- Retromandibular vein - intermediate
- External carotid artery - deepest
5. Facial Nerve (CN VII) - The Most Important Surgical Landmark
Exit from skull base
- Exits through the stylomastoid foramen, located posterolateral to the styloid process and anteromedial to the mastoid process.
Course within the gland
- Enters the posterior surface of the parotid gland.
- Divides almost immediately into the pes anserinus ("goose's foot"), forming:
- Upper (temporofacial) division
- Lower (cervicofacial) division
- These further divide within the gland into 5 terminal branches that emerge from the gland borders:
| Branch | Emergence | Muscles innervated |
|---|---|---|
| Temporal | Superior border | Frontalis, orbicularis oculi (upper) |
| Zygomatic | Anterior border | Orbicularis oculi (lower) |
| Buccal | Anterior border | Buccinator, upper lip muscles |
| Marginal mandibular | Inferior border | Lower lip and chin muscles |
| Cervical | Inferior border | Platysma |
Note: The facial nerve trunk and its divisions are more superficial in children younger than 2 years - an important surgical caveat.
Landmarks for surgical identification of the facial nerve
- Tragal pointer - the main trunk lies approximately 1 cm deep and inferior to the tip of the tragal cartilage (the most commonly used landmark)
- Tympanomastoid suture line - the nerve is found just inferior to this suture as it exits the stylomastoid foramen
- Posterior belly of the digastric muscle - marks the depth of the nerve; the nerve trunk lies just superior to where the digastric attaches to the mastoid
- Retrograde identification - tracing a known peripheral branch (e.g., the marginal mandibular) backwards to the main trunk
6. Vascular Anatomy
Arterial supply
- The external carotid artery enters the deep surface of the gland (or passes just deep to its inferior border) and terminates within the gland by dividing into:
- Maxillary artery - passes horizontally deep to the mandible
- Superficial temporal artery - emerges from the upper border after giving off the transverse facial artery
- The posterior auricular artery also arises before the terminal division.
- The external carotid is often encountered only during total parotidectomy.
Venous drainage
- The maxillary vein and superficial temporal vein unite within the gland to form the retromandibular vein.
- The retromandibular vein divides into:
- An anterior division - joins the facial vein and drains into the internal jugular vein (lies just deep to the marginal mandibularis branch of CN VII)
- A posterior division - joins the posterior auricular vein to form the external jugular vein
7. Parotid Duct (Stensen's Duct)
- Arises from the anterior border of the gland, midway between the zygomatic arch and the corner of the mouth.
- Runs horizontally across the masseter muscle (approximately a finger's breadth below the zygomatic arch).
- At the anterior border of masseter, it turns sharply medially, pierces the buccal fat pad and then the buccinator muscle.
- Opens into the oral cavity at a small papilla on the buccal mucosa opposite the upper second molar tooth.
- The duct and the buccal space are examined by bimanual palpation.
- An accessory parotid gland (present in ~21% of individuals) lies along the duct over the masseter and accounts for ~1% of parotid tumours.
8. Nerve Supply (Autonomic)
| Type | Pathway |
|---|---|
| Parasympathetic (secretomotor) | CN IX (Glossopharyngeal) → tympanic branch → lesser petrosal nerve → otic ganglion → auriculotemporal nerve (branch of V3) → parotid gland |
| Sympathetic | Superior cervical ganglion → plexus on external carotid artery |
9. Relations to the Parapharyngeal Space
- Base: Petrous bone of skull base
- Medial: Lateral pharyngeal wall
- Lateral: Medial pterygoid muscle
- Posterior: Carotid sheath and vertebral bodies
- Anterior: Pterygomandibular raphe
10. Surgical Significance and Complications of Parotidectomy
| Complication | Anatomical Basis |
|---|---|
| Facial nerve palsy | CN VII traverses the gland; temporary neuropraxia common, permanent palsy ~1-2% |
| Frey's syndrome (gustatory sweating) | Auriculotemporal nerve fibres regenerate aberrantly to skin sweat glands |
| Greater auricular nerve sensory loss | C2-C3 nerve crosses the surgical field; unavoidable in most cases; posterior branch can sometimes be preserved |
| Cosmetic hollow | Loss of gland bulk behind the mandibular ramus; can be mitigated with fat transfer |
| Salivary fistula / sialocele | Residual parotid tissue or duct leakage |
Extracapsular parotidrctomy
extracapsular dissection parotid pleomorphic adenoma
PMID: 40843726
Extracapsular Dissection (ECD) of the Parotid Gland
1. Definition and Concept
ECD → Adequate Parotidectomy → Superficial Parotidectomy → Total Conservative Parotidectomy → Radical Parotidectomy
2. Rationale and Historical Context
3. Patient Selection (Indications)
| Criterion | Requirement |
|---|---|
| Histology (presumed) | Benign tumour (typically pleomorphic adenoma or Warthin's tumour) |
| Size | Up to approximately 3 cm |
| Location | Superficial lobe of the parotid (lateral to the facial nerve plane) |
| Mobility | Fully mobile on examination (not tethered to deeper structures) |
| Facial nerve | Clinically intact CN VII function pre-operatively |
| Imaging | No evidence of deep lobe extension, malignant features, or lymphadenopathy |
| Surgeon | Expert hands only - not recommended for inexperienced parotid surgeons |
A 2025 meta-analysis (2507 patients, 21 studies) concluded: "ECD could be considered the treatment of choice for pleomorphic adenomas up to 3 cm in size, mobile and located in the superficial lobe of the parotid gland." - Salzano et al., 2025 (PMID: 40843726)
4. Contraindications
- Large tumours (>3 cm)
- Deep lobe location or parapharyngeal extension
- Malignant tumour (proven or strongly suspected)
- Recurrent pleomorphic adenoma
- Pre-operative facial nerve weakness
- Fixation to skin or deep structures
- Lymphadenopathy
- Tumour adjacent to or abutting the facial nerve
5. Surgical Technique
Incision
- Blair incision - straight preauricular incision curving below the earlobe
- Modified "lazy S" incision - three components: vertical component near the tragus, gentle curve, and horizontal component along neck skin crease (2 finger-breadths below the angle of the mandible). This is the modern preferred approach.
- Facelift (rhytidectomy) incision - for optimal cosmesis
Flap elevation
- The subcutaneous flap is raised above the platysma (same plane as for parotidectomy).
- The great auricular nerve is identified and the posterior branch preserved where possible.
Tumour exposure and dissection
- The parotidomasseteric fascia is incised in a cruciate or curvilinear manner directly over the tumour.
- The tumour is identified and dissection proceeds in a plane immediately outside the tumour capsule.
- A thin cuff of normal parotid parenchyma is taken around the tumour.
- The facial nerve branches are visualised but not formally skeletonised - the surgeon works around them rather than dissecting them free.
- Intraoperative nerve monitoring (IONM) is strongly recommended to make this safer. In the absence of monitoring, extreme caution and a high index of suspicion before dividing any structure are mandatory.
Closure
- The parotid fascia is closed with absorbable sutures.
- A suction drain is placed beneath the posterior belly of digastric and brought out posterior to the suture line.
- Sternocleidomastoid muscle flap or acellular dermal matrix may be placed over the parotid bed to reduce Frey's syndrome risk.
- Skin closed in layers.
6. Arguments For and Against ECD
| Arguments FOR ECD | Arguments FOR Partial/Superficial Parotidectomy |
|---|---|
| Recurrence rates equivalent to superficial parotidectomy | Tumour capsule is histologically incomplete; tumour cells may extend through capsule - a tissue cuff improves microscopic clearance |
| Less cosmetic deformity (more tissue preserved) | If unexpected malignancy found, partial clearance may still be adequate for low-grade tumours |
| Lower incidence of Frey's syndrome | |
| In most cases, no cuff is possible adjacent to the facial nerve branch anyway | Dissecting close on the capsule risks rupture (though this typically happens at the nerve interface where no cuff was possible anyway) |
| If revision surgery required (e.g., malignancy on final histology), the tissue planes for main nerve identification remain virginal |
7. Outcomes - Evidence Summary
Recurrence
- Recurrence rates after ECD are equivalent to those after superficial parotidectomy.
- Overall pleomorphic adenoma recurrence (any technique) is ~2%, typically occurring ~10 years after surgery; some series report 6.7% at 20 years.
- Recurrence is usually multifocal and may result from intraoperative capsule rupture/tumour spillage.
Facial nerve
- Transient facial nerve palsy: Significantly lower with ECD compared to superficial parotidectomy (p < 0.05).
- Permanent facial nerve palsy: Similar rates between ECD and superficial parotidectomy.
- This is because formal nerve skeletonisation is avoided, reducing traction and thermal injury.
Frey's syndrome
- Significantly lower with ECD than with superficial parotidectomy (p < 0.05), because less parotid tissue and fewer auriculotemporal nerve fibres are disrupted.
Other complications
- Salivary fistula, seroma, and haematoma rates are comparable between the two approaches.
2025 Meta-analysis (Salzano et al., 21 studies, 2507 patients): ECD shows lower transient facial palsy, lower Frey's syndrome, and equivalent recurrence vs. superficial parotidectomy for tumours ≤3 cm. PMID: 40843726
8. Important Caveats and Failures
- Capsule rupture during ECD is a known risk and historically associated with increased recurrence - though modern data suggests this association is weaker than previously believed. The rupture most commonly occurs where the tumour abuts a facial nerve branch (exactly where a tissue cuff is anatomically impossible anyway).
- Unexpected malignancy on final histology is a problem, as no formal nerve dissection was performed. However, the advantage here is that the facial nerve planes remain undisturbed, making re-operation easier.
- Enucleation (removing the tumour through its own capsule without any surrounding tissue) is specifically condemned - it results in an unacceptably high recurrence rate and should not be done.
9. ECD for Deep Lobe Tumours
Summary
| Feature | ECD | Superficial Parotidectomy |
|---|---|---|
| Facial nerve formally identified | No | Yes |
| Tumour boundary | Just outside capsule | With cuff of normal parenchyma |
| Recurrence | Equivalent | Equivalent |
| Transient facial palsy | Lower | Higher |
| Permanent facial palsy | Similar | Similar |
| Frey's syndrome | Lower | Higher |
| Tissue preservation | Greater | Less |
| Plane available for revision | Virginal | Scarred |
| Suitable for | Small, mobile, superficial, benign | Most superficial lobe tumours |
Briefly describe Classification of salivary gland tumors. Write management of mucoepidermoid carcinoma of parotid gland. [3+7]
Part 1 [3 marks]: Classification of Salivary Gland Tumours
WHO Classification (2017 - 4th Edition)
A. Epithelial Tumours (>80% of all salivary gland tumours)
| Tumour | Notes |
|---|---|
| Pleomorphic adenoma | Most common salivary gland tumour overall |
| Myoepithelioma | |
| Basal cell adenoma | |
| Warthin's tumour (Cystadenolymphoma) | Almost exclusively in parotid |
| Oncocytoma | |
| Lymphadenoma | |
| Cystadenoma | |
| Sialadenoma papilliferum | |
| Ductal papillomas | |
| Sebaceous adenoma | |
| Canalicular adenoma | Mainly minor glands |
| Tumour | |
|---|---|
| Mucoepidermoid carcinoma | Most common salivary gland malignancy |
| Adenoid cystic carcinoma | |
| Acinic cell carcinoma | |
| Polymorphous adenocarcinoma | |
| Epithelial-myoepithelial carcinoma | |
| Carcinoma ex pleomorphic adenoma | |
| Secretory carcinoma (formerly mammary analogue secretory ca.) | |
| Salivary duct carcinoma | |
| Adenocarcinoma NOS | |
| Basal cell adenocarcinoma | |
| Myoepithelial carcinoma | |
| Sebaceous adenocarcinoma | |
| Lymphoepithelial carcinoma | |
| Intraductal carcinoma | |
| Oncocytic carcinoma | |
| Sialoblastoma (borderline) |
The 2017 WHO classification updated the nomenclature by removing grade from tumour names (e.g., polymorphous low-grade adenocarcinoma became simply polymorphous adenocarcinoma) and reclassified sialoblastoma as a borderline tumour. The number of WHO-recognised malignant epithelial entities has increased greatly over the past 50 years and now stands at 22. - Cummings Otolaryngology
B. Mesenchymal (Soft Tissue) Tumours (<20%)
C. Haematolymphoid Tumours
Part 2 [7 marks]: Management of Mucoepidermoid Carcinoma of the Parotid Gland
Background
Grading - The Cornerstone of Management
| Histological Feature | Points (Auclair) |
|---|---|
| Cystic component <20% | +2 |
| Neural invasion | +2 |
| ≥4 mitoses/10 hpf | +3 |
| Necrosis | +3 |
| Anaplasia | +4 |
| Grade | Score | Histology | Behaviour |
|---|---|---|---|
| Low (Grade 1) | 0-4 | Predominantly cystic, well-circumscribed, mucous cells predominate, minimal atypia | Rarely metastasises; very good prognosis |
| Intermediate (Grade 2) | 5-6 | Less circumscribed, more solid, intermediate cell predominance | Variable; challenging to manage |
| High (Grade 3) | ≥7 | Solid, infiltrative, nuclear atypia, mitoses, necrosis, perineural invasion, lymphovascular emboli; focal mucin essential for diagnosis | Locally aggressive; bone/skin involvement; nodal and distant metastases (mainly lungs) |
Pre-operative Assessment
- FNAC - confirms malignancy in most cases; shows mixture of glandular and squamoid cells
- MRI - superior to CT for evaluating extent, facial nerve involvement, perineural spread, retromandibular parotid, and parapharyngeal extension
- CT neck/chest - staging, nodal assessment, distant metastases (lung)
- Facial nerve function - clinical evaluation mandatory
- MDT discussion - all parotid malignancies should be discussed at a Head and Neck Cancer MDT
Surgical Management (Primary Treatment)
1. Extent of Parotidectomy
| Tumour | Operation |
|---|---|
| Superficial lobe, no nerve involvement | Superficial parotidectomy with wide margins |
| Deep lobe involvement or large tumour | Total conservative parotidectomy (facial nerve preserved) |
| Facial nerve directly invaded | Radical parotidectomy with nerve sacrifice |
- Complete surgical excision with wide margins is advocated for all grades of MEC. - Bailey and Love's
- The surgical principle is negative margins - positive margins are strongly associated with recurrence and are an indication for adjuvant radiotherapy.
2. Facial Nerve Management
| Situation | Decision |
|---|---|
| Nerve not invaded, functioning pre-operatively | Preserve in all cases |
| Pre-operative facial nerve palsy | Nerve very likely invaded - may require sacrifice |
| Nerve directly invaded at surgery | Sacrifice and plan immediate cable graft reconstruction |
| Nerve encased by tumour | Sacrifice and reconstruct |
3. Neck Dissection
| Situation | Decision |
|---|---|
| Clinically/radiologically node-positive (cN+) | Therapeutic neck dissection (selective levels I-IV, or comprehensive as needed) + post-operative radiotherapy |
| Clinically node-negative (cN0), high-grade MEC | Elective neck dissection - occult metastasis rate justifies elective treatment |
| Clinically node-negative (cN0), low-grade MEC | Elective neck dissection not routinely required - occult metastasis rate too low to justify surgery |
| pN+ disease | Post-operative radiotherapy improves locoregional control |
Adjuvant Radiotherapy
- Post-operative radiotherapy is the treatment of choice for intermediate- and high-grade MEC following surgery. - Bailey and Love's
- Indications for post-operative radiotherapy:
- High-grade tumour
- Intermediate-grade tumour
- Positive or close surgical margins
- Perineural invasion
- Lymphovascular invasion
- Node-positive disease (pN+)
- Advanced T stage (T3/T4)
- Facial nerve sacrifice
- Low-grade MEC confined to the parotid with clear margins and no adverse features: surgery alone may be adequate, with careful surveillance.
- Dose typically 60-66 Gy to the primary site (higher doses with positive margins).
Chemotherapy
- No established role as primary or standard adjuvant treatment.
- Used for unresectable, recurrent, or metastatic disease - typically platinum-based regimens.
- Concurrent chemoradiotherapy may be considered in high-risk, unresectable cases.
Prognosis
| Grade | 5-year survival | Key risk |
|---|---|---|
| Low | >90% | Minimal |
| Intermediate | Variable (~70-80%) | Unpredictable behaviour |
| High | ~40-50% | Local recurrence, regional and distant metastases |
- The CRTC1-MAML2 translocation t(11;19)(q21;p13), found in >50% of MECs, is associated with better prognosis and is useful for confirming diagnosis (especially in low/intermediate grade). High-grade MEC is typically negative for this translocation.
- Submandibular MEC has a higher recurrence and metastasis rate than parotid MEC of the same grade - warranting aggressive resection of any submandibular primary.
Summary: Management at a Glance
Low-grade parotid MEC:
→ Superficial/total conservative parotidectomy + nerve preservation
→ Elective neck dissection: NOT routinely required
→ Adjuvant RT: Only if margins positive
Intermediate/High-grade parotid MEC:
→ Total conservative parotidectomy (± nerve sacrifice if involved)
→ Elective neck dissection (cN0) OR therapeutic neck dissection (cN+)
→ Post-operative radiotherapy: MANDATORY
→ Reconstruction: nerve cable graft if CN VII sacrificed
Describe intra-operative methods of identification of Facial nerve. [5]
Intra-operative Methods of Identification of the Facial Nerve
Approach 1: Antegrade (Anterograde) Identification - Standard Method
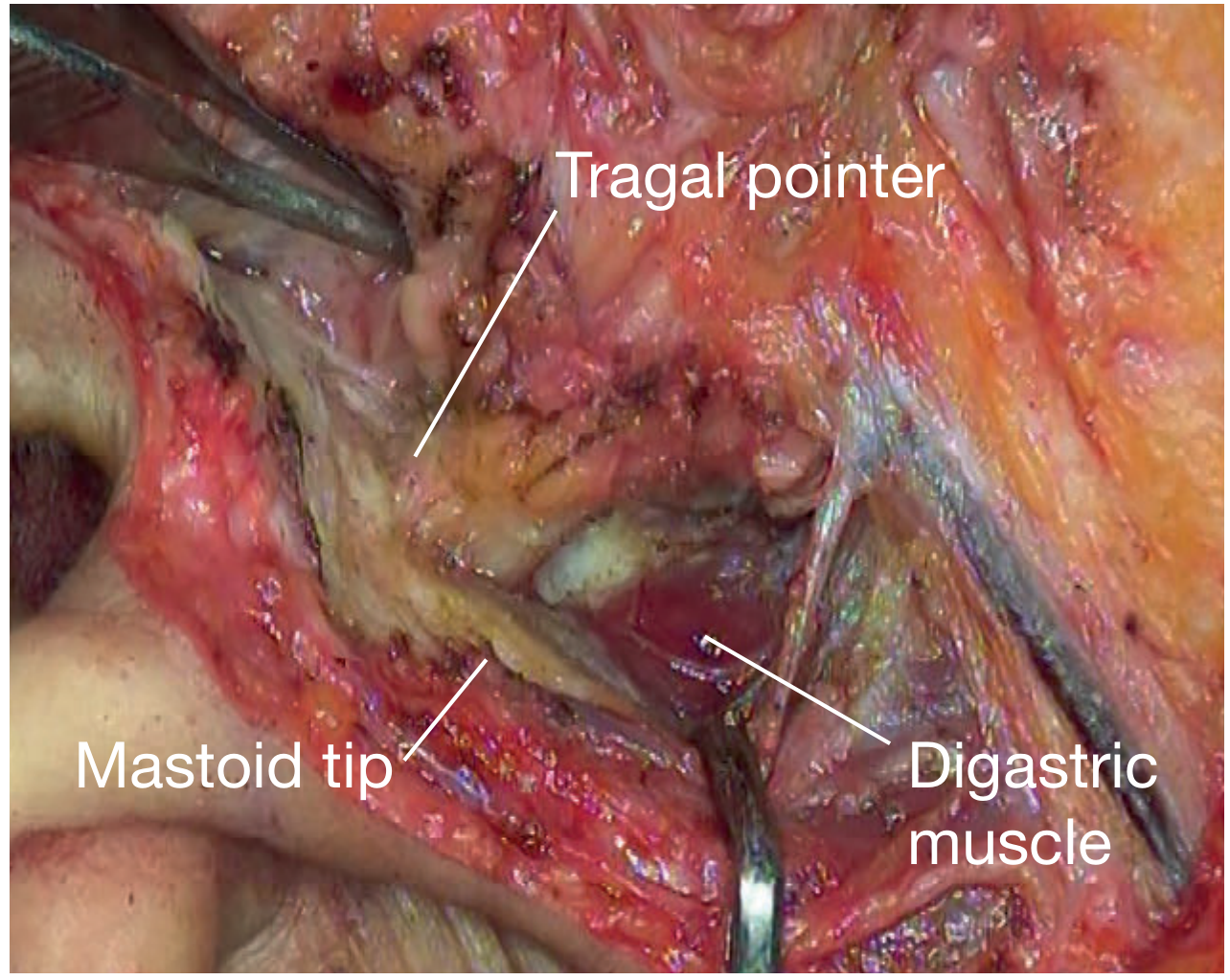
Landmark 1: Tragal Pointer (Conley's Pointer) - Most Commonly Used
- The tragal pointer is the pointed inferior tip of the cartilaginous external auditory canal, exposed by mobilising the parotid gland anteriorly off the tragal cartilage.
- The facial nerve main trunk lies 1 to 1.5 cm deep and inferior to the tip of the tragal pointer.
- It is the most frequently used intraoperative landmark. - Cummings Otolaryngology
- Caveat: The tragal pointer is slightly mobile when retracted, so care must be taken. In children under 2 years, the nerve trunk is more superficial than in adults.
Landmark 2: Tympanomastoid Suture Line - Most Reliable
- The tympanomastoid suture is the bony groove between the tympanic plate and the mastoid process, palpable as a groove with a finger or instrument after the parotid gland is retracted anteriorly.
- The facial nerve lies immediately deep and inferior to this suture line at its point of exit from the skull base, approximately 6-8 mm deep to it.
- Described as "extremely reliable" - the surgeon can literally feel where the nerve will be by following the suture medially. - Scott-Brown's Otorhinolaryngology
- The tympanomastoid suture and tragal pointer together define the most consistent zone for finding the main trunk.
Landmark 3: Posterior Belly of the Digastric Muscle
- The posterior belly of the digastric muscle is identified by dissecting the parotid off the SCM and tracing the muscle to its attachment at the mastoid process.
- The facial nerve leaves the skull immediately anterior to the digastric's attachment to the mastoid, and lies just above the upper border of the posterior belly.
- This landmark also marks the depth at which the nerve is expected to be found - the nerve trunk lies at the same tissue plane as the digastric.
- The nerve is exposed by careful dissection in the area immediately anterior to the posterior belly, in the region of the mastoid process.
Summary of antegrade landmarks:
Landmark Nerve relation Tragal pointer 1-1.5 cm deep and inferior to its tip Tympanomastoid suture Immediately deep and inferior; 6-8 mm deep Posterior belly of digastric Immediately anterior to its mastoid attachment; above its upper border
Approach 2: Retrograde (Peripheral Branch) Identification
- Large or soft tumours directly overlying the main trunk
- Revision surgery (scarred tissue planes)
- Recurrent pleomorphic adenoma
| Branch | How to find it |
|---|---|
| Marginal mandibular branch | Most commonly used; found below the lower border of the mandible, lying superficial to the facial artery and vein at the angle of the mandible, beneath the deep cervical fascia |
| Cervical branch | Found where it pierces the deep fascia below the body of the mandible |
| Zygomatic/temporal branches | Cross the zygomatic arch anterior to, and within 1-2 cm of, the superficial temporal artery |
Approach 3: Intraoperative Nerve Monitoring (IONM)
- Electromyographic (EMG) nerve monitoring involves placing needle electrodes in the facial muscles (orbicularis oculi, orbicularis oris, mentalis) and connecting to a monitor that produces an audible or visual signal when the probe stimulates the facial nerve.
- A handheld probe is used to electrically stimulate tissue during dissection; a response confirms that neural tissue is nearby before cutting.
- Functions:
- Confirms identity of the nerve intraoperatively
- Provides early warning before mechanical trauma
- Allows real-time assessment of nerve function throughout dissection
- Especially valuable in revision surgery and malignant cases
- Limitations: Does not by itself prevent nerve injury if the surgeon disregards the signal; cannot detect crush injury occurring progressively.
- There is no definitive evidence that routine IONM reduces permanent facial palsy rates in standard cases. However, most surgeons advocate its use in difficult or revision cases, and familiarity with it through routine use is arguably the strongest justification for employing it universally. - Scott-Brown's Otorhinolaryngology
Summary
| Method | Landmark / Technique | Nerve Relation |
|---|---|---|
| Tragal pointer (Conley's) | Tip of tragal cartilage | 1-1.5 cm deep and inferior |
| Tympanomastoid suture | Bony groove: tympanic plate + mastoid | 6-8 mm deep and inferior |
| Posterior belly of digastric | Mastoid attachment | Immediately anterior + above upper border |
| Retrograde dissection | Peripheral branch traced proximally | Marginal mandibular, cervical, or zygomatic branches |
| Nerve monitoring (IONM) | EMG stimulation probe | Audible/visual signal on stimulation |
Describe the clinical features and management of submandibular salivary gland calculus disease. [2+3]
Submandibular Salivary Gland Calculus Disease (Sialolithiasis)
Part 1 [2 marks]: Clinical Features
Why the Submandibular Gland Is Most Affected
| Factor | Explanation |
|---|---|
| Long, tortuous duct | Wharton's duct (5 cm) is longer and more angulated than other ducts |
| Uphill / antigravity course | The duct ascends around the posterior border of the mylohyoid against gravity, slowing flow |
| More viscous saliva | Mixed seromucinous secretion is stickier than pure serous saliva |
| Higher calcium content | Saliva has a higher calcium and phosphate concentration |
| Alkaline pH | Alkaline saliva promotes calcium phosphate precipitation |
Symptoms
-
Salivary colic - Recurrent episodes of pain in the submandibular region, typically precipitated by eating (meal-time syndrome), as gustatory stimulation increases saliva production against the obstruction.
-
Postprandial swelling - Cyclical, recurrent enlargement of the submandibular gland that comes on during or after meals and gradually subsides as saliva drains partially. This is the most characteristic symptom.
-
Dry mouth / reduced salivation - Due to decreased salivary flow from the obstructed gland.
-
Foul-tasting fluid - Mucopurulent saliva may be expressible on massaging the gland, pointing to secondary infection.
-
Secondary acute sialadenitis - Salivary stasis encourages retrograde bacterial migration, resulting in acute suppurative infection: more severe pain, persistent swelling (not relieved after meals), erythema, fever, and trismus.
-
Abscess formation - A submandibular or sublingual space abscess if infection progresses.
Signs
- Asymmetric enlargement of the submandibular gland on inspection.
- Bimanual palpation (one finger intraoral along the floor of mouth, other hand below the mandible): a proximal stone may be palpable as a hard, gritty lump along the course of Wharton's duct.
- Reduced or absent salivary flow from the ipsilateral duct orifice (at the sublingual papilla beside the frenulum) on massage of the gland.
- Mucoid, particulate, or mucopurulent saliva expressed from the duct orifice.
- A stone may occasionally be visible at or near the duct orifice in the floor of the mouth.
- In infection: floor of mouth induration, tenderness, erythema, cervical lymphadenopathy.
Part 2 [3 marks]: Management
Investigations
| Investigation | Role |
|---|---|
| Ultrasound | First-line; detects >90% of stones >2 mm; non-invasive |
| Plain X-ray (occlusal view) | Initial test; 80% of submandibular stones are radio-opaque; however misses radiolucent stones |
| CT scan | Superior sensitivity; detects all radiopaque stones; also shows gland enlargement and ductal dilatation; used if diagnosis unclear or neoplasm suspected |
| MR sialography | Non-invasive; uses saliva as contrast; accuracy similar to digital sialography; preferred when sialography is contraindicated |
| Sialography | Gold standard (historical); contrast injected into duct; identifies duct pathology and radiolucent stones (sensitivity 95-100%); contraindicated in acute infection and stones at the duct orifice |
| Sialendoscopy | Diagnostic AND therapeutic; direct visualisation of duct and stone |
Management Algorithm
Step 1: Conservative (Non-surgical) Measures - Always First
- Sialagogues - lemon juice, sour sweets, vitamin C - stimulate salivary flow to flush the stone
- Hydration - adequate fluid intake reduces salivary viscosity
- Local heat / massage of the gland toward the duct orifice
- Analgesics - for pain relief
- Antibiotics - if secondary infection (acute sialadenitis) is present; typically amoxicillin-clavulanate or co-amoxiclav
- Small distal stones may be spontaneously expelled with these measures
Step 2: Minimally Invasive Removal
- For palpable stones in the distal duct, no more than 2 cm from the duct orifice, distal to the posterior edge of the mylohyoid muscle.
- The stone can be milked manually through the orifice, or a transoral incision is made directly over the stone under local anaesthesia to extract it.
- Simple, effective, preserves the gland.
- The duct is incised along its floor over the stone, and the stone removed.
- Suitable for distal impacted stones.
- Direct endoscopic visualisation and stone removal through the natural duct orifice.
- Safe, performed under local anaesthesia, with better outcomes than open surgery in experienced hands. - Bailey and Love's
- Guidelines by stone size:
| Stone size | Approach |
|---|---|
| <5 mm (distal) | Endoscopic basket retrieval alone |
| >5 mm (distal) | Combined: endoscopy + transoral duct slitting |
| 5-7 mm (intraparenchymal) | Endoscopic extraction |
| >7 mm (intraparenchymal) | Transoral slitting or gland excision |
| Hilar stones | Endoscopic approach |
- Used for stones not palpable and not visible endoscopically.
- Fragments the stone, allowing spontaneous passage.
- Not suitable for stones larger than 7-10 mm.
- Multiple sessions may be required. - Bailey and Love's
Step 3: Surgical Gland Excision - Last Resort
- Failed conservative and endoscopic management
- Large, proximal, hilar, or intraglandular stones not amenable to minimally invasive approaches
- Chronic, recurrent sialadenitis with gland fibrosis and irreversible damage (non-functioning gland)
- Suspected malignancy
"Excision of the submandibular gland should be considered as a last resort." - Bailey and Love's Short Practice of Surgery
Summary of Management
Acute infection present?
→ YES: Antibiotics + hydration first; defer stone removal
→ NO: Proceed to stone removal
Stone location:
Distal (anterior to mylohyoid) → Conservative / transoral removal / duct slitting
Mid-duct / mobile → Sialendoscopy ± ESWL
Proximal / hilar / large → Sialendoscopy + transoral combined approach
Intraglandular / failed all → Submandibular gland excision (last resort)
Breast lump case presentation how to do it
How to Present a Breast Lump Case
Opening Statement (Set the Scene)
"Mrs X is a [age]-year-old [occupation] who presents with a [duration]-month history of a lump in the [right/left] breast, first noticed [how it was noticed], associated with [key associated features]."
- Age (critical - younger = likely benign; older = malignant until proven otherwise)
- Side and duration
- Whether symptomatic or incidentally found
1. History of Presenting Complaint (HPC)
About the Lump - SOCRATES adapted
| Feature | Questions to ask / present |
|---|---|
| Site | Which breast? Which quadrant? (UOQ = most common; retroareolar, axillary tail) |
| Onset | When first noticed? How discovered - self, partner, screening? |
| Character | Hard/soft? Smooth/irregular? Single/multiple? |
| Radiation | Is there associated axillary swelling? |
| Associated symptoms | See below |
| Timing | Constant or cyclical? Does it change with menstrual cycle? (cyclical = benign) |
| Exacerbating/relieving | Any change with posture, pressure, lactation? |
| Size progression | Growing rapidly (malignant) or stable (benign)? |
Associated Symptoms - ask specifically about each
- Pain - mastalgia: cyclical (benign fibrocystic) vs non-cyclical (may be malignant)
- Nipple discharge - most important associated symptom:
- Colour: clear, milky, serous, blood-stained (blood-stained = malignant until proven otherwise - carcinoma, duct papilloma)
- Laterality: unilateral (suspicious) vs bilateral (hormonal)
- Spontaneous vs expressed
- Nipple changes: inversion (recent-onset = malignant), eczema/scaling of nipple (Paget's disease of breast = carcinoma of underlying duct)
- Skin changes: redness, dimpling, peau d'orange (cutaneous lymphatic oedema = malignant), ulceration
- Bone pain (spinal, hip - bone metastases)
- Shortness of breath / dry cough (lung/pleural metastases)
- Weight loss, anorexia, fatigue (metastatic disease)
- Jaundice, right upper quadrant pain (liver metastases)
- Headache, neurological symptoms (brain metastases)
2. Past Medical History (PMH)
- Previous breast lumps, biopsies, or operations
- Previous breast cancer (ipsilateral recurrence or contralateral)
- Previous chest wall radiation (risk factor for breast cancer)
- Benign breast disease (fibrocystic change, fibroadenoma)
- Any other malignancy
3. Drug History
- Oral contraceptive pill (OCP) - slight increased risk of breast cancer
- Hormone replacement therapy (HRT) - significant risk factor, especially combined oestrogen-progesterone
- Antipsychotics / metoclopramide / domperidone - cause hyperprolactinaemia → galactorrhoea
- Any anticoagulants (relevant before biopsy)
4. Menstrual and Obstetric History (CRITICAL for breast)
| Feature | Significance |
|---|---|
| Age at menarche | Early menarche (<12 yrs) = increased risk |
| Menstrual cycle - regular? | Cyclical symptoms = benign |
| Age at menopause | Late menopause (>55 yrs) = increased risk |
| Parity | Nulliparity = increased risk |
| Age at first full-term pregnancy | Late first pregnancy (>30 yrs) = increased risk |
| Breastfeeding | Protective against breast cancer |
| Pregnancy - current? | Relevant (physiological breast changes) |
5. Family History (CRITICAL)
- Breast or ovarian cancer in first-degree relatives (mother, sister, daughter)
- Bilateral breast cancer or young age at diagnosis in relatives (<40 yrs) - suggests BRCA1/BRCA2 mutation
- Male breast cancer in the family (BRCA2)
- Number of relatives affected and degree of relation
- Any known BRCA mutation in family
6. Social History
- Smoking (modest risk increase)
- Alcohol consumption (dose-dependent risk increase)
- Occupation
- BMI / obesity (post-menopausal risk)
- Anxiety about diagnosis; patient's concerns
7. Examination Findings - How to Present
General inspection
"On general inspection, the patient was comfortable at rest / in mild discomfort. She was [BMI]. There was no jaundice, pallor, or lymphadenopathy visible."
Breast Inspection - done in 3 positions:
- Arms by the side (resting)
- Arms raised above head (tethers skin/ligaments of Cooper)
- Hands pressed on hips (contracts pectoralis - reveals deep fixity)
- Leaning forward (pendulous breasts - reveals asymmetry)
| Sign | Significance |
|---|---|
| Asymmetry - size, shape, level | Any new asymmetry is suspicious |
| Skin changes: redness, erythema | Infection / inflammatory carcinoma |
| Peau d'orange (skin like orange peel) | Cutaneous lymphatic obstruction = malignancy |
| Skin dimpling / tethering | Involvement of Cooper's ligaments = malignancy |
| Skin ulceration | Advanced malignancy |
| Nipple inversion - recent onset | Subareolar carcinoma tethering the duct |
| Nipple retraction - longstanding, slit-like | Usually benign (periductal mastitis) |
| Paget's disease - eczema/scaling of nipple | Underlying ductal carcinoma in-situ |
| Prominent veins | Rapidly growing tumour / Paget's |
| Visible lump | Size, quadrant |
Example: "On inspection, both breasts were symmetrical at rest. On raising the arms, there was a visible skin dimple in the upper outer quadrant of the right breast. There was no peau d'orange, nipple inversion, or skin ulceration."
Breast Palpation
| Feature | Benign | Malignant |
|---|---|---|
| Site | State quadrant (e.g., UOQ 2 cm from areola) | |
| Size | Measure in 2 dimensions (e.g., 2 x 3 cm) | |
| Shape | Smooth, regular (benign) | Irregular (malignant) |
| Surface | Smooth | Nodular, irregular |
| Consistency | Soft, firm, rubbery (benign); tense-cystic | Hard, stony (malignant) |
| Edge/margin | Well-defined, distinct (benign) | Ill-defined, indistinct (malignant) |
| Mobility | Mobile in all directions (benign - fibroadenoma "breast mouse") | Fixed to skin or pectoralis (malignant) |
| Skin tethering | Absent | Present: dimple moves with lump on arm raising |
| Muscle fixation | Not fixed to pectoralis | Fixed: lump moves less with pectoralis contracted (hands on hips) |
| Tenderness | Tender (benign, abscess, cyst) | Usually non-tender |
| Temperature | Warm (inflammatory) | Not warm (unless inflammatory ca.) |
Example: "On palpation in the right UOQ, there was a 3 x 2 cm firm, irregular, ill-defined lump with a nodular surface. It was non-tender. There was skin tethering overlying the lump, confirmed by a dimple on raising the arms. The lump was slightly fixed to the pectoralis major on pressing the hands on the hips. Nipple discharge was not expressible."
Axillary Examination
"Axillary examination revealed / did not reveal palpable lymphadenopathy. [If present]: There were [number] palpable lymph nodes in the [level/group], measuring approximately [size], which were [firm/hard/matted/mobile/fixed]."
Other nodes
- Supraclavicular nodes (level IV+ spread; Virchow's node - left)
- Infraclavicular nodes
- Contralateral axilla
Systemic examination
- Liver - hepatomegaly (metastases)
- Spine - tenderness (bone metastases)
- Chest - reduced air entry, dullness (pleural effusion from metastases)
- Neurological - if any neurological symptoms
8. Summary and Differential Diagnosis
"In summary, this is a [age]-year-old woman presenting with a [duration] history of a hard, irregular, ill-defined [size] lump in the [right UOQ] with overlying skin tethering and ipsilateral level I axillary lymphadenopathy. Given these features, my primary differential diagnosis is [breast carcinoma]. My other differentials include [fibroadenoma / cyst / fat necrosis / phyllodes tumour / abscess]."
9. Investigations - Triple Assessment
"I would investigate this patient using the Triple Assessment framework." - Bailey and Love's Short Practice of Surgery
| Arm | Investigation | Details |
|---|---|---|
| 1. Clinical | History + Examination | As above |
| 2. Imaging | USS (<35 yrs, dense breasts) | Cystic vs solid; BI-RADS scoring |
| Mammogram (>35-40 yrs) | CC and oblique views; microcalcifications = DCIS | |
| MRI breast | Pre-op staging, lobular ca., implants, BRCA carriers | |
| USS axilla | If cancer suspected - assess nodes | |
| 3. Pathology | Core needle biopsy (CNB) | Gold standard - histology, receptor status (ER, PR, HER2) |
| Fine needle aspiration cytology (FNAC) | Rapid; cytology only | |
| Trucut / vacuum-assisted biopsy | Larger cores; for microcalcifications |
The positive predictive value of triple assessment approaches 100% when all three arms are concordant. - Bailey and Love's
10. Benign vs Malignant: The Key Differentiating Table
| Feature | Benign | Malignant |
|---|---|---|
| Age | Young (<35 yrs) | Older (>40 yrs) |
| Pain | Often painful | Usually painless |
| Shape | Regular, smooth | Irregular, nodular |
| Edge | Well-defined | Ill-defined |
| Consistency | Soft/firm/rubbery | Hard, stony |
| Mobility | Mobile ("breast mouse") | Fixed to skin/muscle |
| Skin changes | Absent | Tethering, peau d'orange, ulceration |
| Nipple | Normal | Inversion (recent), Paget's |
| Discharge | Clear/milky | Blood-stained |
| Axilla | No lymphadenopathy | Hard, matted nodes |
| Growth | Slow / cyclical | Progressive |
Model Case Presentation (Example)
"Mrs A is a 52-year-old postmenopausal teacher who presents with a 3-month history of a painless lump in her right breast, noticed incidentally on self-examination. The lump has progressively increased in size. She has no nipple discharge but noticed the skin over the lump appears dimpled. She has no systemic symptoms. She has been on HRT for 5 years. Her mother was diagnosed with breast cancer at 62. Her menarche was at age 11 and menopause at 53. She is nulliparous.On examination she is comfortable at rest. Breast inspection reveals a visible asymmetry in the right UOQ. On raising the arms, a skin dimple is apparent in the right UOQ. On palpation, there is a hard, 3 x 2 cm, irregular, ill-defined, non-tender lump in the right UOQ at the 10 o'clock position, approximately 3 cm from the nipple. The lump shows overlying skin tethering and is slightly restricted in mobility on contracting the pectoralis major. No nipple discharge is expressible. There are two palpable, firm, 1 cm lymph nodes in the right axilla at level I. No supraclavicular or contralateral lymphadenopathy.My primary differential is carcinoma of the right breast (T2 N1 Mx). I would investigate with Triple Assessment: ultrasound and mammogram of the right breast, ultrasound-guided core needle biopsy of the lump, and USS-guided FNA of the axillary nodes. Further staging with CT chest/abdomen/pelvis and bone scan as appropriate."
Complication of superficial parotidectomy
Complications of Superficial Parotidectomy
A. Specific Complications
1. Facial Nerve Palsy - The Most Important Complication
Temporary (Neuropraxia) - Common
- Occurs due to traction, retraction, thermal injury, or oedema around the nerve during dissection, without structural nerve damage.
- The marginal mandibular branch is the most commonly affected (lower lip weakness, drooling).
- Recovery: Neuropraxia usually resolves within 4-6 weeks.
- More severe injury (axonotmesis) causes degeneration and recovery may take 6-12 months or longer, and may be incomplete.
Permanent Palsy - Serious
- Occurs due to actual nerve transection, thermal damage, or ischaemia.
- Risk of permanent facial palsy is ~1-2% for routine parotidectomy. - Scott-Brown's Otorhinolaryngology
- Risk is higher with:
- Malignant disease
- Revision surgery (scarred, distorted planes)
- Inexperienced surgeon
- Large or deep tumours
Consequences by branch injured
| Branch | Functional loss |
|---|---|
| Temporal | Inability to raise eyebrow, frontalis paralysis |
| Zygomatic | Inability to close eye (lagophthalmos) - corneal exposure and ulceration if not protected |
| Buccal | Upper lip weakness, nasolabial fold loss |
| Marginal mandibular | Lower lip weakness, drooling, asymmetric smile - most commonly affected |
| Cervical | Platysma weakness |
When the zygomatic/temporal divisions are affected, eye care (lubricants, taping at night, eye patch) is essential to protect the cornea from exposure keratitis. - Bailey and Love's
Management of post-operative facial palsy
- Observation if neuropraxia expected (no continuity lost)
- Eye care if upper face affected
- Electromyography (EMG) at 3-4 months if no recovery - to assess reinnervation
- Nerve repair (primary anastomosis or cable graft) if nerve was sacrificed or transected
- Facial reanimation procedures for established permanent palsy (cross-face nerve grafts, hypoglossal-facial anastomosis, free muscle transfer)
2. Frey's Syndrome (Auriculotemporal Syndrome / Gustatory Sweating) - Most Common Late Complication
Definition
Pathophysiology - Misdirected Nervous Regeneration
Incidence
- Clinically symptomatic in ~23-35% of patients after parotidectomy.
- If Minor's starch-iodine test is used to screen all patients, up to 96% show subclinical evidence of gustatory sweating. - Cummings Otolaryngology
- Onset typically within the first year after surgery (latent period 5 weeks to several months), but can occur decades later.
Diagnosis
- Minor's Starch-Iodine Test (Gold standard):
- Iodine solution painted over the preauricular region and allowed to dry
- Starch powder dusted over the painted area
- Patient chews a sialagogue (lemon wedge) for several minutes
- Appearance of dark blue-black spots = positive (dissolved starch + iodine + sweat)
Management
| Severity | Treatment |
|---|---|
| Mild | Antiperspirants containing aluminium chlorohydrate, applied to the skin |
| Moderate | Topical glycopyrrolate 1% roll-on lotion (anticholinergic) - effective |
| Moderate | Topical atropine cream |
| Severe | Botulinum toxin A (intradermal injection into the affected area) - most effective treatment; benefit lasts ~18 months for 60% of patients - Scott-Brown's |
| Refractory | Tympanic neurectomy - surgical interruption of the lesser petrosal nerve (parasympathetic pathway to parotid) via middle ear approach |
Prevention
- Thick skin flap elevation during surgery - creates greater distance between nerve ends and sweat glands
- Partial/superficial parotidectomy rather than total parotidectomy
- SCM muscle flap interposition between skin and surgical bed - reduces aberrant reinnervation (evidence remains inconclusive)
- Temporalis fascia, allodermis, or autologous fat interposition
- Extracapsular dissection (ECD) - significantly lower incidence vs superficial parotidectomy
- Careful SMAS closure
3. Greater Auricular Nerve Sensory Loss - Unavoidable
- The greater auricular nerve (C2, C3) crosses the surgical field over the SCM and is divided during parotidectomy.
- Results in sensory loss over the angle of the mandible, lower parotid region, and inferior two-thirds of the pinna (earlobe numbness is the most noticeable to patients).
- Considered unavoidable in standard parotidectomy, but sensory loss generally decreases in the first 12 months post-operatively.
- If the posterior branch of the nerve is identified and preserved at surgery, sensory loss may be reduced in both extent and duration. - Scott-Brown's Otorhinolaryngology
4. Sialocele and Salivary Fistula
Sialocele
- Collection of saliva under the skin flap from residual parotid acini left behind.
- Presents as a soft, fluctuant, painless preauricular swelling appearing 1-2 weeks post-operatively.
- Management:
- Repeated aspiration
- Pressure dressings
- Anticholinergics (e.g., oral glycopyrrolate, hyoscine) to reduce salivary secretion
- Usually self-limiting; resolves spontaneously
Salivary Fistula
- Persistent leakage of clear sialorrhoea from the wound.
- Less common than sialocele.
- Management: aspiration, pressure dressings, anticholinergics, wound care.
- Longstanding fistulae may require low-dose radiotherapy to ablate residual acini. - Bailey and Love's
Prevention: underrunning the capsule during closure to avoid exposing the main acinar ductal system. - Bailey and Love's
5. First Bite Syndrome
- Severe cramping pain in the parotid region on the first bite of each meal, diminishing with subsequent bites.
- Caused by disruption of sympathetic supply to the parotid bed; parasympathetic activity causes maximal myoepithelial cell contraction at the first stimulus (first bite).
- More common after deep lobe parotidectomy or surgery near the parapharyngeal space.
- Management: gabapentin, carbamazepine, botulinum toxin injection.
B. General Complications
6. Haematoma
- Uncommon; occurs early (within 24-48 hours).
- Presents as rapidly expanding preauricular/neck swelling, pain, and tense wound.
- Small haematomas resolve spontaneously; large collections require surgical evacuation under general anaesthesia.
- Prevention: meticulous intraoperative haemostasis, suction drain placement.
- Extreme collections with discolouration suggest a bleeding diathesis. - Bailey and Love's
7. Wound Infection
- Parotidectomy is a clean operation and infection is rare (<1%).
- Risk reduced by: aseptic drain management and timely drain removal.
- If infection occurs: antibiotics ± drainage.
8. Cosmetic Deformity
- Can be mitigated by autologous fat transfer (fat graft) placed at the time of primary surgery or as a secondary procedure. - Scott-Brown's; Bailey and Love's
Summary Table
| Complication | Type | Incidence | Key Management |
|---|---|---|---|
| Temporary facial palsy | Specific, early | Common | Observation, eye care; resolves 4-6 wks |
| Permanent facial palsy | Specific, late | 1-2% | Nerve repair, reanimation |
| Frey's syndrome | Specific, late | 23-35% symptomatic; 96% subclinical | Botulinum toxin A (most effective); antiperspirants; tympanic neurectomy |
| Great auricular nerve loss | Specific | Unavoidable | Reassurance; decreases over 12 months |
| Sialocele / Salivary fistula | Specific | Uncommon | Aspiration, pressure, anticholinergics |
| First bite syndrome | Specific | Uncommon | Gabapentin, botulinum toxin |
| Haematoma | General | Uncommon | Evacuation if large |
| Infection | General | Rare (<1%) | Antibiotics |
| Cosmetic hollow / scar | General | Common | Fat grafting |
Classify salivary gland tumours. Describe the presentation and management of a 30-year old man with pleomorphic adenoma of parotid gland. b) Investigation and management of cervical lymphadenopathy.
Part A: Classification of Salivary Gland Tumours + Pleomorphic Adenoma in a 30-Year-Old Man
Classification of Salivary Gland Tumours (WHO 2017)
I. Benign Epithelial Tumours
- Pleomorphic adenoma (most common overall)
- Myoepithelioma
- Basal cell adenoma
- Warthin's tumour (Adenolymphoma)
- Oncocytoma
- Cystadenoma
- Canalicular adenoma
- Sebaceous adenoma
- Ductal papillomas
II. Malignant Epithelial Tumours (22 entities)
- Mucoepidermoid carcinoma (most common malignant)
- Adenoid cystic carcinoma
- Acinic cell carcinoma
- Carcinoma ex pleomorphic adenoma
- Polymorphous adenocarcinoma
- Secretory carcinoma
- Salivary duct carcinoma
- Epithelial-myoepithelial carcinoma
- Adenocarcinoma NOS
- Others (basal cell adenocarcinoma, oncocytic carcinoma, lymphoepithelial carcinoma, etc.)
III. Mesenchymal Tumours (<20%)
IV. Haematolymphoid Tumours
Pleomorphic Adenoma of the Parotid: Presentation in a 30-Year-Old Man
Background / Epidemiology
Presentation
History
- Painless, slowly progressive swelling in the preauricular region - the hallmark presentation. The patient likely noticed a small lump that has been growing over months to years.
- Growth is gradual - rapid growth or pain should raise concern for malignant transformation.
- No facial nerve weakness - any facial palsy strongly suggests malignant change or a different diagnosis.
- No constitutional symptoms (no fever, weight loss - these suggest lymphoma or infection).
- Duration - weeks, months, years?
- Rate of growth - slow vs sudden acceleration?
- Any pain or tenderness?
- Any facial weakness/asymmetry (nerve involvement)?
- Any skin changes over the lump?
- Any swelling inside the mouth (deep lobe extension can present as paratonsillar bulge)?
- Any change with eating (salivary duct obstruction)?
- History of radiation to the head/neck (risk factor)
- No significant PMH expected for simple pleomorphic adenoma
Examination
- A visible, discrete preauricular or infra-auricular swelling, typically unilateral.
- Overlying skin normal - no erythema, peau d'orange, dimpling, or ulceration.
- Facial symmetry intact.
- If the tumour is large and long-standing, it can reach enormous proportions - the "double head" appearance. - Bailey and Love's
| Feature | Expected in Pleomorphic Adenoma |
|---|---|
| Site | Preauricular / parotid region |
| Size | Variable - usually 2-4 cm at presentation |
| Shape | Smooth, bosselated (lobulated surface) |
| Consistency | Firm to rubbery (varies: soft if myxoid; hard if chondroid/calcified) |
| Edge | Well-defined, distinct margin |
| Mobility | Mobile in all directions - not fixed to skin or underlying muscle |
| Skin tethering | Absent |
| Muscle fixity | Not fixed to masseter |
| Tenderness | Non-tender |
| Transillumination | Not transilluminable (solid tumour) |
"Pleomorphic adenoma presents as a painless, well-defined solitary mobile mass with gradual progression over many years." - Bailey and Love's
- All 5 branches tested: temporal, zygomatic, buccal, marginal mandibular, cervical.
- Should be entirely normal in uncomplicated pleomorphic adenoma.
- Check for a paratonsillar or soft palate bulge (deep lobe extension through the stylomandibular tunnel).
- Bimanual palpation of the buccal space and Stensen duct.
- Palpate all cervical lymph node levels - should be no lymphadenopathy in benign disease.
- Examine the opposite parotid (synchronous tumours are rare but possible).
Histopathology (for completeness)
- Gross: Well-circumscribed, firm, nodular, white-tan cut surface with cartilaginous areas and sometimes cystic degeneration.
- Micro: Mixed epithelial, myoepithelial, and stromal components in a myxoid/chondroid stroma.
- The capsule is thin and incomplete in ~50% of cases - especially the myxoid type, which is fragile and prone to intraoperative rupture.
- Calcification or bone is virtually pathognomonic of pleomorphic adenoma.
- Malignant transformation risk: historically ~1-5% at 10 years; actual risk is probably very low (~0.15% show features of malignant change). - Scott-Brown's Otorhinolaryngology
Investigations
-
Clinical assessment - as above
-
Imaging:
- Ultrasound (first line): Well-defined, hypoechoic solid mass, lobulated margins, posterior acoustic enhancement. Distinguishes solid from cystic. Guides FNAC.
- MRI (preferred for parotid): Superior soft tissue detail; defines deep lobe extension, parapharyngeal involvement, relationship to facial nerve plane. Pleomorphic adenoma shows high signal on T2. Calcification/bone = virtually diagnostic.
- CT: Less preferred but used if MRI unavailable or for bony detail.
- Sialography: Not routinely required.
-
Tissue diagnosis:
- FNAC (Fine Needle Aspiration Cytology): Widely used first-line tissue diagnosis. Sensitivity ~80-90%. Shows characteristic "chondromyxoid matrix" with epithelial and myoepithelial cells. Safe, no seeding risk.
- Core needle biopsy: More reliable histology; preferred if FNAC inconclusive.
- Open/excision biopsy: Avoided pre-operatively (causes scarring, risk of capsule breach and seeding).
Management
Decision to operate
- Definitive histology (cannot distinguish from malignancy without tissue)
- Continued growth if untreated
- Small but real risk of malignant transformation (carcinoma ex pleomorphic adenoma) - Scott-Brown's
Choice of operation
| Site | Operation |
|---|---|
| Superficial lobe (majority) | Superficial parotidectomy with facial nerve preservation - the standard operation |
| Deep lobe / both lobes | Total conservative parotidectomy (preserving facial nerve) |
| Minor salivary gland (palate etc.) | Wide local excision |
| Submandibular gland | Gland excision (extracapsular) |
- Superficial parotidectomy with a cuff of normal tissue is the operation of choice.
- The principle is: remove the tumour with a margin of normal parotid parenchyma wherever possible, to include any pseudopods from the incomplete capsule.
- Enucleation is absolutely contraindicated - the thin, incomplete capsule means enucleation almost invariably breaches the tumour and seeds the field, leading to multifocal recurrence. - Scott-Brown's; Bailey and Love's
- Extracapsular dissection (ECD) may be considered as an alternative in expert hands for small, mobile, superficial tumours.
Intraoperative principles
- Identify and preserve the facial nerve (tragal pointer, tympanomastoid suture, posterior digastric).
- Handle the tumour with minimal direct contact.
- Avoid capsule rupture - the myxoid stroma makes it fragile. If rupture occurs, contain the spillage and remove all visible tumour material.
- Intraoperative nerve monitoring (IONM) recommended.
Post-operative
- Suction drain for 24-48 hours.
- Monitor facial nerve function.
- Histological confirmation of diagnosis and adequate margins.
- Surveillance: clinical review ± imaging; recurrence typically presents 5-10 years later.
Recurrence
- Overall recurrence rate ~2%; data from Dutch national registry showed 6.7% at 20 years.
- Recurrence is almost always multifocal.
- Caused by: enucleation, capsule breach/tumour spillage, or inadequate margin.
- Recurrent tumours carry ~3% risk of malignant change.
- Management of recurrence: total parotidectomy ± post-operative radiotherapy; requires experienced head and neck surgeon.
Part B: Investigation and Management of Cervical Lymphadenopathy
Definition
Classification / Causes
By Duration
| Type | Definition |
|---|---|
| Acute | <2 weeks |
| Subacute | 2-6 weeks |
| Chronic | >6 weeks (most concerning for malignancy) |
By Cause (Surgical sieve: INVITED MD or similar)
| Category | Examples |
|---|---|
| Infective | Viral: EBV (infectious mononucleosis), CMV, HIV, adenovirus, rubella, COVID-19 |
| Bacterial: Streptococcal tonsillitis, TB (most common cause of chronic cervical LN worldwide), cat scratch disease (Bartonella), actinomycosis, brucellosis | |
| Fungal: Histoplasmosis | |
| Inflammatory / Autoimmune | Kikuchi's disease, sarcoidosis, SLE, Kawasaki disease, Castleman's disease |
| Neoplastic - Primary | Lymphoma: Hodgkin's (Reed-Sternberg cells; bimodal age distribution) and Non-Hodgkin's |
| Neoplastic - Secondary (Metastatic) | Head and neck primary (oral cavity, pharynx, larynx, thyroid, parotid), lung, breast, gastric, unknown primary |
| Drug-induced | Phenytoin, allopurinol, penicillin |
| Other | Thyroglossal cyst, branchial cyst, lipoma, sebaceous cyst (non-nodal causes of neck lumps) |
Investigations
Step 1: History and Examination (most important step)
- Age (young = reactive/lymphoma; old = metastatic)
- Duration and progression (rapid = infection/lymphoma; slow = metastatic)
- Associated symptoms:
- Fever, night sweats, weight loss ("B symptoms") = lymphoma
- Sore throat, URTI = reactive
- Cough, haemoptysis = TB, lung cancer
- Ear/nose/throat symptoms = head and neck primary
- Dysphagia, odynophagia = pharyngeal/oesophageal primary
- Smoking, alcohol (risk of HNSCC)
- Travel history (TB endemic areas, EBV)
- HIV risk factors
- Occupation (animal contact = cat scratch, brucellosis)
- Characteristics of the node: Size, consistency (soft/firm/hard/rubbery), mobility, tenderness, fluctuance, skin changes (erythema, sinus)
- Tender, mobile = reactive/infective
- Hard, fixed, irregular = malignant
- Rubbery = lymphoma
- Fluctuant = abscess or TB (cold abscess)
- Level of node (I-VI) - guides primary site of cancer
- Bilateral vs unilateral - bilateral = reactive/systemic; unilateral = more often metastatic
- Full ENT/head and neck examination - oral cavity, oropharynx, nasopharynx, larynx, thyroid, parotid
- Systemic examination - splenomegaly (lymphoma, EBV), hepatomegaly, other lymph node groups
Step 2: Blood Tests
| Test | Purpose |
|---|---|
| FBC + differential | Lymphocytosis (EBV), neutrophilia (infection), pancytopaenia (marrow infiltration) |
| ESR, CRP | Infection, inflammation, lymphoma |
| Monospot / Paul-Bunnell test + EBV serology | Infectious mononucleosis |
| CMV, HIV serology | Viral causes |
| Mantoux / tuberculin skin test | TB exposure |
| IGRA (Interferon-Gamma Release Assay) | Active / latent TB |
| Serum ACE, calcium | Sarcoidosis |
| LDH, uric acid | Lymphoma (tumour lysis markers) |
| Thyroid function tests | Thyroid malignancy |
| LFTs | Liver involvement |
Step 3: Imaging
| Investigation | Role |
|---|---|
| Ultrasound neck | First-line; size, number, morphology (round vs oval, echogenicity, hilar architecture); guides biopsy |
| CT neck with contrast | Essential for malignancy staging; identifies primary tumour, extracapsular spread, deep compartment nodes |
| CT chest/abdomen/pelvis | Systemic staging in lymphoma, metastatic disease |
| MRI neck | Better soft tissue detail; perineural spread |
| PET-CT | Lymphoma staging, unknown primary, response assessment |
| CXR | TB (hilar lymphadenopathy, consolidation), lung primary, mediastinal lymphoma |
Step 4: Tissue Diagnosis
| Technique | Indications / Notes |
|---|---|
| FNAC (Fine Needle Aspiration Cytology) | First-line tissue investigation; quick, safe, minimally invasive; excellent for metastatic carcinoma and reactive nodes; less reliable for lymphoma (architectural pattern needed) |
| Core needle biopsy (CNB) | Better histological architecture; preferred if lymphoma suspected; image-guided |
| Excision biopsy | Gold standard for lymphoma diagnosis (whole node needed for architecture); used when FNAC/CNB non-diagnostic; also for suspected TB (culture + histology) |
| Endoscopy + biopsy | Panendoscopy (direct laryngoscopy, pharyngoscopy, oesophagoscopy, bronchoscopy) if occult primary suspected |
| Bone marrow biopsy | Lymphoma staging |
Important rule: Do NOT perform excision biopsy if metastatic SCC is suspected before ENT endoscopy - removal of the nodal metastasis may compromise neck dissection planes. Investigate the primary first.
Step 5: Special Tests
- Sputum AFB smear + culture (if TB suspected)
- Nasopharyngoscopy + biopsy (EBV-related NPC - common in Southeast Asia)
- HPV testing on node biopsy (HPV-related oropharyngeal SCC)
Management
1. Reactive / Infective Lymphadenopathy
- Viral (EBV, CMV): Supportive; reassurance; most resolve in 2-6 weeks.
- Bacterial (streptococcal): Antibiotics (amoxicillin/penicillin); if abscess - incision and drainage.
- TB: Anti-tuberculous therapy (RHEZ - Rifampicin, Isoniazid, Ethambutol, Pyrazinamide for 2 months, then RH for 4 months); surgical drainage only if fluctuant cold abscess fails medical therapy.
- Cat scratch disease: Azithromycin; usually self-limiting.
2. Lymphoma
- Referred to haematology/oncology.
- Hodgkin's lymphoma: ABVD chemotherapy (Adriamycin, Bleomycin, Vinblastine, Dacarbazine) ± radiotherapy; excellent prognosis.
- Non-Hodgkin's lymphoma: R-CHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, Prednisolone) for B-cell NHL; other regimens depending on subtype.
3. Metastatic Carcinoma (from Head and Neck Primary)
- Identify and treat the primary - surgery ± radiotherapy ± chemotherapy depending on site and stage.
- Neck dissection (selective or comprehensive) to treat nodal disease.
- Chemoradiotherapy for unresectable or organ-preservation protocols (oropharyngeal SCC).
- Unknown primary: Panendoscopy ± tonsillectomy; if still unknown - treat bilateral neck and potential mucosal primary sites with chemoradiotherapy.
4. Thyroid Malignancy
- Total thyroidectomy + neck dissection.
- Radioiodine ablation.
- TSH suppression.
5. Sarcoidosis
- Observation if asymptomatic.
- Corticosteroids if systemic involvement.
6. Inflammatory (Kikuchi's Disease, Castleman's)
- Kikuchi's: Self-limiting; NSAIDs; rarely hydroxychloroquine.
- Castleman's: Surgery (unicentric); rituximab/siltuximab (multicentric).
Summary Flowchart
Cervical lymphadenopathy
↓
History + Examination
↓
Duration < 2 weeks, tender, URTI symptoms, young patient
→ Treat conservatively; review in 2-4 weeks
→ If resolving: reassure
↓ (if not resolving or suspicious features)
Bloods + Ultrasound neck
↓
FNAC / Core biopsy
↓
Reactive: Treat cause
Lymphoma: Haematology referral → excision biopsy → chemo/RT
Metastatic SCC: ENT endoscopy → identify/treat primary + neck dissection
TB: Anti-tuberculous therapy
Att
- Att = Attention (you want to flag something)?
- Atticotomy (surgical procedure)?
- Attic cholesteatoma?
- Something else entirely?
Initial management and complications of typhoid ileal perforation. [6]
Initial Management and Complications of Typhoid Ileal Perforation
Background
- Located on the antimesenteric border of the terminal ileum (within 60 cm of the ileocaecal valve)
- Often multiple (in up to 30-40% of cases) - making simple repair inadequate in many instances
- Associated with faecal peritonitis - causing septic shock and rapid deterioration
Initial Management
Step 1: Immediate Resuscitation (A-B-C-D-E approach)
- Ensure airway is patent; administer high-flow oxygen (15L/min via non-rebreather mask)
- Monitor oxygen saturation; prepare for intubation if respiratory failure
- Establish two large-bore IV cannulas (14-16G)
- Send urgent bloods: FBC, U&E, LFTs, coagulation screen, blood cultures (×2), serum procalcitonin, cross-match
- IV fluid resuscitation: Crystalloids (normal saline or Hartmann's/Ringer's lactate) - 1-2L bolus immediately; reassess continuously
- Insert urinary catheter - monitor urine output (target >0.5 mL/kg/hr)
- Insert nasogastric tube - decompress the stomach, prevent aspiration; keep on free drainage (NPO status)
- Monitor vitals: pulse, BP, RR, temperature, SpO2 - frequent reassessment
Step 2: Investigations
| Investigation | Purpose |
|---|---|
| Erect CXR | Free gas under diaphragm (pneumoperitoneum) - confirms perforation |
| AXR (erect + supine) | Pneumoperitoneum; dilated bowel loops |
| USS abdomen | Free fluid in peritoneum; may identify the perforation site |
| CT abdomen (if stable) | Confirms perforation, extent of contamination, number of perforations |
| FBC | Leucopenia or leucocytosis; anaemia |
| Widal test / Typhidot | Serological diagnosis; Widal: O titre ≥1:160 = significant |
| Blood cultures | Positive in 1st-2nd week (most reliable diagnostic test) |
| Stool cultures | Positive from 2nd week onward |
| Bone marrow culture | Most sensitive (90%); rarely done in acute setting |
| ABG | Metabolic acidosis, respiratory failure |
| Serum electrolytes | Hyponatraemia common in typhoid |
Step 3: Antibiotics (Anti-typhoid + Broad-spectrum for peritonitis)
| Setting | First-line agent | Dose | Duration |
|---|---|---|---|
| Empirical / MDR-endemic | Ceftriaxone | 2 g IV once daily | 10-14 days |
| Fully susceptible | Ciprofloxacin | 400 mg IV q12h | 5-7 days |
| Alternative | Azithromycin | 500 mg IV/OD | 10 days |
Note: Fluoroquinolones should no longer be used as first-line empirical therapy in the Indian subcontinent due to high prevalence of decreased susceptibility. Ceftriaxone is the preferred empirical agent. - Harrison's
- Metronidazole 500 mg IV q8h (anaerobic cover)
- Piperacillin-tazobactam or Meropenem if severely septic or MDR concern
- This covers gram-negatives and anaerobes from faecal contamination
Step 4: Supportive Measures Pre-operatively
- Strict NPO (nil per oral)
- Nasogastric tube on free drainage (decompression, reduce contamination at surgery)
- Urinary catheter (fluid balance monitoring)
- Analgesia: IV morphine titrated to pain (do NOT withhold analgesia)
- Anti-pyretics: Paracetamol IV for fever control
- DVT prophylaxis: LMWH (after surgery) + TED stockings
- Stress ulcer prophylaxis: IV proton pump inhibitor
- Correct coagulopathy: FFP if INR elevated; platelet transfusion if platelets <50 × 10⁹/L
- Blood transfusion if Hb <7-8 g/dL
Step 5: Emergency Surgery
- Assessment: Identify all perforations carefully - multiple perforations in 30-40% of cases; examine the entire ileum systematically.
- Peritoneal lavage: Copious irrigation with warm saline (3-6 litres) to reduce faecal contamination.
- Surgical options - choice depends on:
- Number of perforations
- Condition of bowel (degree of inflammation, ischaemia)
- Degree of peritoneal contamination
- Patient's haemodynamic status
- Surgeon's experience
| Situation | Surgical Option |
|---|---|
| Single perforation, healthy bowel margins, minimal contamination | Simple closure (transverse, two-layer) - most common for single perforation |
| Multiple perforations / perforation with surrounding ischaemia / close perforations | Resection + primary anastomosis (if contamination not severe) OR Resection + ileostomy (damage control) |
| Severely compromised patient, massive contamination | Damage control surgery: resection + bring both ends as stomas; anastomosis deferred |
| Right ileocaecal involvement | Right hemicolectomy ± ileostomy |
- Do the minimum necessary to save life.
- Resect perforated segment; create temporary ileostomy.
- Close abdomen (even if temporary).
- ICU resuscitation.
- Definitive anastomosis at 48-72 hours ("second look" laparotomy) once physiologically stable.
- Post-washout: Drains placed in pelvis and paracolic gutters.
- Wound closure: Primary closure if possible; consider delayed primary closure if grossly contaminated.
Step 6: Post-operative Intensive Care
- ICU admission in most cases.
- Continue IV antibiotics (anti-typhoid + broad-spectrum).
- Mechanical ventilation if required.
- Vasopressors (noradrenaline) if septic shock persists.
- Total parenteral nutrition (TPN) or early enteral feeding via NG/NJ tube.
- Strict fluid balance, electrolyte correction.
- Monitor for post-operative complications.
Complications
A. Local Complications
| Complication | Notes |
|---|---|
| Faecal peritonitis | Present at diagnosis; ongoing if inadequate surgical clearance |
| Intra-abdominal abscess | Residual/recurrent sepsis post-operatively; subphrenic, pelvic, paracolic - requires CT-guided drainage |
| Wound infection / dehiscence | Common due to contaminated field; may progress to burst abdomen |
| Anastomotic leak (if primary anastomosis done) | Presents 3-5 days post-op; re-laparotomy required |
| Enterocutaneous fistula | If anastomosis/repair breaks down; often closes with conservative management |
| Re-perforation | Multiple perforations may have been missed intraoperatively; requires re-laparotomy |
| Intestinal obstruction | Early (ileus, anastomotic oedema) or late (adhesions) |
| Stoma complications | Prolapse, retraction, necrosis, parastomal hernia (if ileostomy performed) |
| Incisional hernia | Late complication; common after contaminated laparotomy |
B. Systemic Complications of Typhoid Fever Itself
| Complication | Notes |
|---|---|
| Septic shock | Most common cause of death; systemic vasodilation, multi-organ failure |
| Intestinal haemorrhage | Second most common intestinal complication (after perforation); erosion of mesenteric vessels by ulcers; presents with fresh rectal bleeding; managed conservatively (most settle) |
| Pneumonia | S. typhi bronchopneumonia or aspiration pneumonia |
| Myocarditis / pericarditis | Rare; presents with chest pain, ECG changes, elevated troponin |
| Typhoid encephalopathy | Altered consciousness, delirium, seizures; mechanism unclear (endotoxin-mediated); treat with dexamethasone in severe cases |
| Haematological: DIC, thrombocytopaenia, haemolytic anaemia | DIC from sepsis; requires FFP, cryoprecipitate, platelet transfusion |
| Hepatitis | Elevated transaminases; rarely hepatic failure |
| Cholecystitis | S. typhi can colonise gallbladder; chronic carrier state |
| Osteomyelitis / Septic arthritis | Haematogenous spread; especially in patients with sickle cell disease |
| Relapse | Occurs in ~5-10% of patients; less severe than initial illness; treat with another course of antibiotics |
| Chronic carrier state | Persistence of S. typhi in gallbladder (>1 year excretion); risk for spreading disease to contacts |
C. Post-operative Complications Summary
Immediate (0-24 h): Septic shock, DIC, respiratory failure
Early (1-7 days): Wound infection, anastomotic leak, ileus, intra-abdominal abscess, re-perforation
Late (>1 week): Adhesive obstruction, fistula, incisional hernia, chronic carrier state
Prognosis
| Factor | Associated with worse outcome |
|---|---|
| Delay to surgery (>24h from perforation) | Strongly negative |
| Multiple perforations | Higher mortality |
| Age extremes | |
| Faecal peritonitis with severe contamination | |
| MDR S. typhi | |
| Pre-operative shock |