What are the pharmacological actions adverse effects and uses of ACE inhibitors
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ACE inhibitors"[MeSH Terms] AND "pharmacology"[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Let me compose the full response.
ACE Inhibitors - Pharmacological Actions, Adverse Effects, and Uses
Source: Lippincott Illustrated Reviews: Pharmacology & Goodman and Gilman's Pharmacological Basis of Therapeutics
Mechanism of Action
ACE (Angiotensin-Converting Enzyme) inhibitors block the enzyme ACE, which normally cleaves angiotensin I (inactive) into angiotensin II (a potent vasoconstrictor). The result is a two-pronged vasodilatory effect:
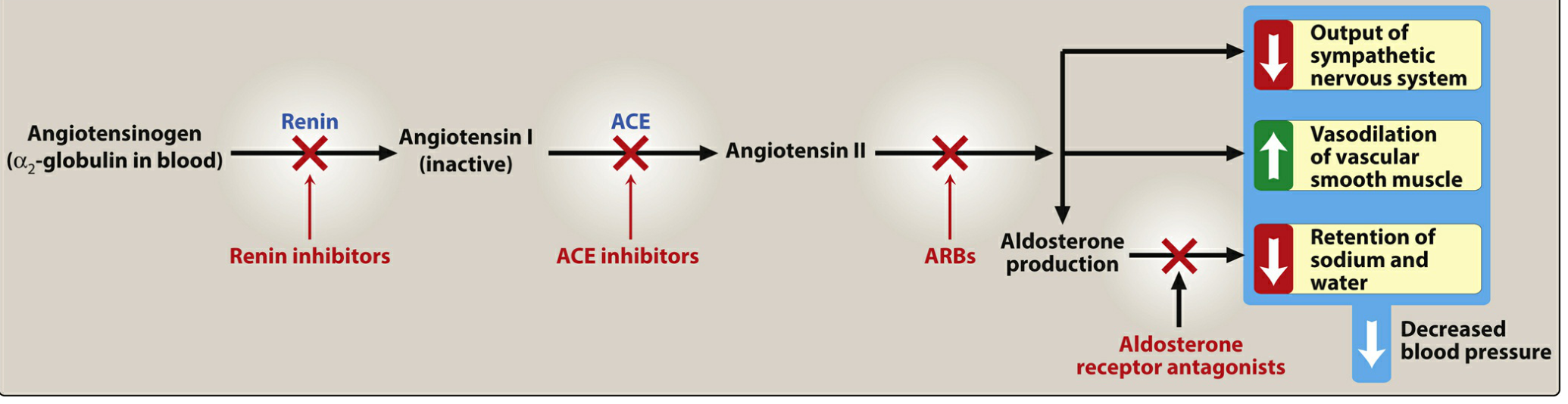
Figure: Effects of various drug classes on the renin-angiotensin-aldosterone system (RAAS). ACE inhibitors block the conversion of Angiotensin I → Angiotensin II.
Pharmacological Actions
-
Vasodilation (arteriolar and venous)
- Reduced angiotensin II → decreased vasoconstriction
- ACE also normally breaks down bradykinin; inhibiting ACE raises bradykinin levels, which stimulates production of nitric oxide and prostacyclin (both potent vasodilators)
- Net result: decreased peripheral vascular resistance → lower blood pressure
-
Reduced aldosterone secretion
- Less angiotensin II → less aldosterone → less sodium and water retention
- Reduces both preload and afterload, lowering myocardial workload
-
Renal hemodynamic effects
- Efferent arteriolar vasodilation → decreased intraglomerular pressure
- Slows progression of diabetic nephropathy; decreases albuminuria
-
Cardiac remodeling
- Sustained use leads to regression of left ventricular hypertrophy
- Improved ventricular remodeling after myocardial infarction
-
Neurohormonal effects
- Blunts the angiotensin II-mediated increase in epinephrine and aldosterone seen in heart failure
- Improves clinical signs/symptoms of HF and significantly improves survival in HFrEF (heart failure with reduced ejection fraction)
Therapeutic Uses
| Indication | Notes |
|---|---|
| Hypertension | First-line; equally effective at equivalent doses across all ACE inhibitors |
| Heart failure (HFrEF) | Standard of care; all stages of LV failure; start low, titrate to target dose |
| Post-MI | Improve ventricular remodeling; indicated in all patients post-MI |
| Diabetic nephropathy | Slow disease progression, reduce albuminuria |
| Chronic kidney disease | First-line in hypertensive patients with CKD |
| Coronary artery disease | Patients at high cardiovascular risk benefit from long-term therapy |
| Left ventricular hypertrophy | Regression with chronic use |
| Asymptomatic LV dysfunction | Can be used even before overt HF symptoms develop |
Adverse Effects
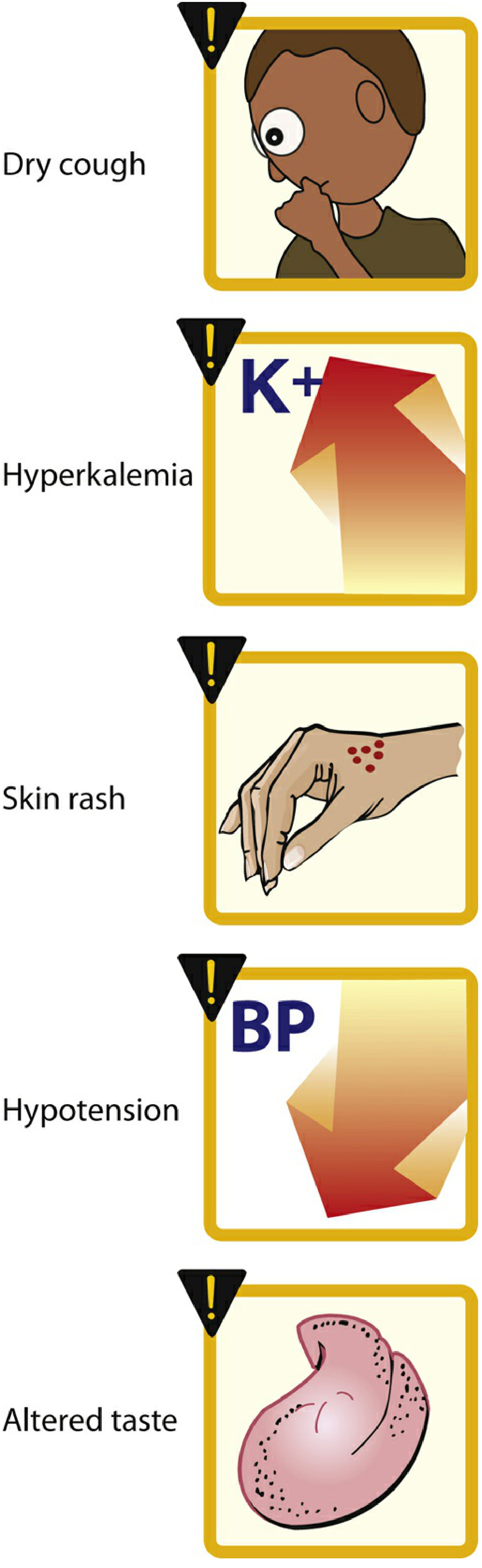
Figure 8.11: Common adverse effects of ACE inhibitors (Lippincott)
| Adverse Effect | Mechanism / Notes |
|---|---|
| Dry cough | Most common (up to 10% of patients); due to raised bradykinin and substance P in the pulmonary tree; more frequent in women; resolves within days of stopping |
| Angioedema | Rare but life-threatening; swelling of lips, oral mucosa, throat; also bradykinin-mediated; contraindication to further use |
| Hyperkalemia | Reduced aldosterone → reduced K+ excretion; caution with K+ supplements, K+-sparing diuretics, and MRAs |
| Hypotension | Especially first-dose or postural; much more common if combined with a diuretic |
| Renal insufficiency / elevated creatinine | Efferent dilation can reduce GFR; a rise in creatinine up to 30% above baseline is acceptable and does not require discontinuation |
| Skin rash | More common with captopril (sulfhydryl group) |
| Dysgeusia (altered taste) | Particularly with captopril |
| Leukopenia / neutropenia | Rare; more common with captopril at high doses |
| Teratogenicity | Contraindicated in pregnancy - causes fetal renal anomalies, oligohydramnios, and fetal death (especially 2nd/3rd trimester) |
Pharmacokinetics - Key Points
- All ACE inhibitors are orally bioavailable as a drug or prodrug
- Except captopril and lisinopril, all others are prodrugs requiring hepatic activation (these two may be preferred in severe hepatic impairment)
- Fosinopril is the only ACE inhibitor with dual elimination (renal + fecal) - does not require dose adjustment in renal impairment
- Enalaprilat is the only formulation available for IV administration
- Captopril absorption is reduced by food - take on empty stomach
- Half-lives of active compounds range from 2 to 12 hours, but ACE inhibition lasts much longer
Common Drugs in This Class
| Drug | Brand Name | Notes |
|---|---|---|
| Captopril | Generic | Sulfhydryl group; rash/taste disturbance more common; taken on empty stomach |
| Enalapril | Vasotec | Prodrug; most widely used |
| Lisinopril | Prinivil, Zestril | Active drug (not prodrug); once daily |
| Ramipril | Altace | Prodrug; used in high-CV-risk patients (HOPE trial) |
| Fosinopril | Generic | Dual elimination; safe in renal impairment |
| Quinapril | Accupril | Prodrug |
| Perindopril | Generic | Prodrug |
| Enalaprilat | IV form | Only IV ACE inhibitor |
Key Drug Interactions
- Potassium-sparing diuretics / K+ supplements / MRAs: risk of severe hyperkalemia
- Diuretics: increased risk of first-dose hypotension
- NSAIDs: blunt antihypertensive effect; increase risk of renal dysfunction
- ARBs or aliskiren: dual RAAS blockade - generally avoided due to increased risk of hypotension, hyperkalemia, and renal failure
Contraindications
- Pregnancy (all trimesters - teratogenic)
- History of angioedema with an ACE inhibitor
- Bilateral renal artery stenosis (can precipitate acute kidney injury)
- Severe hyperkalemia
Sources: Lippincott Illustrated Reviews: Pharmacology, 8th Ed., Ch. 8 & 10; Goodman & Gilman's The Pharmacological Basis of Therapeutics, Ch. 43.
Arb s
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
I have excellent, comprehensive content from multiple authoritative textbooks. Here is the full answer:
Angiotensin Receptor Blockers (ARBs)
Sources: Lippincott Illustrated Reviews: Pharmacology | Katzung's Basic & Clinical Pharmacology | Goodman & Gilman's Pharmacological Basis of Therapeutics | Braunwald's Heart Disease
Mechanism of Action
ARBs are competitive antagonists at the AT1 (angiotensin type 1) receptor - the receptor subtype responsible for virtually all the harmful biological effects of angiotensin II. By blocking AT1 receptors, ARBs prevent angiotensin II from exerting its effects regardless of how angiotensin II was produced (via ACE or alternative pathways like chymase).
Figure: RAAS pathway - ARBs block the AT1 receptor, downstream of the ACE inhibition site
Key distinction from ACE inhibitors:
- ARBs do not inhibit ACE-mediated degradation of bradykinin or substance P
- Therefore, they cause no cough and much less angioedema
- They provide more complete blockade of angiotensin II effects (ACE inhibitors only block one enzyme; angiotensin II can still be made via other routes like chymase)
- During AT1 blockade, increased angiotensin II stimulates unopposed AT2 receptors, which may produce additional vasodilation and antiproliferative effects
Pharmacological Actions
| Action | Mechanism |
|---|---|
| Vasodilation (arterioles + veins) | Block AT1 → smooth muscle relaxation → reduced peripheral resistance |
| Reduced aldosterone | AT1 block → less aldosterone → increased Na+/water excretion |
| Reduced cardiac preload and afterload | Venodilatation + arteriolar dilation |
| Increased renal salt and water excretion | Reduced aldosterone + efferent arteriolar dilation |
| Reduced plasma volume | Natriuresis and diuresis |
| Anti-hypertrophic | Block AT1-mediated cardiac and vascular smooth muscle hypertrophy (important in HF remodeling) |
| Renoprotective | Reduce intraglomerular pressure; slow diabetic nephropathy progression |
| AT2 stimulation | Increased AngII (from lost AT1 feedback) stimulates AT2 → vasodilation, antiproliferative effects |
Therapeutic Uses
1. Hypertension
- First-line agents, especially with coexisting diabetes, heart failure, or CKD
- Full antihypertensive effect typically reached after ~4 weeks
- Most ARBs are effective with once-daily dosing (exception: losartan may need twice daily in some)
- If BP not controlled with ARB alone, add a drug with different mechanism (diuretic or CCB)
- Young/middle-aged Caucasians respond well; elderly African American patients are relatively more resistant
2. Heart Failure with Reduced EF (HFrEF)
- Indicated when ACE inhibitors are not tolerated (cough/angioedema), as a substitute
- Losartan, valsartan, and candesartan are most studied in HFrEF
- Candesartan (CHARM-Alternative trial) significantly reduced all-cause mortality, CV death, and hospitalizations in ACE-intolerant HF patients
- High-dose losartan (150 mg/day) is superior to low-dose (HEAAL trial)
- Not recommended to combine ARB + ACE inhibitor due to increased hypotension, hyperkalemia, and renal dysfunction without added mortality benefit
3. Post-Myocardial Infarction
- Valsartan was non-inferior to captopril for mortality in post-MI LV dysfunction (VALIANT trial)
- An alternative to ACE inhibitors in post-MI patients who are ACE-intolerant
4. Diabetic Nephropathy
- Slow progression; reduce proteinuria
- Valsartan may reduce the incidence of new-onset diabetes in patients with impaired glucose tolerance
5. Chronic Kidney Disease
- Renoprotective; first-line in hypertensive CKD patients
6. Marfan Syndrome
- Losartan may be as effective as atenolol (standard treatment) by blocking AT1-mediated TGF-β signaling
Pharmacokinetics
| Property | Details |
|---|---|
| Route | All orally active |
| Dosing | Once daily (most); valsartan: twice daily |
| Protein binding | Highly plasma protein bound |
| Losartan | Undergoes extensive first-pass hepatic metabolism → active metabolite (EXP-3174); other ARBs have inactive metabolites |
| Elimination | Urine and feces (dual route for most) |
| Onset of full effect | ~4 weeks |
Adverse Effects
ARBs have a similar adverse effect profile to ACE inhibitors, with two important differences:
| Adverse Effect | Notes |
|---|---|
| Hypotension | Especially first-dose; increased risk if on diuretic |
| Hyperkalemia | Reduced aldosterone → K+ retention; monitor K+ levels; caution with K+-sparing diuretics/MRAs/K+ supplements |
| Renal insufficiency | Monitor creatinine; rise up to 30% above baseline acceptable |
| Teratogenicity | Contraindicated in pregnancy (all trimesters) |
| Cough | Significantly lower incidence than ACE inhibitors (no bradykinin accumulation) |
| Angioedema | Much rarer than with ACE inhibitors; still possible |
| Sprue-like enteropathy | A syndrome of chronic diarrhea with intestinal villous atrophy; notably associated with olmesartan |
| Dizziness/headache | Common at initiation |
From the ON-TARGET trial (Goodman & Gilman): Telmisartan caused cough in 1.1% vs 4.2% with ramipril, and angioedema in 0.1% vs 0.3% - confirming much lower incidence of these bradykinin-mediated effects.
Contraindications
- Pregnancy (teratogenic - renal dysgenesis, oligohydramnios, fetal death)
- Bilateral renal artery stenosis
- Severe hyperkalemia
- Combination with ACE inhibitor (dual RAAS blockade not recommended - increases adverse effects without benefit)
- Combination with aliskiren in patients with diabetes or renal impairment
Available ARBs
| Drug | Brand Name | Notes |
|---|---|---|
| Losartan | Cozaar | First ARB approved; active metabolite (EXP-3174); may need twice daily; uricosuric (lowers uric acid) |
| Valsartan | Diovan | Twice daily; studied in HFrEF (Val-HeFT, VALIANT) |
| Candesartan | Atacand | Most studied in HF (CHARM trials); prodrug |
| Irbesartan | Avapro | Once daily; studied in diabetic nephropathy |
| Telmisartan | Micardis | Longest half-life; PPAR-γ agonism; studied in ON-TARGET |
| Olmesartan | Benicar | Associated with sprue-like enteropathy |
| Azilsartan | Edarbi | Most potent BP-lowering ARB |
| Eprosartan | Teveten | No longer marketed in the U.S. |
ARBs vs ACE Inhibitors - Key Comparison
| Feature | ACE Inhibitors | ARBs |
|---|---|---|
| Mechanism | Block ACE enzyme | Block AT1 receptor |
| Bradykinin effect | Increase (bradykinin accumulates) | No change |
| Cough | Common (up to 10%) | Much rarer |
| Angioedema | Rare but possible | Very rare |
| Completeness of AngII block | Partial (alternative pathways exist) | More complete |
| AT2 stimulation | Minimal | Yes (increased AngII stimulates AT2) |
| Efficacy in HF | Equivalent | Equivalent (as substitute) |
| Preferred if | Standard first choice | ACE inhibitor intolerance |
Sources: Lippincott Illustrated Reviews: Pharmacology, 8th Ed., Ch. 8 & 10; Katzung's Basic & Clinical Pharmacology, 16th Ed., Ch. 11; Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 30 & 43; Braunwald's Heart Disease, 12th Ed., Ch. 50
Difference and similarities between ace inhibitor and arb s
Finding Sources
Finding Sources
I have everything needed from the prior sessions and the new queries. Here is the full, structured comparison:
ACE Inhibitors vs ARBs - Differences and Similarities
Sources: Lippincott Illustrated Reviews: Pharmacology | Katzung's Basic & Clinical Pharmacology 16e | Goodman & Gilman's Pharmacological Basis of Therapeutics | Braunwald's Heart Disease | Brenner & Rector's The Kidney
Quick Visual Overview
ACE inhibitors act at ACE (enzyme); ARBs act downstream at the AT1 receptor
SIMILARITIES
1. Mechanism - Both Block the RAAS
Both drug classes ultimately prevent angiotensin II from acting at the AT1 receptor, either by reducing its production (ACE inhibitors) or by blocking where it binds (ARBs).
2. Pharmacological Effects - Nearly Identical
| Effect | ACE Inhibitors | ARBs |
|---|---|---|
| Arteriolar vasodilation | Yes | Yes |
| Venous vasodilation (reduced preload) | Yes | Yes |
| Reduced aldosterone secretion | Yes | Yes |
| Decreased sodium and water retention | Yes | Yes |
| Reduced cardiac afterload and preload | Yes | Yes |
| Anti-hypertrophic (LV regression) | Yes | Yes |
| Efferent arteriolar dilation (renal) | Yes | Yes |
3. Therapeutic Indications - Essentially the Same
- Hypertension - both are first-line agents with similar efficacy
- Heart failure (HFrEF) - both reduce morbidity and mortality
- Post-myocardial infarction - both improve LV remodeling
- Diabetic nephropathy - both slow progression and reduce proteinuria
- Chronic kidney disease - both renoprotective (reduce intraglomerular pressure)
- Left ventricular hypertrophy - both cause regression with chronic use
From Brenner & Rector's The Kidney: "Although ACE inhibitors and ARBs differ significantly in their effects on the RAAS in ways that may be therapeutically relevant, experimental studies indicate that both treatments produce similar changes in glomerular hemodynamics (for a given blood pressure change)."
4. Adverse Effect Overlap
| Adverse Effect | Both Cause? |
|---|---|
| Hypotension (especially first dose) | Yes |
| Hyperkalemia | Yes |
| Renal insufficiency / raised creatinine | Yes |
| Teratogenicity (contraindicated in pregnancy) | Yes |
| Dizziness | Yes |
5. Drug Interactions - Same Cautions
- Both require caution with potassium-sparing diuretics, K+ supplements, and MRAs (hyperkalemia risk)
- Both potentiated by diuretics (hypotension)
- Both blunted by NSAIDs
- Should NOT be combined with each other - dual RAAS blockade increases hypotension, hyperkalemia, and renal impairment without mortality benefit (ON-TARGET trial)
6. Contraindications - Shared
- Pregnancy
- Bilateral renal artery stenosis
- Severe hyperkalemia
DIFFERENCES
| Feature | ACE Inhibitors | ARBs |
|---|---|---|
| Site of action | Block the ACE enzyme (prevents conversion of Ang I → Ang II) | Block AT1 receptor (prevent Ang II binding) |
| Completeness of AngII blockade | Incomplete - angiotensin II can still be produced via alternate enzymes (chymase, cathepsin, etc.) | More complete - blocks the receptor regardless of how Ang II was made |
| Effect on bradykinin | Increase bradykinin (ACE normally breaks it down) | No effect on bradykinin levels |
| Effect on substance P | Increase | No change |
| Dry cough | Common - up to 10% of patients (bradykinin + substance P in pulmonary tree) | Much rarer (no bradykinin accumulation) |
| Angioedema | Rare (~0.1-0.3%) but life-threatening | Very rare (~0.1%) - significantly lower |
| AT2 receptor stimulation | Minimal (Ang II levels fall) | Yes - Ang II rises (lost AT1 feedback) → stimulates AT2 → vasodilation, antiproliferative effects |
| Nitric oxide / prostacyclin | Increased (via raised bradykinin) | Not directly increased |
| First choice vs substitute | Primary / first choice | Substitute when ACE inhibitor not tolerated |
| Prodrug vs active | Most are prodrugs (except captopril, lisinopril) | Most are active drugs (losartan converts to active metabolite EXP-3174) |
| IV formulation | Yes (enalaprilat) | None available |
| Uricosuric effect | None | Losartan is uniquely uricosuric (lowers uric acid - useful in gout) |
| Sprue-like enteropathy | Not reported | Olmesartan specifically linked |
| Skin rash / dysgeusia | Yes (especially captopril - sulfhydryl group) | Not a significant feature |
| Effect on bradykinin-related vasodilation | Enhanced (therapeutic benefit contribution) | No direct bradykinin contribution |
| Renal protection - degree of evidence | Long-established | Equivalent (well-established in diabetic nephropathy) |
| Cost | Generally cheaper (generics widely available) | Slightly more expensive |
Why Bradykinin Matters - The Key Difference Explained
ACE Inhibitors:
Ang I --[ACE blocked]-→ Ang II ↓
Bradykinin --[ACE blocked]-→ NOT degraded → Bradykinin ↑
↓
Nitric oxide ↑ + Prostacyclin ↑ → Vasodilation ✓
BUT also: Cough, Angioedema ✗
ARBs:
Ang I → Ang II (via ACE + chymase etc.) → AT1 receptor BLOCKED
Bradykinin → degraded normally → No bradykinin accumulation
↓
No cough ✓, No angioedema ✓
BUT: No bradykinin-mediated vasodilation contribution
Clinical Decision - When to Choose Which?
| Situation | Choice |
|---|---|
| Standard first-line hypertension | ACE inhibitor (cheaper, more established) |
| Hypertension + cough on ACE inhibitor | Switch to ARB |
| History of angioedema on ACE inhibitor | ARB (but use caution - angioedema can still rarely occur) |
| HFrEF | ACE inhibitor preferred; ARB if ACE-intolerant |
| Diabetic nephropathy | Either (evidence for both; ARBs slightly more studied in type 2 DM) |
| Hypertension + gout | Losartan (uricosuric effect) |
| Marfan syndrome | Losartan (reduces TGF-β signaling) |
| Hyperkalemia or renal insufficiency | Neither well-tolerated; re-evaluate dose |
| Pregnancy | Both absolutely contraindicated |
| Combination of both | Not recommended - no added benefit; more harm |
Summary Table
| Property | ACE Inhibitors | ARBs |
|---|---|---|
| Mechanism | Block ACE enzyme | Block AT1 receptor |
| BP lowering efficacy | Equal | Equal |
| Bradykinin effect | Raise | No change |
| Cough | Common (~10%) | Rare (<2%) |
| Angioedema | Rare (~0.3%) | Very rare (~0.1%) |
| Hyperkalemia | Yes | Yes |
| Teratogenicity | Yes | Yes |
| Renoprotection | Yes | Yes |
| Cardiac remodeling | Yes | Yes |
| Preferred role | First choice | ACE-intolerant substitute |
| IV form | Yes (enalaprilat) | No |
| Unique side effect | Cough, rash (captopril) | Sprue-like enteropathy (olmesartan) |
| Cost | Lower | Higher |
Bottom line: ACE inhibitors and ARBs are clinically interchangeable for most indications with nearly identical efficacy. The primary reason to choose an ARB over an ACE inhibitor is intolerance to ACE inhibitor (cough in ~10%, angioedema). ARBs offer more complete blockade of angiotensin II but lose the bradykinin-mediated vasodilatory benefit. Combining both is not recommended.
Sources: Lippincott Illustrated Reviews: Pharmacology 8e, Ch. 8 & 10 | Katzung's Basic & Clinical Pharmacology 16e, Ch. 11 | Goodman & Gilman's 14e, Ch. 30 & 43 | Braunwald's Heart Disease 12e, Ch. 50 | Brenner & Rector's The Kidney
Create a comparison presentation on RAAS blockers
Reading File
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null && mkdir -p /home/daytona/workspace/raas…
Writing File
~/raas-blockers-ppt/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "RAAS Blockers: A Comprehensive Comparison";
pres.author = "Orris Medical";
// ─── COLOR PALETTE ───────────────────────────────────────────────────────────
const C = {
navy: "0D2B55", // dominant dark bg
teal: "0E7C7B", // ACE inhibitor accent
crimson: "C0392B", // ARB accent
gold: "E8A838", // Renin inhibitor accent
purple: "6C3483", // MRA accent
slate: "1C3A5E", // section header bg
light: "EAF2FB", // content bg light
white: "FFFFFF",
offwhite:"F4F6F7",
ltgray: "D5D8DC",
dktext: "1A252F",
subtext: "566573",
};
// ─── HELPER FUNCTIONS ────────────────────────────────────────────────────────
function titleSlide(slide, title, subtitle) {
// Full dark bg
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
// Teal accent bar left
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: C.teal } });
// Gold accent bar
slide.addShape(pres.ShapeType.rect, { x: 0.18, y: 0, w: 0.06, h: 5.625, fill: { color: C.gold } });
// Crimson bar bottom
slide.addShape(pres.ShapeType.rect, { x: 0, y: 5.2, w: 10, h: 0.425, fill: { color: C.crimson } });
slide.addText(title, {
x: 0.6, y: 1.2, w: 8.8, h: 1.6,
fontSize: 40, bold: true, color: C.white,
fontFace: "Calibri", align: "left", valign: "middle",
});
slide.addText(subtitle, {
x: 0.6, y: 2.9, w: 8, h: 0.8,
fontSize: 20, color: C.gold, fontFace: "Calibri",
align: "left", bold: false, italic: true,
});
slide.addText("Sources: Lippincott Pharmacology • Katzung • Goodman & Gilman • Braunwald's Heart Disease", {
x: 0.6, y: 5.05, w: 8.8, h: 0.25,
fontSize: 9, color: C.white, fontFace: "Calibri", align: "left",
});
}
function sectionDivider(slide, sectionNum, title, accent, subtitle) {
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.08, fill: { color: accent } });
slide.addShape(pres.ShapeType.rect, { x: 0, y: 5.545, w: 10, h: 0.08, fill: { color: accent } });
slide.addText(`0${sectionNum}`, {
x: 0.5, y: 0.8, w: 2, h: 2,
fontSize: 100, bold: true, color: accent,
fontFace: "Calibri", align: "left", valign: "middle",
transparency: 60,
});
slide.addText(title, {
x: 2.8, y: 1.6, w: 6.5, h: 1.2,
fontSize: 36, bold: true, color: C.white,
fontFace: "Calibri", align: "left", valign: "middle",
});
if (subtitle) {
slide.addText(subtitle, {
x: 2.8, y: 2.85, w: 6.5, h: 0.7,
fontSize: 16, color: C.ltgray, fontFace: "Calibri", align: "left", italic: true,
});
}
}
function slideHeader(slide, title, accentColor) {
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.75, fill: { color: accentColor || C.slate } });
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0.75, w: 10, h: 5.0, fill: { color: C.offwhite } });
slide.addText(title, {
x: 0.3, y: 0, w: 9.4, h: 0.75,
fontSize: 22, bold: true, color: C.white,
fontFace: "Calibri", valign: "middle", margin: 0,
});
}
function colorBox(slide, x, y, w, h, color, label, labelColor) {
slide.addShape(pres.ShapeType.rect, { x, y, w, h, fill: { color }, line: { color: C.white, width: 1 } });
if (label) {
slide.addText(label, {
x, y, w, h,
fontSize: 11, bold: true, color: labelColor || C.white,
fontFace: "Calibri", align: "center", valign: "middle",
});
}
}
function pillBadge(slide, x, y, w, label, color, textColor) {
slide.addShape(pres.ShapeType.roundRect, {
x, y, w, h: 0.32,
fill: { color },
line: { color, width: 0 },
rectRadius: 0.06,
});
slide.addText(label, {
x, y, w, h: 0.32,
fontSize: 10, bold: true, color: textColor || C.white,
fontFace: "Calibri", align: "center", valign: "middle",
});
}
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 1 — TITLE
// ════════════════════════════════════════════════════════════════════════════
let s = pres.addSlide();
titleSlide(s,
"RAAS Blockers:\nA Comprehensive Comparison",
"ACE Inhibitors • ARBs • Renin Inhibitors • Mineralocorticoid Receptor Antagonists"
);
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 2 — RAAS PATHWAY OVERVIEW (text diagram)
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "The RAAS Pathway & Sites of Drug Action", C.slate);
// Pathway boxes
const pathway = [
{ label: "Angiotensinogen\n(α₂-globulin)", x: 0.3, color: "2C3E50" },
{ label: "Angiotensin I\n(inactive)", x: 2.4, color: "2C3E50" },
{ label: "Angiotensin II\n(active)", x: 4.5, color: "922B21" },
{ label: "AT1 Receptor\nActivation", x: 6.6, color: "78281F" },
];
pathway.forEach(p => {
colorBox(s, p.x, 0.95, 1.9, 0.75, p.color, p.label, C.white);
});
// Arrows between pathway boxes
[2.3, 4.4, 6.5].forEach(x => {
s.addShape(pres.ShapeType.rightArrow, { x, y: 1.15, w: 0.25, h: 0.35, fill: { color: C.ltgray } });
});
// Drug intervention labels
const interventions = [
{ label: "RENIN INHIBITORS\n(Aliskiren)\nBlock here ↑", x: 0.3, y: 1.85, color: C.gold },
{ label: "ACE INHIBITORS\n(Captopril, Lisinopril…)\nBlock conversion ↑", x: 2.4, y: 1.85, color: C.teal },
{ label: "ARBs\n(Losartan, Valsartan…)\nBlock AT1 receptor ↑", x: 6.6, y: 1.85, color: C.crimson },
];
interventions.forEach(iv => {
slide_addRoundedBox(s, iv.x, iv.y, 1.9, 0.9, iv.color, iv.label);
});
function slide_addRoundedBox(sl, x, y, w, h, color, label) {
sl.addShape(pres.ShapeType.roundRect, {
x, y, w, h,
fill: { color },
line: { color: C.white, width: 1 },
rectRadius: 0.05,
});
sl.addText(label, {
x, y, w, h,
fontSize: 9.5, color: C.white, bold: true,
fontFace: "Calibri", align: "center", valign: "middle",
});
}
// Aldosterone pathway
colorBox(s, 4.5, 1.85, 1.9, 0.5, "7D6608", "Aldosterone\nRelease", C.white);
s.addShape(pres.ShapeType.downArrow, { x: 5.35, y: 1.72, w: 0.3, h: 0.18, fill: { color: "7D6608" } });
// MRA label
slide_addRoundedBox(s, 4.5, 2.5, 1.9, 0.7, C.purple, "MRAs\n(Spironolactone, Eplerenone)\nBlock aldosterone receptor");
// Effects boxes (right side)
const effects = [
{ label: "↓ Vasoconstriction", color: "1A5276" },
{ label: "↓ Aldosterone", color: "1A5276" },
{ label: "↓ SNS activity", color: "1A5276" },
{ label: "→ ↓ Blood Pressure", color: "145A32" },
];
effects.forEach((e, i) => {
colorBox(s, 8.6, 0.88 + i * 0.55, 1.3, 0.45, e.color, e.label, C.white);
if (i < 3) s.addShape(pres.ShapeType.downArrow, { x: 9.12, y: 0.88 + i * 0.55 + 0.45, w: 0.25, h: 0.15, fill: { color: C.ltgray } });
});
// Legend note
s.addText("Blue arrows = drug blocks pathway | All RAAS blockers ultimately reduce blood pressure, cardiac remodeling, and renal damage", {
x: 0.3, y: 3.45, w: 9.4, h: 0.35,
fontSize: 10, italic: true, color: C.subtext, fontFace: "Calibri",
});
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 3 — ACE INHIBITORS OVERVIEW
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "ACE Inhibitors — Overview", C.teal);
// Left panel
s.addShape(pres.ShapeType.rect, { x: 0.2, y: 0.85, w: 4.5, h: 4.6, fill: { color: "EBF5FB" }, line: { color: C.teal, width: 1.5 } });
pillBadge(s, 0.35, 0.92, 1.6, "MECHANISM", C.teal);
s.addText([
{ text: "Block ACE enzyme", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Prevent Ang I → Ang II conversion", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Bradykinin NOT degraded → accumulates", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "↑ Nitric oxide + Prostacyclin (vasodilation)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "↓ Aldosterone → ↓ Na+/H₂O retention", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "↓ Cardiac preload AND afterload", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Efferent arteriolar dilation → ↓ intraglomerular pressure", options: { bullet: { code: "2022" } } },
], { x: 0.3, y: 1.3, w: 4.3, h: 2.5, fontSize: 11, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
pillBadge(s, 0.35, 3.85, 1.2, "KEY DRUGS", C.teal);
s.addText("Captopril • Enalapril • Lisinopril\nRamipril • Fosinopril • Quinapril\nPerindopril • Trandolapril", {
x: 0.3, y: 4.17, w: 4.3, h: 0.9,
fontSize: 11, color: C.dktext, fontFace: "Calibri", italic: true,
});
// Right panel
s.addShape(pres.ShapeType.rect, { x: 4.9, y: 0.85, w: 4.9, h: 4.6, fill: { color: "EBF5FB" }, line: { color: C.teal, width: 1.5 } });
pillBadge(s, 5.05, 0.92, 1.5, "USES", C.teal);
const uses_ace = [
"Hypertension (first-line)",
"Heart failure / HFrEF",
"Post-MI (ventricular remodeling)",
"Diabetic nephropathy",
"Chronic kidney disease",
"LV hypertrophy regression",
"Asymptomatic LV dysfunction",
"High CV risk patients",
];
s.addText(uses_ace.map((u, i) => ({ text: u, options: { bullet: { code: "2022" }, breakLine: i < uses_ace.length - 1 } })),
{ x: 5.0, y: 1.3, w: 4.6, h: 2.5, fontSize: 11, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
pillBadge(s, 5.05, 3.85, 1.8, "ADVERSE EFFECTS", C.crimson);
const ae_ace = [
{ text: "Dry cough (up to 10%)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Angioedema (rare, life-threatening)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Hyperkalemia", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Hypotension (first dose)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Renal insufficiency", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Teratogenic (avoid in pregnancy)", options: { bullet: { code: "2022" } } },
];
s.addText(ae_ace, { x: 5.0, y: 4.2, w: 4.6, h: 1.8, fontSize: 10.5, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.25 });
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 4 — ARBs OVERVIEW
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "Angiotensin Receptor Blockers (ARBs) — Overview", C.crimson);
s.addShape(pres.ShapeType.rect, { x: 0.2, y: 0.85, w: 4.5, h: 4.6, fill: { color: "FDEDEC" }, line: { color: C.crimson, width: 1.5 } });
pillBadge(s, 0.35, 0.92, 1.6, "MECHANISM", C.crimson);
s.addText([
{ text: "Competitive antagonists at AT1 receptor", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Block Ang II regardless of how it was made", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "More complete Ang II blockade than ACEi", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Do NOT affect bradykinin levels", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "↑ Ang II → stimulates unopposed AT2 receptor", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "AT2 stimulation → vasodilation + antiproliferative", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "↓ Aldosterone, ↓ preload and afterload", options: { bullet: { code: "2022" } } },
], { x: 0.3, y: 1.3, w: 4.3, h: 2.5, fontSize: 11, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
pillBadge(s, 0.35, 3.85, 1.2, "KEY DRUGS", C.crimson);
s.addText("Losartan • Valsartan • Candesartan\nIrbesartan • Telmisartan • Olmesartan\nAzilsartan • Eprosartan", {
x: 0.3, y: 4.17, w: 4.3, h: 0.9,
fontSize: 11, color: C.dktext, fontFace: "Calibri", italic: true,
});
s.addShape(pres.ShapeType.rect, { x: 4.9, y: 0.85, w: 4.9, h: 4.6, fill: { color: "FDEDEC" }, line: { color: C.crimson, width: 1.5 } });
pillBadge(s, 5.05, 0.92, 1.5, "USES", C.crimson);
const uses_arb = [
"Hypertension (first-line)",
"HFrEF (substitute for ACEi)",
"Post-MI with LV dysfunction",
"Diabetic nephropathy (Type 2 DM)",
"Chronic kidney disease",
"ACEi-intolerant patients",
"Marfan syndrome (Losartan)",
"LV hypertrophy",
];
s.addText(uses_arb.map((u, i) => ({ text: u, options: { bullet: { code: "2022" }, breakLine: i < uses_arb.length - 1 } })),
{ x: 5.0, y: 1.3, w: 4.6, h: 2.5, fontSize: 11, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.3 });
pillBadge(s, 5.05, 3.85, 1.8, "ADVERSE EFFECTS", "922B21");
const ae_arb = [
{ text: "Hypotension (first dose)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Hyperkalemia", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Renal insufficiency", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Cough — much rarer than ACEi", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Angioedema — very rare", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Olmesartan → sprue-like enteropathy", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Teratogenic (avoid in pregnancy)", options: { bullet: { code: "2022" } } },
];
s.addText(ae_arb, { x: 5.0, y: 4.2, w: 4.6, h: 1.8, fontSize: 10.5, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.25 });
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 5 — RENIN INHIBITORS + MRAs
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "Renin Inhibitors & Mineralocorticoid Receptor Antagonists (MRAs)", C.slate);
// Renin Inhibitors left
s.addShape(pres.ShapeType.rect, { x: 0.2, y: 0.85, w: 4.6, h: 4.6, fill: { color: "FEF9E7" }, line: { color: C.gold, width: 2 } });
pillBadge(s, 0.35, 0.9, 1.8, "RENIN INHIBITORS", C.gold, C.dktext);
s.addText("Aliskiren (Tekturna)", {
x: 0.3, y: 1.29, w: 4.4, h: 0.35,
fontSize: 13, bold: true, color: C.gold, fontFace: "Calibri",
});
s.addText([
{ text: "Mechanism", options: { bold: true, breakLine: true } },
{ text: "Directly inhibit renin enzyme", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Act earliest in RAAS cascade", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Block Angiotensinogen → Ang I step", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "", options: { breakLine: true } },
{ text: "Uses", options: { bold: true, breakLine: true } },
{ text: "Hypertension (monotherapy or add-on)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "", options: { breakLine: true } },
{ text: "Adverse Effects", options: { bold: true, breakLine: true } },
{ text: "Diarrhea (especially high dose)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Hyperkalemia, renal impairment", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Cough, angioedema (less than ACEi)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "", options: { breakLine: true } },
{ text: "Contraindications", options: { bold: true, breakLine: true } },
{ text: "Pregnancy, diabetes + ACEi/ARB combo", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Renal insufficiency", options: { bullet: { code: "2022" } } },
], { x: 0.3, y: 1.65, w: 4.4, h: 3.6, fontSize: 10.5, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.2 });
// MRAs right
s.addShape(pres.ShapeType.rect, { x: 5.1, y: 0.85, w: 4.7, h: 4.6, fill: { color: "F5EEF8" }, line: { color: C.purple, width: 2 } });
pillBadge(s, 5.25, 0.9, 1.2, "MRAs", C.purple);
s.addText("Spironolactone • Eplerenone • Finerenone", {
x: 5.2, y: 1.29, w: 4.5, h: 0.35,
fontSize: 12, bold: true, color: C.purple, fontFace: "Calibri",
});
s.addText([
{ text: "Mechanism", options: { bold: true, breakLine: true } },
{ text: "Block aldosterone at mineralocorticoid receptor", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Prevent Na+ retention and K+ excretion", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Prevent myocardial fibrosis and hypertrophy", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "", options: { breakLine: true } },
{ text: "Uses", options: { bold: true, breakLine: true } },
{ text: "Symptomatic HFrEF", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Post-MI with LV dysfunction + HF", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Resistant hypertension (add-on)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Primary hyperaldosteronism", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "", options: { breakLine: true } },
{ text: "Adverse Effects", options: { bold: true, breakLine: true } },
{ text: "Hyperkalemia (monitor K+)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Gynecomastia, dysmenorrhea (spironolactone)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Eplerenone: selective → fewer endocrine SE", options: { bullet: { code: "2022" } } },
], { x: 5.2, y: 1.65, w: 4.5, h: 3.65, fontSize: 10.5, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.2 });
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 6 — HEAD-TO-HEAD COMPARISON TABLE: ACEi vs ARBs
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "ACE Inhibitors vs ARBs — Head-to-Head Comparison", C.navy);
const rows = [
["Feature", "ACE Inhibitors", "ARBs"],
["Site of Action", "ACE enzyme (blocks Ang I → Ang II)", "AT1 receptor (blocks Ang II binding)"],
["Bradykinin effect", "↑ Bradykinin accumulation", "No effect on bradykinin"],
["Completeness of AngII block", "Partial (chymase pathway remains)", "More complete"],
["Dry Cough", "Common (~10% patients)", "Rare (<2%)"],
["Angioedema", "Rare (~0.3%)", "Very rare (~0.1%)"],
["AT2 stimulation", "Minimal", "Yes — Ang II ↑ stimulates AT2"],
["Hyperkalemia", "Yes", "Yes"],
["Teratogenicity", "Yes — avoid in pregnancy", "Yes — avoid in pregnancy"],
["Preferred role", "First choice", "Substitute if ACEi not tolerated"],
["IV formulation", "Yes (Enalaprilat)", "None"],
["Unique effects", "Rash/dysgeusia (captopril)", "Sprue enteropathy (olmesartan); Uricosuric (losartan)"],
["Cost", "Generally lower", "Generally higher"],
];
const colW = [2.6, 3.4, 3.4];
const colX = [0.15, 2.75, 6.15];
const rowH = 0.33;
const startY = 0.82;
rows.forEach((row, ri) => {
row.forEach((cell, ci) => {
const isHeader = ri === 0;
const isFeatureCol = ci === 0;
const bg = isHeader ? C.navy : (ri % 2 === 0 ? "EBF5FB" : C.white);
const textColor = isHeader ? C.gold : (isFeatureCol ? C.navy : C.dktext);
s.addShape(pres.ShapeType.rect, {
x: colX[ci], y: startY + ri * rowH, w: colW[ci], h: rowH,
fill: { color: bg }, line: { color: C.ltgray, width: 0.5 },
});
s.addText(cell, {
x: colX[ci] + 0.05, y: startY + ri * rowH, w: colW[ci] - 0.1, h: rowH,
fontSize: isHeader ? 11 : 9.5,
bold: isHeader || isFeatureCol,
color: textColor, fontFace: "Calibri",
valign: "middle", margin: 2,
});
});
});
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 7 — FULL 4-WAY COMPARISON TABLE
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "All RAAS Blockers — 4-Way Comparison", C.slate);
const rows4 = [
["Property", "ACE Inhibitors", "ARBs", "Renin Inhibitors", "MRAs"],
["Target", "ACE enzyme", "AT1 receptor", "Renin enzyme", "Aldosterone receptor"],
["BP lowering", "✓✓✓", "✓✓✓", "✓✓", "✓✓"],
["Cough", "Common (~10%)", "Rare", "Rare", "No"],
["Angioedema", "Rare", "Very rare", "Rare", "No"],
["Hyperkalemia", "Yes", "Yes", "Yes", "Yes (main SE)"],
["Pregnancy", "CI", "CI", "CI", "CI"],
["Heart failure", "First-line", "ACEi substitute", "Not established", "First-line (add-on)"],
["Diabetic nephropathy", "Yes", "Yes", "Limited", "Yes (Finerenone)"],
["Unique SE", "Rash (captopril)", "Enteropathy (olmesartan)", "Diarrhea", "Gynecomastia (spiro)"],
];
const cW4 = [2.1, 1.95, 1.95, 1.95, 1.95];
const cX4 = [0.1, 2.2, 4.15, 6.1, 8.05];
const headerColors4 = [C.slate, C.teal, C.crimson, C.gold, C.purple];
rows4.forEach((row, ri) => {
row.forEach((cell, ci) => {
const isHeader = ri === 0;
let bg;
if (isHeader) {
bg = headerColors4[ci];
} else if (ci === 0) {
bg = "D5DBDB";
} else {
bg = ri % 2 === 0 ? "F2F3F4" : C.white;
}
const textColor = (isHeader || ci === 0) ? (ci === 3 ? C.dktext : C.white) : C.dktext;
s.addShape(pres.ShapeType.rect, {
x: cX4[ci], y: 0.82 + ri * 0.46, w: cW4[ci], h: 0.46,
fill: { color: bg }, line: { color: C.ltgray, width: 0.5 },
});
s.addText(cell, {
x: cX4[ci] + 0.04, y: 0.82 + ri * 0.46, w: cW4[ci] - 0.08, h: 0.46,
fontSize: isHeader ? 9.5 : 9,
bold: isHeader || ci === 0,
color: textColor, fontFace: "Calibri",
valign: "middle", align: ci === 0 ? "left" : "center", margin: 2,
});
});
});
// CI note
s.addText("CI = Contraindicated | ✓✓✓ = Strong evidence | ✓✓ = Moderate evidence", {
x: 0.1, y: 5.4, w: 9.8, h: 0.22,
fontSize: 8, italic: true, color: C.subtext, fontFace: "Calibri",
});
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 8 — PHARMACOKINETICS COMPARISON
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "Pharmacokinetics — Key Differences", C.slate);
// ACE inhibitors PK box
s.addShape(pres.ShapeType.rect, { x: 0.2, y: 0.85, w: 4.6, h: 4.6, fill: { color: "EBF5FB" }, line: { color: C.teal, width: 2 } });
s.addText("ACE Inhibitors", { x: 0.35, y: 0.9, w: 4.3, h: 0.38, fontSize: 14, bold: true, color: C.teal, fontFace: "Calibri" });
s.addText([
{ text: "Route: All orally bioavailable", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Prodrugs: Most (except captopril, lisinopril)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "IV form: Enalaprilat only", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Renal elimination: Most (except fosinopril)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Fosinopril: Dual renal + fecal — safe in renal impairment", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Captopril: Short-acting; take on empty stomach", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Half-life of active compounds: 2–12 hours", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "ACE inhibition lasts longer than plasma t½", options: { bullet: { code: "2022" } } },
], { x: 0.3, y: 1.33, w: 4.4, h: 3.9, fontSize: 11, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.35 });
// ARBs PK box
s.addShape(pres.ShapeType.rect, { x: 5.1, y: 0.85, w: 4.7, h: 4.6, fill: { color: "FDEDEC" }, line: { color: C.crimson, width: 2 } });
s.addText("ARBs", { x: 5.25, y: 0.9, w: 4.5, h: 0.38, fontSize: 14, bold: true, color: C.crimson, fontFace: "Calibri" });
s.addText([
{ text: "Route: All orally active", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Dosing: Once daily (most); valsartan twice daily", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Highly plasma protein bound", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Losartan: Active metabolite EXP-3174 (extensive first-pass)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Other ARBs: Inactive metabolites", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Elimination: Urine and feces (dual)", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "Full antihypertensive effect: ~4 weeks", options: { bullet: { code: "2022" }, breakLine: true } },
{ text: "No IV formulation available", options: { bullet: { code: "2022" } } },
], { x: 5.2, y: 1.33, w: 4.5, h: 3.9, fontSize: 11, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.35 });
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 9 — SIMILARITIES
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "ACE Inhibitors & ARBs — Shared Properties", C.slate);
const simCols = [
{
title: "Shared Pharmacology",
color: C.teal,
items: [
"Arteriolar + venous vasodilation",
"Reduce aldosterone secretion",
"Reduce Na+/H₂O retention",
"Reduce cardiac preload & afterload",
"Anti-hypertrophic (LV regression)",
"Efferent arteriolar dilation",
"Renoprotective effects",
],
},
{
title: "Shared Clinical Uses",
color: C.crimson,
items: [
"Hypertension (first-line)",
"Heart failure (HFrEF)",
"Post-MI / LV remodeling",
"Diabetic nephropathy",
"Chronic kidney disease",
"LV hypertrophy regression",
"High cardiovascular risk",
],
},
{
title: "Shared Adverse Effects",
color: "6C3483",
items: [
"Hypotension (first-dose effect)",
"Hyperkalemia",
"Renal insufficiency",
"Teratogenicity",
"Bilateral renal artery stenosis risk",
],
},
];
simCols.forEach((col, ci) => {
const x = 0.2 + ci * 3.25;
s.addShape(pres.ShapeType.rect, { x, y: 0.85, w: 3.1, h: 4.6, fill: { color: "F4F6F7" }, line: { color: col.color, width: 2 } });
s.addShape(pres.ShapeType.rect, { x, y: 0.85, w: 3.1, h: 0.45, fill: { color: col.color } });
s.addText(col.title, { x: x + 0.08, y: 0.85, w: 2.94, h: 0.45, fontSize: 12, bold: true, color: C.white, fontFace: "Calibri", valign: "middle" });
s.addText(
col.items.map((item, i) => ({ text: item, options: { bullet: { code: "2713" }, breakLine: i < col.items.length - 1 } })),
{ x: x + 0.08, y: 1.35, w: 2.94, h: 3.9, fontSize: 11, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.45 }
);
});
// Shared note at bottom
s.addShape(pres.ShapeType.rect, { x: 0.2, y: 5.22, w: 9.6, h: 0.32, fill: { color: "D6EAF8" }, line: { color: C.teal, width: 0.5 } });
s.addText("Both classes are NOT recommended in combination — dual RAAS blockade increases hyperkalemia, hypotension, and renal dysfunction without added mortality benefit (ON-TARGET trial)", {
x: 0.35, y: 5.22, w: 9.3, h: 0.32,
fontSize: 9, italic: true, color: C.navy, fontFace: "Calibri", valign: "middle",
});
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 10 — WHEN TO CHOOSE WHICH
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "Clinical Decision Guide — When to Choose Which RAAS Blocker", C.navy);
const decisions = [
{ situation: "Standard hypertension, no comorbidities", choice: "ACE Inhibitor", reason: "First-line, cheaper, well-established", color: C.teal },
{ situation: "Hypertension + cough on ACEi", choice: "Switch to ARB", reason: "No bradykinin accumulation → no cough", color: C.crimson },
{ situation: "Angioedema on ACEi", choice: "ARB (with caution)", reason: "Much lower incidence of angioedema", color: C.crimson },
{ situation: "HFrEF (primary)", choice: "ACE Inhibitor", reason: "Most established; survival benefit proven", color: C.teal },
{ situation: "HFrEF + ACEi-intolerant", choice: "ARB (candesartan, valsartan)", reason: "Non-inferior to ACEi; CHARM-Alt trial", color: C.crimson },
{ situation: "Symptomatic HFrEF + tolerating ACEi/ARB", choice: "Switch to ARNI (sacubitril/valsartan)", reason: "Superior to ACEi in PARADIGM-HF trial", color: "1A5276" },
{ situation: "Hypertension + gout", choice: "Losartan (ARB)", reason: "Unique uricosuric effect lowers uric acid", color: C.crimson },
{ situation: "Marfan syndrome", choice: "Losartan (ARB)", reason: "Blocks AT1-mediated TGF-β signaling", color: C.crimson },
{ situation: "Symptomatic HFrEF on ACEi + BB", choice: "Add MRA (spironolactone/eplerenone)", reason: "Reduces mortality (RALES, EMPHASIS-HF)", color: C.purple },
{ situation: "Pregnancy", choice: "Both CONTRAINDICATED", reason: "Both are teratogenic", color: "C0392B" },
];
decisions.forEach((d, i) => {
const y = 0.86 + i * 0.47;
s.addShape(pres.ShapeType.rect, { x: 0.1, y, w: 3.6, h: 0.43, fill: { color: "EAF2FB" }, line: { color: C.ltgray, width: 0.5 } });
s.addText(d.situation, { x: 0.15, y, w: 3.5, h: 0.43, fontSize: 9.5, color: C.dktext, fontFace: "Calibri", valign: "middle", bold: false });
s.addShape(pres.ShapeType.rect, { x: 3.7, y, w: 2.5, h: 0.43, fill: { color: d.color }, line: { color: C.white, width: 0.5 } });
s.addText(d.choice, { x: 3.75, y, w: 2.4, h: 0.43, fontSize: 9.5, bold: true, color: C.white, fontFace: "Calibri", valign: "middle" });
s.addShape(pres.ShapeType.rect, { x: 6.2, y, w: 3.7, h: 0.43, fill: { color: "F4F6F7" }, line: { color: C.ltgray, width: 0.5 } });
s.addText(d.reason, { x: 6.25, y, w: 3.6, h: 0.43, fontSize: 9, italic: true, color: C.subtext, fontFace: "Calibri", valign: "middle" });
});
// Column headers
["Clinical Situation", "Drug Choice", "Reason"].forEach((h, i) => {
const xs = [0.1, 3.7, 6.2];
const ws = [3.6, 2.5, 3.7];
s.addShape(pres.ShapeType.rect, { x: xs[i], y: 0.78, w: ws[i], h: 0.08, fill: { color: C.gold } });
});
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 11 — CONTRAINDICATIONS
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "Contraindications & Cautions for RAAS Blockers", "922B21");
const ciData = [
{
drug: "ALL RAAS Blockers",
color: "922B21",
items: [
"Pregnancy (all trimesters — teratogenic)",
"Bilateral renal artery stenosis",
"Severe hyperkalemia (K+ > 5.5 mEq/L)",
"Combination ACEi + ARB (dual RAAS blockade)",
],
},
{
drug: "ACE Inhibitors",
color: C.teal,
items: [
"History of ACEi-induced angioedema",
"Severe aortic stenosis (relative)",
"Caution: severe renal impairment (most need dose adjustment, except fosinopril)",
],
},
{
drug: "ARBs",
color: C.crimson,
items: [
"History of ARB-induced angioedema",
"Olmesartan: sprue-like enteropathy history",
"Combination with aliskiren in diabetes/renal impairment",
],
},
{
drug: "MRAs",
color: C.purple,
items: [
"Severe renal impairment (GFR < 30)",
"Hyperkalemia",
"Spironolactone: caution in men (gynecomastia)",
],
},
];
ciData.forEach((d, i) => {
const col = i < 2 ? i : i - 2;
const row = i < 2 ? 0 : 1;
const x = 0.2 + col * 4.85;
const y = 0.85 + row * 2.4;
s.addShape(pres.ShapeType.rect, { x, y, w: 4.6, h: 2.2, fill: { color: "FDFEFE" }, line: { color: d.color, width: 2 } });
s.addShape(pres.ShapeType.rect, { x, y, w: 4.6, h: 0.4, fill: { color: d.color } });
s.addText(d.drug, { x: x + 0.08, y, w: 4.44, h: 0.4, fontSize: 12, bold: true, color: i === 2 ? C.white : C.white, fontFace: "Calibri", valign: "middle" });
s.addText(
d.items.map((item, ii) => ({ text: item, options: { bullet: { code: "26A0" }, breakLine: ii < d.items.length - 1 } })),
{ x: x + 0.08, y: y + 0.45, w: 4.44, h: 1.65, fontSize: 10.5, color: C.dktext, fontFace: "Calibri", lineSpacingMultiple: 1.35 }
);
});
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 12 — KEY CLINICAL TRIALS
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
slideHeader(s, "Landmark Clinical Trials for RAAS Blockers", C.navy);
const trials = [
{ trial: "HOPE (2000)", drug: "Ramipril (ACEi)", finding: "↓ CV death, MI, stroke by 22% in high-risk patients", color: C.teal },
{ trial: "SOLVD (1991)", drug: "Enalapril (ACEi)", finding: "↓ Mortality + HF hospitalizations in HFrEF", color: C.teal },
{ trial: "CHARM-Alt (2003)", drug: "Candesartan (ARB)", finding: "↓ Mortality/hospitalizations in ACEi-intolerant HF", color: C.crimson },
{ trial: "VALIANT (2003)", drug: "Valsartan (ARB)", finding: "Non-inferior to captopril in post-MI LV dysfunction", color: C.crimson },
{ trial: "HEAAL (2009)", drug: "Losartan (ARB)", finding: "High-dose (150mg) superior to low-dose (50mg) in HFrEF", color: C.crimson },
{ trial: "ON-TARGET (2008)", drug: "Telmisartan vs Ramipril", finding: "Equal efficacy; less cough & angioedema with ARB; combo not better", color: "7D6608" },
{ trial: "RALES (1999)", drug: "Spironolactone (MRA)", finding: "↓ Mortality by 30% in severe HFrEF", color: C.purple },
{ trial: "EMPHASIS-HF (2011)", drug: "Eplerenone (MRA)", finding: "↓ CV death/hospitalizations in mild symptomatic HFrEF", color: C.purple },
{ trial: "PARADIGM-HF (2014)", drug: "Sacubitril/Valsartan (ARNI)", finding: "Superior to enalapril → ↓ CV death/HF hospitalizations by 20%", color: "1A5276" },
];
trials.forEach((t, i) => {
const y = 0.86 + i * 0.51;
s.addShape(pres.ShapeType.rect, { x: 0.1, y, w: 1.8, h: 0.47, fill: { color: t.color }, line: { color: C.white, width: 0.5 } });
s.addText(t.trial, { x: 0.12, y, w: 1.76, h: 0.47, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", align: "center" });
s.addShape(pres.ShapeType.rect, { x: 1.9, y, w: 2.4, h: 0.47, fill: { color: "EAF2FB" }, line: { color: C.ltgray, width: 0.5 } });
s.addText(t.drug, { x: 1.95, y, w: 2.3, h: 0.47, fontSize: 10, bold: true, color: C.dktext, fontFace: "Calibri", valign: "middle" });
s.addShape(pres.ShapeType.rect, { x: 4.3, y, w: 5.6, h: 0.47, fill: { color: i % 2 === 0 ? "F2F3F4" : C.white }, line: { color: C.ltgray, width: 0.5 } });
s.addText(t.finding, { x: 4.35, y, w: 5.5, h: 0.47, fontSize: 9.5, color: C.dktext, fontFace: "Calibri", valign: "middle" });
});
// ════════════════════════════════════════════════════════════════════════════
// SLIDE 13 — SUMMARY / CONCLUSION
// ════════════════════════════════════════════════════════════════════════════
s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.navy } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.06, fill: { color: C.teal } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 5.565, w: 10, h: 0.06, fill: { color: C.crimson } });
s.addText("Key Takeaways", {
x: 0.4, y: 0.25, w: 9.2, h: 0.65,
fontSize: 28, bold: true, color: C.gold, fontFace: "Calibri", align: "center",
});
const takeaways = [
{ icon: "→", text: "All RAAS blockers ultimately reduce Ang II activity — but at different points in the cascade", color: C.teal },
{ icon: "→", text: "ACEi and ARBs have near-identical clinical efficacy across HTN, HF, and CKD", color: C.crimson },
{ icon: "→", text: "The key difference: ACEi raise bradykinin → cough (10%) and angioedema; ARBs do not", color: C.gold },
{ icon: "→", text: "ARBs are the preferred substitute when ACEi are not tolerated", color: C.crimson },
{ icon: "→", text: "MRAs (spironolactone/eplerenone) add mortality benefit in HFrEF on top of ACEi/ARB + beta-blocker", color: C.purple },
{ icon: "→", text: "ARNI (sacubitril/valsartan) is now preferred over ACEi in HFrEF when tolerated", color: "5DADE2" },
{ icon: "→", text: "All RAAS blockers are CONTRAINDICATED in pregnancy and bilateral renal artery stenosis", color: "E74C3C" },
{ icon: "→", text: "Do NOT combine ACEi + ARB — dual RAAS blockade causes more harm than benefit", color: "E74C3C" },
];
takeaways.forEach((t, i) => {
s.addShape(pres.ShapeType.rect, { x: 0.35, y: 1.05 + i * 0.55, w: 0.04, h: 0.38, fill: { color: t.color } });
s.addText(t.text, {
x: 0.5, y: 1.05 + i * 0.55, w: 9.1, h: 0.42,
fontSize: 12, color: C.white, fontFace: "Calibri", valign: "middle",
});
});
// ════════════════════════════════════════════════════════════════════════════
// WRITE FILE
// ════════════════════════════════════════════════════════════════════════════
pres.writeFile({ fileName: "/home/daytona/workspace/raas-blockers-ppt/RAAS_Blockers_Comparison.pptx" })
.then(() => console.log("✅ Presentation saved successfully."))
.catch(err => console.error("❌ Error:", err));
Running Command
cd /home/daytona/workspace/raas-blockers-ppt && node build.js 2>&1
Running Command
ls -lh /home/daytona/workspace/raas-blockers-ppt/RAAS_Blockers_Comparison.pptx
Your presentation is ready! Download it here:
RAAS Blockers Comparison
Presentation · PPTX
Here's what's inside the 13-slide deck (430 KB):
| Slide | Content |
|---|---|
| 1 | Title slide — dark navy with teal/crimson/gold accents |
| 2 | RAAS Pathway Diagram — showing where each drug class acts |
| 3 | ACE Inhibitors — mechanism, uses, adverse effects, key drugs |
| 4 | ARBs — mechanism, uses, adverse effects, key drugs |
| 5 | Renin Inhibitors + MRAs — side-by-side overview |
| 6 | ACEi vs ARBs — detailed head-to-head comparison table |
| 7 | All 4 classes — 4-way comparison table |
| 8 | Pharmacokinetics — key differences (ACEi vs ARBs) |
| 9 | Similarities between ACEi and ARBs |
| 10 | Clinical Decision Guide — when to choose which drug |
| 11 | Contraindications and Cautions for all classes |
| 12 | Landmark Clinical Trials (HOPE, CHARM-Alt, RALES, PARADIGM-HF, etc.) |
| 13 | Key Takeaways — summary slide |
Color coding used throughout:
- 🔵 Teal = ACE Inhibitors
- 🔴 Crimson = ARBs
- 🟡 Gold = Renin Inhibitors
- 🟣 Purple = MRAs
This is a shared conversation. Sign in to Orris to start your own chat.