Umn vs lmn fnp
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I have all the information needed for a thorough, well-illustrated answer.
UMN vs LMN Facial Nerve Palsy (FNP)
The Key Anatomical Basis
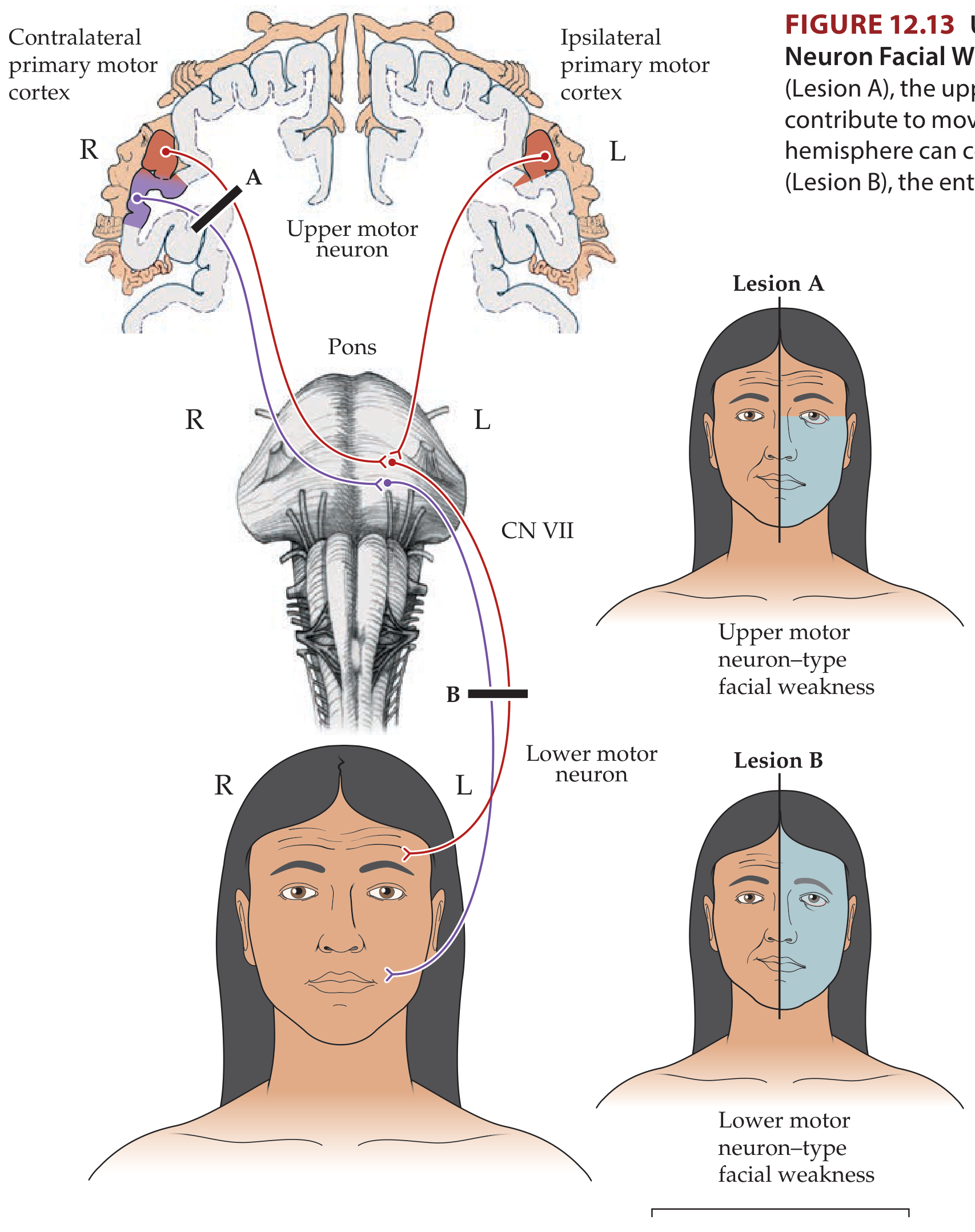
The facial nucleus (CN VII) in the pons receives bilateral corticobulbar input for the upper face (forehead, orbicularis oculi) - fibers come from both the ipsilateral and contralateral motor cortices. However, the lower face receives only contralateral UMN input. This bilateral supply to the upper face is the basis of the classic UMN-sparing pattern.
Comparison Table
| Feature | UMN FNP | LMN FNP |
|---|---|---|
| Forehead sparing | YES - forehead spared (bilateral cortical input) | NO - entire ipsilateral face affected |
| Side of weakness | Contralateral to lesion | Ipsilateral to lesion |
| Orbicularis oculi | Mild weakness only (slightly wide palpebral fissure) | Severe weakness - eye cannot close (Bell's phenomenon visible) |
| Lower face | Weak (nasolabial fold flattening, asymmetric smile) | Weak (same) |
| Emotional vs. volitional | May dissociate - emotional smile more symmetric than voluntary smile | Both volitional and emotional movements equally affected |
| Taste | Preserved | May be lost (ipsilateral anterior 2/3 tongue) - if nerve lesion is proximal to chorda tympani |
| Lacrimation | Preserved | May be impaired (dry eye) - if proximal to greater superficial petrosal nerve |
| Hyperacusis | Absent | May be present (stapedius weakness) |
| Retroauricular pain | Absent | May be present (Bell's palsy) |
| Corneal exposure risk | Low | High |
Localizing Features
UMN FNP - Causes & Clues
- Lesion site: Cortex (face area of primary motor cortex) or corticobulbar tract above the facial nucleus in the pons
- Common causes: Stroke, brain tumor, MS
- Associated signs: Contralateral arm/hand weakness, sensory loss, aphasia, dysarthria - these "neighborhood effects" are KEY to identifying a UMN cause
- Reflexes: Corneal reflex intact or hyperactive; gag reflex intact
LMN FNP - Causes & Clues
- Lesion site: Facial nucleus in pons, OR the facial nerve anywhere along its course (posterior fossa, petrous canal, stylomastoid foramen, parotid)
- Common causes:
- Bell's palsy (idiopathic - most common overall)
- Herpes zoster oticus (Ramsay Hunt syndrome)
- Lyme disease
- Sarcoidosis
- HIV, carcinomatous meningitis
- Parotid tumor, acoustic neuroma
- Brainstem lesion (Foville syndrome: ipsilateral CN VI + VII palsy + contralateral hemiparesis)
- Associated signs: None if peripheral; brainstem signs (gaze palsy, Horner, ataxia) if nuclear/fascicular
Important Caveat
A very dense UMN lesion can occasionally mimic LMN by affecting all facial movements - this is rare but can mislead. Always look for associated neurological signs to confirm localization. As Plum and Posner notes, a patient with UMN palsy will typically show a much more symmetric smile when laughing spontaneously (emotional) than when asked to smile voluntarily - this emotional-volitional dissociation does not occur in LMN palsy.
Bell's Palsy (Prototypical LMN FNP)
- Acute onset, often preceded by retroauricular pain
- Complete unilateral LMN-type palsy (entire half of face, forehead included)
- May have: ipsilateral taste loss, hyperacusis, dry eye
- Treatment: Prednisolone 25 mg BD x 10 days (improves recovery from 63% to 83% at 3 months); antivirals add benefit in severe cases
- Prognosis: ~90% recover; ~10% have poor recovery; aberrant regeneration can cause synkinesis (jaw winking, crocodile tears)
Sources:
- Neuroanatomy through Clinical Cases, 3rd Ed., Fig. 12.13 and Section 12.3
- Goldman-Cecil Medicine, Section 388
- Bradley and Daroff's Neurology in Clinical Practice, Section 103
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
This is a shared conversation. Sign in to Orris to start your own chat.