PAD Medical management
"peripheral artery disease"[MeSH Terms] AND "drug therapy"[MeSH Terms]
"peripheral arterial disease"[MeSH Terms] AND management
Medical Management of Peripheral Arterial Disease (PAD)
1. Antithrombotic Therapy
Antiplatelet Agents
- Aspirin 75-325 mg/day - a COX-1 inhibitor, the most widely used agent
- Clopidogrel 75 mg/day - a P2Y12 receptor antagonist; in the CAPRIE trial, clopidogrel was superior to aspirin in symptomatic PAD patients (3.71% vs. 4.86% annual event rate). Clopidogrel is preferred in current smokers, as it has shown greater event reduction vs. aspirin in this group
- Ticagrelor 90 mg twice daily - In the EUCLID trial, ticagrelor showed similar benefit to clopidogrel monotherapy (HR 1.02); may have a role in poor clopidogrel metabolizers
Dual Antiplatelet Therapy (DAPT)
- DAPT (aspirin + P2Y12 antagonist) was NOT shown to reduce MACE more than aspirin alone in PAD in the CHARISMA trial, and increases bleeding risk
- Exception: In PAD patients with a prior MI, adding ticagrelor to low-dose aspirin reduced both MACE and major adverse limb events (MALE) in PEGASUS-TIMI 54
- DAPT is commonly used after peripheral endovascular interventions, though clear supporting trial data are limited
Low-Dose Oral Anticoagulation (Pathway Antithrombotic Strategy)
- Rivaroxaban 2.5 mg twice daily + aspirin is supported by two major trials:
- COMPASS trial: In 6,391 PAD patients, this combination reduced MACE (5.1% vs. 6.9%, p=0.005) and MALE (1.5% vs. 2.6%, HR 0.57) vs. aspirin alone
- VOYAGER-PAD trial: In 6,564 patients post-revascularization, rivaroxaban + aspirin reduced a composite of acute limb ischemia, major amputation, MI, stroke, and cardiovascular death (HR 0.85, p=0.009)
- A meta-analysis of both trials confirmed superiority of the combination over aspirin alone for cardiovascular and limb events
- Major bleeding was increased with rivaroxaban, though fatal/critical organ bleeding was not significantly different
- Recommendation: Aspirin + low-dose rivaroxaban is reasonable in patients without elevated bleeding risk; full-dose anticoagulation is NOT routinely recommended as benefit does not outweigh bleeding risk
Vorapaxar
- A PAR-1 (thrombin receptor) antagonist approved for reducing thrombotic cardiovascular events in patients with a history of MI or PAD
- Contraindicated in patients with prior intracranial hemorrhage due to increased major bleeding risk
2. Lipid-Lowering Therapy
- Target: LDL < 70 mg/dL
- Agents: Rosuvastatin 40 mg/day or simvastatin 80 mg/day (though simvastatin 80 mg carries myopathy risk)
- Statins reduce mortality, MACE, MALE, and improve symptomatic outcomes. They also have pleiotropic effects: improved endothelial function, smooth muscle proliferation inhibition, plaque stabilization, and reduced platelet aggregation
- A VA population-based study of 155,647 patients showed high-intensity statin at PAD diagnosis significantly reduced limb loss and mortality
- Add ezetimibe (reduces intestinal LDL absorption, proven to lower cardiovascular events)
- Add PCSK9 inhibitors (e.g., evolocumab, alirocumab) if LDL goal still not reached - these monoclonal antibodies upregulate hepatic LDL receptors and have demonstrated reduction in MACE and major adverse lower extremity events
3. Blood Pressure Control
- Primary goal: reduce MACE
- ACE inhibitors are preferred - in the HOPE trial, ramipril reduced MI, stroke, and cardiovascular death by 25% vs. placebo in PAD patients
- Angiotensin receptor blockers (ARBs) are an alternative - In ONTARGET, telmisartan showed similar efficacy to ramipril with less angioedema
- Target BP: SBP < 140 mmHg, DBP < 90 mmHg (lower targets increasingly supported by cardiology guidelines)
- Importantly: beta-blockers are NOT contraindicated in PAD and may be used for concurrent cardiac indications
4. Glycemic Control (Diabetic Patients)
- DM significantly accelerates PAD progression; severity of disease correlates with chronic glucose exposure
- HbA1c target: <7% recommended by Global Vascular Guidelines for CLTI; <8% suggested by IWGDF to avoid hypoglycemia - individualize based on patient factors
- SGLT2 inhibitors (e.g., empagliflozin, dapagliflozin): reduce cardiovascular mortality, heart failure, renal complications, MACE, and amputation
- GLP-1 receptor agonists (e.g., semaglutide, liraglutide): similar cardiovascular and renal benefits
- Tight glycemic control reduces microvascular complications short-term and macrovascular complications when sustained over decades
5. Symptom Management - Intermittent Claudication
Cilostazol
- Cilostazol 100 mg twice daily is a Class I recommendation (ACC/AHA) for intermittent claudication
- Mechanism: reversible PDE-IIIa inhibitor - causes vasodilation and inhibits platelet aggregation (increases cAMP in platelets and vascular smooth muscle)
- Based on a Cochrane review of 16 RCTs: significantly improves pain-free and maximum walking distance
- Key contraindication: Congestive heart failure of any severity (class effect of PDE3 inhibitors)
- Common side effects: headache, palpitations, diarrhea, dizziness (main reasons for noncompliance)
- Should NOT substitute for aspirin/clopidogrel in ACS patients with concurrent PAD
Pentoxifylline
- No longer recommended - removed from guidelines due to lack of demonstrated benefit
6. Smoking Cessation
- Assess smoking status at every visit
- Pharmacologic options (used alone or in combination):
- Varenicline (most effective)
- Bupropion
- Nicotine replacement therapy (patches, gum, lozenges)
- Intensive smoking cessation intervention (behavioral + pharmacologic) resulted in 21.3% vs. 6.8% success at 6 months compared with minimal intervention
7. Supervised Exercise Therapy
- A Cochrane review of 32 RCTs (1,835 IC patients): exercise improved both pain-free and maximum walking distance vs. placebo/usual care
- A meta-analysis of 25 RCTs: supervised treadmill exercise improved walking performance by ~180 m vs. no exercise
- Since 2017, CMS covers up to 36 sessions over 12 weeks for PAD patients with walking impairment
- Protocol: Minimum 45-60 minutes, 3 times/week for 12 weeks; intensity sufficient to elicit claudication
- Home-based walking is a reasonable alternative for those without access to supervised programs
Summary Table
| Domain | Agent/Intervention | Key Point |
|---|---|---|
| Antiplatelet | Aspirin 75-325 mg/day OR Clopidogrel 75 mg/day | SAPT for all symptomatic PAD |
| Antithrombotic | Rivaroxaban 2.5 mg BID + ASA | Reduces MACE and MALE (COMPASS, VOYAGER-PAD) |
| Lipid | High-intensity statin | LDL goal <70 mg/dL; add ezetimibe or PCSK9i if needed |
| BP control | ACE inhibitor (ramipril) or ARB | HOPE trial: 25% reduction in MI/stroke/CVD death |
| Claudication | Cilostazol 100 mg BID | Class I; contraindicated in CHF |
| Diabetes | SGLT2i or GLP-1 agonist | Reduces amputation and cardiovascular mortality |
| Lifestyle | Smoking cessation + exercise | Supervised exercise: 36 sessions/12 weeks (CMS-covered) |
Peripheral arterial disease medical management
Peripheral Arterial Disease - Medical Management
1. Antithrombotic Therapy
Single Antiplatelet Therapy (SAPT) - First Line for All Symptomatic PAD
| Agent | Dose | Notes |
|---|---|---|
| Aspirin | 75-325 mg/day | COX-1 inhibitor; most widely used |
| Clopidogrel | 75 mg/day | P2Y12 antagonist; preferred over aspirin in current smokers (CAPRIE trial: 3.71% vs. 4.86% annual event rate) |
| Ticagrelor | 90 mg BID | Similar efficacy to clopidogrel (EUCLID trial, HR 1.02); use in poor clopidogrel metabolizers |
- Asymptomatic PAD: SAPT reasonable if reduced ABI + low bleeding risk, given high prevalence of subclinical CAD
- USPSTF 2022 guidance against aspirin for primary prevention in the general population does not override clinical judgment in established PAD
Dual Antiplatelet Therapy (DAPT)
- Aspirin + clopidogrel: NOT superior to aspirin alone in PAD (CHARISMA trial) and increases bleeding
- Exception: Aspirin + ticagrelor in PAD patients with prior MI reduces MACE and MALE (PEGASUS-TIMI 54)
- Commonly used post-peripheral intervention, though RCT data are limited
Low-Dose Anticoagulation (Vascular Dose Strategy)
- Rivaroxaban 2.5 mg BID + aspirin (COMPASS trial):
- In 6,391 PAD patients: reduced MACE (5.1% vs. 6.9%, p=0.005) and MALE (HR 0.57)
- Rivaroxaban 2.5 mg BID + aspirin (VOYAGER-PAD trial):
- In 6,564 post-revascularization patients: reduced composite of ALI, major amputation, MI, stroke, CV death (HR 0.85, p=0.009)
- Major bleeding increased, but fatal/critical organ bleeding was not significantly different
- Recommended in patients without elevated bleeding risk; full-dose anticoagulation is NOT routinely recommended
Vorapaxar
- PAR-1 thrombin receptor antagonist; approved for PAD patients to reduce thrombotic CV events
- Contraindicated in prior intracranial hemorrhage
2. Lipid-Lowering Therapy
| Step | Drug | Mechanism |
|---|---|---|
| 1st line | Rosuvastatin 40 mg/day or Simvastatin 80 mg/day | HMG-CoA reductase inhibitor |
| Add-on | Ezetimibe | Reduces intestinal LDL absorption |
| Add-on | PCSK9 inhibitors (evolocumab, alirocumab) | Increase hepatic LDL receptors |
- Statins reduce mortality, MACE, MALE, and improve walking symptoms
- Pleiotropic effects: improved endothelial function, plaque stabilization, reduced platelet aggregation
- VA study (155,647 patients): high-intensity statin at PAD diagnosis significantly reduced limb loss and mortality
3. Blood Pressure Control
- Target: SBP < 140 mmHg, DBP < 90 mmHg (lower targets increasingly supported)
- ACE inhibitors are preferred:
- Ramipril: 25% reduction in MI, stroke, and CV death vs. placebo (HOPE trial, PAD subgroup)
- ARBs are an equivalent alternative:
- Telmisartan showed similar efficacy to ramipril with less angioedema (ONTARGET)
- Beta-blockers are NOT contraindicated in PAD
4. Glycemic Control (Diabetic Patients)
| Target | Guideline | Rationale |
|---|---|---|
| HbA1c < 7% | Global Vascular Guidelines (CLTI) | Standard target |
| HbA1c < 8% | IWGDF | Avoids hypoglycemia risk in high-risk patients |
- Individualize based on age, duration of DM, comorbidities, hypoglycemia risk
- SGLT2 inhibitors (empagliflozin, dapagliflozin): reduce CV mortality, heart failure, renal events, MACE, and amputation
- GLP-1 receptor agonists (semaglutide, liraglutide): reduce CV mortality and MACE
5. Symptom Management - Intermittent Claudication
Cilostazol (Class I Recommendation - ACC/AHA)
- Dose: 100 mg twice daily for a 3-month trial
- Mechanism: Reversible PDE-IIIa inhibitor → increases cAMP → vasodilation + antiplatelet effect
- Evidence: Cochrane review of 16 RCTs - significantly improves pain-free and maximum walking distance
- Contraindication: Heart failure of ANY severity (all PDE3 inhibitors)
- Side effects: Headache (most common), palpitations, diarrhea, dizziness
- Does NOT substitute for aspirin/clopidogrel in concurrent ACS
Pentoxifylline
- No longer recommended - removed from guidelines (lack of efficacy)
6. Smoking Cessation
- Associated with decreased mortality and improved amputation-free survival
- Assess at every visit; counsel + offer pharmacotherapy + refer to cessation program
- Intensive intervention: 21.3% vs. 6.8% success at 6 months vs. minimal intervention
| Agent | Notes |
|---|---|
| Varenicline | Most effective |
| Bupropion | Effective; second line |
| Nicotine replacement | Patches, gum, lozenges; can combine with above |
7. Supervised Exercise Therapy
- Most effective non-interventional treatment for claudication symptoms
- Cochrane review (32 RCTs, 1,835 patients): improved pain-free and maximum walking distance
- Meta-analysis (25 RCTs): supervised treadmill exercise improved walking by ~180 m vs. no exercise
- CMS-covered: up to 36 sessions over 12 weeks for PAD patients with walking impairment (since 2017)
- Protocol: 45-60 min, 3x/week, 12 weeks; intensity sufficient to elicit claudication symptoms
- Home-based walking: reasonable alternative if supervised therapy is inaccessible
8. Wound and Foot Care (CLTI Patients)
- Multidisciplinary approach: vascular surgeon, wound care specialists, podiatry, nutritionists
- Regular foot inspection; patient education on footwear and skin care
- Early referral for non-healing wounds
Quick Reference Summary
MACE Prevention:
├── SAPT: Aspirin 75-325 mg OR Clopidogrel 75 mg (preferred in smokers)
├── Consider: Rivaroxaban 2.5 mg BID + ASA (if low bleeding risk)
├── Statin: LDL goal <70 mg/dL (+ ezetimibe / PCSK9i if needed)
└── ACE inhibitor / ARB for BP control
Limb Symptom Relief (IC):
├── Supervised Exercise (36 sessions / 12 wk) - most effective
└── Cilostazol 100 mg BID (contraindicated in CHF)
Risk Factor Modification:
├── Smoking cessation (varenicline preferred)
├── Diabetes: SGLT2i or GLP-1 agonist (HbA1c <7-8%)
└── BP target: <140/90 mmHg
- 2024 ACC/AHA PAD Guideline - PMID 38743805
- 2024 ESC Guidelines for PAD and Aortic Diseases - PMID 39210722
- 2025 SVS Focused Update - Intermittent Claudication - PMID 40316185
Target hb in suspected Apmls Patient with hb 6
"acute promyelocytic leukemia" AND "transfusion" AND "hemoglobin"
"acute promyelocytic leukemia" AND "supportive care" AND coagulopathy
APL acute promyelocytic leukemia hemoglobin transfusion target guidelines 2024
https://emcrit.org/ibcc/apl
APL acute promyelocytic leukemia "hemoglobin" OR "haemoglobin" transfusion target "8" OR "9" OR "10" g/dL ELN guideline
Transfusion Target Hb in Suspected APL (with Hb 6 g/dL)
Short Answer
APL Is a Transfusion Emergency - Not Just for Anemia
- DIC (consumptive coagulopathy from release of procoagulant granule contents)
- Hyperfibrinolysis (primary fibrinolysis driven by leukemic cells)
- Resulting in life-threatening hemorrhage - most commonly intracranial (65%) or pulmonary hemorrhage (32%)
Full Transfusion Targets in Suspected APL
| Product | Target | Why |
|---|---|---|
| pRBCs | Hb ≥ 8-9 g/dL | Liberal target given hemorrhage risk; NCCN uses 8-10 g/dL for symptomatic leukemia anemia |
| Platelets | > 30,000-50,000/mm³ | Maintain >50,000 actively; ELN guideline minimum is >30,000 |
| Fibrinogen | > 150 mg/dL | Most critical target - give 10 units cryoprecipitate PRN; ELN minimum is >100-150 mg/dL |
| FFP/INR | INR < 1.5-2 | ELN recommends <1.5 (may be difficult to achieve) |
| Vitamin K | Give empirically | If any possibility of vitamin K deficiency |
For your patient with Hb 6 g/dL: Transfuse 2 units pRBCs to bring Hb to ≥ 8 g/dL, and simultaneously check and aggressively correct platelets, fibrinogen, and INR.
Why a More Liberal Hb Target is Used in APL
- Active or impending hemorrhage - even without overt bleeding, these patients are in a coagulopathic state
- NCCN guidelines for leukemia-related anemia allow 8-10 g/dL if symptomatic
- Maintaining higher Hb provides a buffer against sudden blood loss from hemorrhagic complications
- Anemia itself can worsen tissue hypoxia in the context of shock from hemorrhage
What Else Must Be Done Immediately (Even Before Diagnosis Confirmed)
- Start ATRA immediately on clinical/morphological suspicion (45 mg/m²/day in 2 divided doses) - do NOT wait for genetic confirmation. ATRA reduces the severity of DIC
- Stop all anticoagulants and antiplatelets
- Avoid invasive procedures - prefer PICC over central line
- Monitor CBC, PT, aPTT, fibrinogen, D-dimer q6-12 hours until coagulopathy resolves
- Daily D-dimer throughout hospitalization
- Baseline Echo + ECG (required before starting arsenic trioxide/ATO)
- Correct electrolytes (Mg, K) if starting ATO
Key Principle
In APL, fibrinogen correction (cryoprecipitate) and platelet support are more urgently life-saving than the Hb alone. A patient with Hb 6 who has fibrinogen 80 mg/dL is at far greater risk from intracranial hemorrhage than from anemia. Both must be corrected, but fibrinogen has priority.
Hyperthyroidism treatment
"hyperthyroidism"[MeSH Terms] AND "therapy"[MeSH Terms]
"hyperthyroidism" AND "guidelines" AND "antithyroid"
Hyperthyroidism - Treatment
Overview of Treatment Modalities
| Modality | Mechanism | Best for |
|---|---|---|
| Antithyroid drugs (ATDs) | Inhibit thyroid hormone synthesis | Young patients, mild-moderate disease, pregnancy, pre-op/pre-RAI |
| Radioactive iodine (RAI / ¹³¹I) | Destroys thyroid follicular cells | Persistent Graves', toxic nodular goiter, older patients |
| Surgery (thyroidectomy) | Removes gland tissue | Large goiters, suspicious nodules, RAI contraindicated, patient preference |
Treatment Decision Flowchart
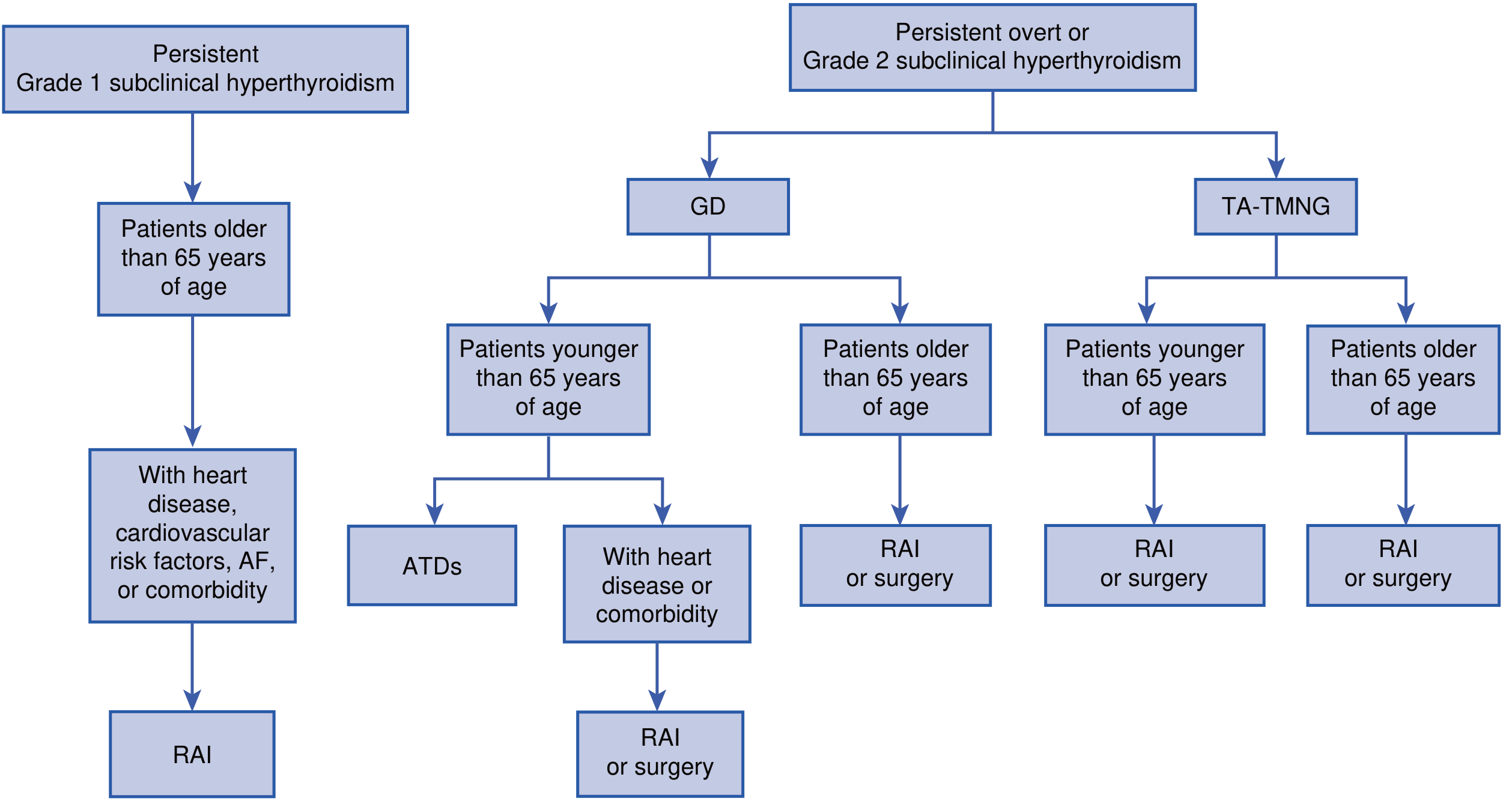
- Graves' disease (GD) + age < 65: ATDs first; RAI or surgery if comorbidity exists
- Graves' disease (GD) + age > 65: RAI or surgery (definitive)
- Toxic adenoma or toxic multinodular goiter (TA-TMNG): RAI or surgery regardless of age
- Grade 1 subclinical hyperthyroidism + age > 65 with cardiovascular risk/AF: RAI
1. Antithyroid Drugs (Thioamides)
Methimazole vs. Propylthiouracil (PTU)
| Feature | Methimazole | PTU |
|---|---|---|
| Preferred agent | Yes - in most situations | Only in specific indications |
| Mechanism | Inhibits TPO → blocks iodination and coupling of T3/T4 | Same + also blocks T4→T3 peripheral conversion |
| Dosing | Once daily (after euthyroid) - better adherence | Every 6-8 h (divided doses throughout) |
| Half-life | 6 hours | 90 minutes |
| Hepatotoxicity | Less severe | Can cause fatal acute liver failure (FDA restricted) |
| Teratogenicity | Aplasia cutis, choanal atresia, TEF fistula (methimazole embryopathy) | Safer in 1st trimester |
| FDA indications for PTU only | - | 1st trimester pregnancy, thyroid storm, minor adverse reaction to methimazole |
Dosing Regimen
- Initial: 10-20 mg every 12 h (or 20-40 mg single dose for mild-moderate disease)
- Maintenance (titration): 2.5-10 mg once daily
- Block-replace regimen: fixed high dose + add LT4 to prevent hypothyroidism
- Initial: 100-200 mg every 6-8 h
- Maintenance: 50-150 mg once daily
Monitoring
- Thyroid function tests (free T4 preferred over TSH initially) at 4-6 weeks
- Euthyroidism typically achieved in 6-8 weeks
- TSH may remain suppressed for months - use free T4 as primary monitor early
- Titration regimen preferred (lower doses; monitors spontaneous remission)
Duration and Remission
- Treat for 12-18 months for maximum remission rates
- Remission rates: 30-60% (titration regimen)
- Relapse risk is higher in: young patients, males, smokers, large goiters, high TRAb, severe hyperthyroidism
- If relapsed: prolonged low-dose therapy for up to 10 years or switch to definitive therapy
Adverse Effects
| Effect | Details |
|---|---|
| Minor (1-5%): rash, urticaria, fever, arthralgia | May switch to alternative ATD or treat with antihistamine |
| Agranulocytosis | Sore throat + fever = STOP drug immediately, check WBC + differential |
| Hepatotoxicity | PTU >> methimazole; stop if transaminases >2-3x ULN |
2. Radioactive Iodine (RAI / ¹³¹I)
- Preferred treatment for most patients >21 years (especially in North America)
- Dose range: 370-555 MBq (10-15 mCi), or 80-120 μCi/g thyroid weight corrected for uptake
- Effect takes 6-12 weeks to achieve euthyroidism/hypothyroidism
- A second dose can be given 6 months later if insufficient response
- Hypothyroidism occurs in ~80% of patients → require lifelong LT4 replacement
Pre-RAI preparation:
- Stop methimazole 2-3 days before RAI (not to interfere with iodine uptake)
- May restart methimazole 3-7 days after RAI (tapering over 4-6 weeks)
- PTU requires longer washout before RAI (prolonged radioprotective effect)
- Avoid iodine-containing foods/contrast to maximize ¹³¹I uptake
- In elderly or cardiac patients: pretreat with ATDs until euthyroid before RAI
Contraindications to RAI:
- Absolute: Pregnancy, breast-feeding
- Relative: Active moderate-to-severe Graves' ophthalmopathy (can worsen eye disease, especially in smokers)
- If RAI given with ophthalmopathy: cover with prednisone 0.2-0.5 mg/kg/day, tapered over 6-12 weeks
After RAI:
- Avoid close prolonged contact with children/pregnant women for 5-7 days
- Annual thyroid function testing required (progressive hypothyroidism: ~10-20% year 1, then 5%/year)
- Patients can conceive safely 6 months after RAI
3. Surgery (Total or Near-Total Thyroidectomy)
Indications:
- Very large goiters / multinodular goiters with compressive symptoms
- Suspicion of thyroid malignancy
- Coexisting hyperparathyroidism
- RAI contraindicated (pregnancy, active severe ophthalmopathy)
- Patient preference (especially young patients)
- Relapse after ATDs who prefer surgery over RAI
Pre-operative preparation:
- Antithyroid drugs until euthyroid (~6 weeks)
- Potassium iodide (SSKI): 1-2 drops orally TID for 10-14 days before surgery
- Purpose: reduces vascularity of the gland, lowers risk of thyrotoxic crisis
- Alternative: Lugol's iodine 5 drops BID x 10-14 days
Complications:
- Bleeding, laryngeal edema
- Hypoparathyroidism (hypocalcemia)
- Recurrent laryngeal nerve damage (hoarseness)
- These are rare when performed by experienced surgeons
- ~80-90% will require lifelong LT4 replacement after near-total thyroidectomy
4. Adjunct Therapy - Beta Blockers
- Age ≥ 60 years
- Heart rate > 90 bpm
- Cardiovascular disease
- Thyrotoxic periodic paralysis
| Drug | Dose |
|---|---|
| Propranolol | 20-40 mg PO every 6 h |
| Atenolol / Metoprolol | 25-50 mg PO every 6-8 h |
| Esmolol | IV use in thyroid storm/ICU |
- Taper and withdraw as thyroid hormone levels normalize
- If beta blockers contraindicated (e.g., asthma): use diltiazem 90-120 mg TID-QID
Additional adjuncts:
- Cholestyramine (bile acid sequestrant): rapidly lowers T4 by increasing fecal excretion
- Barbiturates: accelerate T4 breakdown via hepatic enzyme induction
- Digoxin: may be needed for AF in thyrotoxicosis, but requires higher doses (increased clearance)
- Warfarin: requires lower doses when patient is thyrotoxic (enhanced catabolism of clotting factors)
- Anticoagulation: Consider in all patients with AF (CHA₂DS₂-VASc score); most revert to sinus rhythm after euthyroidism achieved
5. Iodide (Lugol's / SSKI)
- Mechanism: Inhibits iodination of tyrosines (Wolff-Chaikoff effect) + blocks hormone release from thyroglobulin
- Wolff-Chaikoff effect lasts only a few days (escape occurs)
- Uses:
- Pre-operative preparation (reduces gland vascularity)
- Thyroid storm
- NOT suitable for long-term therapy
- Adverse effects: sore mouth/throat, tongue swelling, metallic taste, mucosal ulcerations
6. Special Situations
Toxic Multinodular Goiter / Toxic Adenoma
- RAI is the preferred treatment
- Very large goiters: surgery (subtotal thyroidectomy)
- Pre-treat with methimazole before definitive therapy
Subclinical Hyperthyroidism
- Grade 1 (TSH 0.1-0.4 mU/L): Treatment NOT recommended in asymptomatic young/premenopausal women
- Grade 2 (TSH < 0.1 mU/L) or older patients with cardiac risk: Treat (RAI or ATDs)
- LT4 suppression therapy: only justified in high-risk thyroid cancer patients
Pregnancy
| Trimester | Preferred Drug | Rationale |
|---|---|---|
| 1st trimester | PTU | Methimazole causes embryopathy (aplasia cutis, choanal atresia) |
| 2nd-3rd trimester | Switch to methimazole | PTU hepatotoxicity risk; convert at 15-20 mg PTU : 1 mg MMI |
| All trimesters | Target free T4 at/above upper reference range | Avoid fetal hypothyroidism |
| Last trimester | May stop if euthyroid on low dose | TRAb levels naturally decline |
- RAI is absolutely contraindicated in pregnancy and breast-feeding
- Breast-feeding is safe with low doses of ATDs
7. Thyroid Storm (Thyrotoxic Crisis)
| Drug | Dose | Purpose |
|---|---|---|
| PTU | 600 mg loading, then 200-250 mg q4h | Blocks synthesis + T4→T3 conversion (preferred over MMI in storm) |
| Lugol's iodine / SSKI | Start 1 hour AFTER PTU | Blocks hormone release (Wolff-Chaikoff); do NOT give before PTU |
| Propranolol | 60-80 mg PO q4h or IV esmolol | Controls adrenergic symptoms |
| Hydrocortisone | 100 mg IV q8h | Blocks T4→T3 conversion; treats relative adrenal insufficiency |
| Cooling measures | Paracetamol (NOT aspirin) | Aspirin displaces T4 from binding proteins |
| Treat precipitant | Antibiotics, fluids, etc. | Infection is most common precipitant |
Quick Reference Summary
Graves' Disease:
Young, mild disease → ATDs (methimazole x 12-18 months)
Older / cardiac disease → RAI (definitive)
Large goiter / malignancy suspicion → Surgery
Pregnancy (T1) → PTU → switch to methimazole T2/T3
Toxic Nodular → RAI or Surgery
Symptom Control → Beta blocker (propranolol/atenolol)
Pre-surgery → ATD to euthyroid + SSKI x 10-14 days
Pre-RAI → Stop MMI 2-3 days before; restart 3-7 days after
Thyroid Storm → PTU + Iodide (1hr later) + Propranolol + Hydrocortisone
Hyperthyroidism
Hyperthyroidism
Definition
Causes and Classification
Primary Hyperthyroidism (↑T3/T4, ↓TSH, ↑Radioiodine uptake)
| Cause | Key Features |
|---|---|
| Graves' disease | Most common (80%); autoimmune; diffuse goiter + ophthalmopathy |
| Toxic multinodular goiter (TMNG) | Elderly women; autonomous nodules; no eye signs |
| Toxic adenoma | Single hot nodule; suppresses rest of gland |
| TSH-secreting pituitary adenoma | Rare; TSH normal or elevated (inappropriate) |
| Gestational thyrotoxicosis | Driven by hCG cross-reacting with TSH receptor |
| Struma ovarii | Ectopic thyroid tissue in ovarian teratoma |
Thyrotoxicosis WITHOUT Hyperthyroidism (↓Radioiodine uptake)
| Cause | Mechanism |
|---|---|
| Subacute (de Quervain's) thyroiditis | Destructive - viral; painful; self-limited |
| Silent / postpartum thyroiditis | Painless destructive; autoimmune |
| Drug-induced | Amiodarone, cytokines, tyrosine kinase inhibitors, immune checkpoint inhibitors |
| Thyrotoxicosis factitia | Exogenous thyroid hormone ingestion |
| Radiation thyroiditis | After RAI therapy |
Graves' Disease - Pathogenesis
- Thyroid-stimulating immunoglobulins (TSI) / TRAb - present in ~90% of patients - bind and continuously stimulate the TSH receptor, mimicking TSH → unregulated T3/T4 production
- TPO antibodies and thyroglobulin antibodies also present in up to 80% of cases
- Genetic associations: CTLA4, PTPN22, IL2RA polymorphisms; TSHR gene variants; HLA-B8/DR3 in Caucasians
- Hyperthyroidism with diffuse goiter
- Infiltrative ophthalmopathy (exophthalmos)
- Infiltrative dermopathy (pretibial myxedema) - in minority
Clinical Features
General Symptoms and Signs (Any Cause of Thyrotoxicosis)
| System | Symptoms | Signs |
|---|---|---|
| General | Weight loss with increased appetite, heat intolerance, sweating, fatigue | Warm, moist skin, hyperpigmentation |
| Cardiovascular | Palpitations, dyspnea, chest pain | Tachycardia (sinus or AF), bounding pulse, widened pulse pressure, systolic hypertension, systolic flow murmur |
| Neurological | Hyperactivity, irritability, insomnia, anxiety | Fine tremor (best elicited at fingertips), proximal myopathy, hyperreflexia |
| GI | Diarrhea/hyperdefecation, nausea | Increased bowel frequency |
| Reproductive | Oligomenorrhea/amenorrhea, loss of libido | Gynecomastia in men |
| Skin/hair | Hair loss (up to 40%), nail changes | Onycholysis, palmar erythema |
| Musculoskeletal | Muscle weakness | Osteopenia (long-standing); mild hypercalcemia in ~20% |
| Eyes (non-specific) | - | Lid retraction, lid lag, staring appearance (sympathetic overactivity - any cause) |
Apathetic thyrotoxicosis: Seen in the elderly - presents with fatigue, weight loss, and AF, with minimal hyperadrenergic features. Easy to miss.
Graves'-Specific Features

- Occurs in ~1/3 of Graves' patients clinically; detectable by CT/US in most
- Mechanism: Activated T cells release IFN-γ, TNF, IL-1 → fibroblast proliferation → glycosaminoglycan accumulation → retro-orbital tissue expansion → proptosis
- TSH-R expressed in orbital tissue; IGF-1R signaling on orbital fibroblasts also implicated
- Earliest symptoms: gritty eye sensation, excess tearing, eye discomfort
- Advanced: proptosis (>22 mm), diplopia, corneal ulceration, optic nerve compression → vision loss
- Occurs in 10% of patients WITHOUT hyperthyroidism (euthyroid ophthalmopathy)
| Grade | Features |
|---|---|
| 0 | No signs or symptoms |
| 1 | Only signs (lid retraction/lag) |
| 2 | Soft tissue involvement (periorbital edema) |
| 3 | Proptosis (>22 mm) |
| 4 | Extraocular muscle involvement (diplopia) |
| 5 | Corneal involvement |
| 6 | Sight loss (optic neuropathy) |
- <5% of patients; almost always with moderate-to-severe ophthalmopathy
- Indurated, non-pitting purple/skin-colored lesions over anterior shin
- Contain large amounts of glycosaminoglycans (hyaluronic acid, chondroitin sulfate)
- Rare triad: digital clubbing, soft tissue swelling of hands/feet, periosteal reaction of distal metatarsals
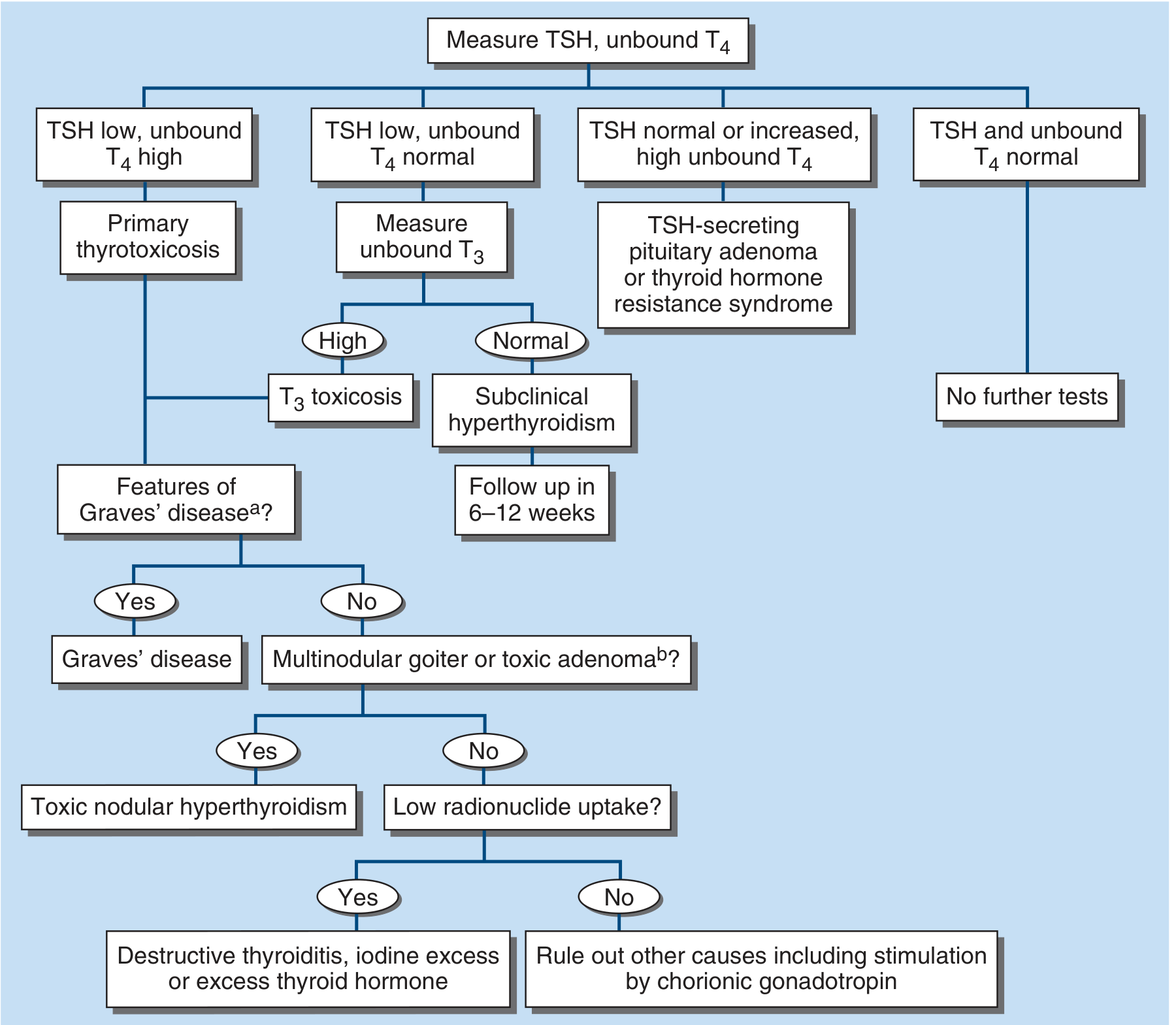
Diagnosis
Step 1 - Biochemical Confirmation
| Pattern | Interpretation |
|---|---|
| TSH ↓, free T4 ↑ | Primary thyrotoxicosis (most common) |
| TSH ↓, free T4 normal, free T3 ↑ | T3 thyrotoxicosis (2-5% of cases) |
| TSH normal/↑, free T4 ↑ | TSH-secreting pituitary adenoma or thyroid hormone resistance |
| TSH ↓, free T4 normal, free T3 normal | Subclinical hyperthyroidism |
TSH is the most sensitive biomarker - start here. A normal TSH effectively excludes thyrotoxicosis.
Step 2 - Diagnostic Algorithm
Step 3 - Distinguishing the Cause
| Test | Graves' | Toxic MNG/Adenoma | Destructive Thyroiditis |
|---|---|---|---|
| TRAb / TSI | Positive (~90%) | Negative | Negative |
| Radioiodine uptake | Diffusely high | Focally high ("hot" nodule) | Low/absent |
| Thyroid scan | Diffuse uniform uptake | Patchy or focal "hot" spot | Absent uptake |
| Color Doppler US | Increased blood flow ("thyroid inferno") | Variable | Decreased/absent flow |
| Anti-TPO antibodies | Often positive | Usually negative | May be positive (postpartum) |
| ESR / CRP | Normal | Normal | Elevated (subacute thyroiditis) |
Other Lab Abnormalities in Thyrotoxicosis
- ↑ Bilirubin, ↑ liver enzymes, ↑ ferritin
- Microcytic anemia, thrombocytopenia
- Mild hypercalcemia (~20%), hypercalciuria
- Elevated sex hormone-binding globulin
Cardiovascular Complications
- Atrial fibrillation: More common >50 years; up to 75% revert to sinus rhythm after achieving euthyroidism
- Heart failure: Especially with preexisting cardiac disease; high-output state progresses to failure
- Angina precipitation: High O₂ demand in setting of ischemic heart disease
- Hypokalemic periodic paralysis: Particularly in Asian males with thyrotoxicosis
- Thromboembolic events: Embolic stroke from AF; hyperthyroidism is a hypercoagulable state
Note: Warfarin requirement is decreased in thyrotoxicosis (increased clotting factor catabolism). Digoxin requires higher doses (increased clearance).
Thyroid Storm (Thyrotoxic Crisis)
- Thermoregulatory: High fever (often >38.5°C)
- Cardiovascular: Extreme tachycardia, AF, heart failure, hypotension
- CNS: Agitation, confusion, seizures, coma
- GI/hepatic: Nausea, vomiting, jaundice
- PTU 600 mg load then 200-250 mg q4h (preferred over MMI in storm - also blocks T4→T3)
- Wait 1 hour, then give Lugol's iodine/SSKI (prevents iodide being used as substrate)
- Propranolol 60-80 mg PO q4h or IV esmolol (controls adrenergic symptoms)
- Hydrocortisone 100 mg IV q8h (blocks T4→T3; treats relative adrenal insufficiency)
- Paracetamol for fever - NOT aspirin (aspirin displaces T4 from binding proteins)
- ICU admission + treat underlying precipitant
Treatment Summary (see previous detailed response)
| Modality | Indication |
|---|---|
| ATDs (methimazole/PTU) | First line; young patients; mild-moderate disease; pregnancy; pre-RAI/pre-op |
| Radioiodine (¹³¹I) | Persistent Graves'; toxic nodular goiter; older patients (North American preference) |
| Surgery | Large goiter; malignancy suspicion; RAI contraindicated; patient preference |
| Beta blockers | Symptomatic control while awaiting definitive therapy |
Subclinical Hyperthyroidism
- TSH ↓, normal free T4 and T3
- Grade 1: TSH 0.1-0.4 mU/L; usually from autonomous nodules; treat only if symptomatic or >65 years with cardiac risk
- Grade 2: TSH <0.1 mU/L; treat (atrial fibrillation risk, osteoporosis risk)
- Risk of AF is 3-fold higher, risk of fracture is 2-fold higher in overt subclinical hyperthyroidism
Normal ft4 22.9 t4 198.46 and TSH <0.0083
Thyroid Function Test Interpretation
The Results
| Test | Patient Value | Reference Range (Adults) | Status |
|---|---|---|---|
| Free T4 (fT4) | 22.9 pmol/L | 12-22 pmol/L (or 0.82-1.77 ng/dL) | ↑ Mildly elevated |
| Total T4 | 198.46 nmol/L (≈15.4 µg/dL) | 64-154 nmol/L (5-12.5 µg/dL adults) | ↑ Elevated |
| TSH | < 0.0083 mIU/L | 0.45-4.50 mIU/L (adults) | ↓↓ Profoundly suppressed |
Interpretation
Primary Diagnosis: Overt Primary Hyperthyroidism
- TSH < 0.0083 mIU/L is profoundly suppressed - well below the lower normal limit of 0.45 mIU/L. Modern sensitive TSH assays can detect down to ≤0.004-0.01 mIU/L; this value indicates near-total TSH suppression from excessive negative feedback by circulating thyroid hormones
- Free T4 of 22.9 pmol/L is above the upper reference limit (~12-22 pmol/L), confirming true overt hyperthyroidism - not just subclinical disease
- Total T4 of 198.46 nmol/L (~15.4 µg/dL) also exceeds the adult upper limit of ~154 nmol/L (12.5 µg/dL)
Important Note: "Normal" fT4?
- Even if fT4 22.9 is within your lab's range, a TSH of <0.0083 with ANY elevation in thyroid hormones is still diagnostic of overt hyperthyroidism
- The TSH is the most sensitive indicator - a profoundly suppressed TSH in the context of elevated total T4 confirms the diagnosis regardless of how fT4 is classified
Why is Total T4 Elevated More Than Free T4?
- Actual hyperthyroidism (both total and free T4 rise together - as here)
- Elevated TBG from: estrogens (OCP, pregnancy, HRT, tamoxifen), acute hepatitis, familial TBG excess
Differential Diagnosis of This Pattern
| Cause | Distinguishing Features |
|---|---|
| Graves' disease (most likely) | Diffuse goiter, ophthalmopathy, positive TRAb/TSI, diffusely high RAI uptake |
| Toxic multinodular goiter | Elderly, multinodular goiter on USS, focal hot spots on scan |
| Toxic adenoma | Solitary palpable nodule; single hot spot suppressing rest of gland |
| Subacute thyroiditis | Painful neck, raised ESR/CRP, low RAI uptake |
| Iodine-induced (amiodarone, contrast) | Drug history; T4 may be disproportionately elevated vs T3 (T4 thyrotoxicosis) |
| Exogenous T4 ingestion | Undetectable thyroglobulin, low RAI uptake |
| Postpartum thyroiditis | Postpartum, painless, may have positive anti-TPO |
Next Steps
- Check free T3 - in 2-5% of thyrotoxicosis, only T3 is elevated (T3 toxicosis); important to get baseline
- TRAb / TSI - confirm/exclude Graves' disease
- Anti-TPO antibodies - supports autoimmune etiology
- Thyroid ultrasound with Doppler - goiter size, nodules, vascularity ("thyroid inferno" in Graves')
- Radionuclide scan (¹²³I or ⁹⁹ᵐTc) if needed - differentiates high-uptake (Graves', toxic nodule) from low-uptake (thyroiditis, factitia) causes
- Clinical assessment - symptoms (palpitations, weight loss, tremor, heat intolerance), goiter, ophthalmopathy, HR, BP, tremor
One Important Caveat
Summary
TSH < 0.0083 + fT4 22.9 pmol/L + Total T4 198.46 nmol/L = Overt primary hyperthyroidism. This patient requires clinical evaluation to determine the underlying cause (most likely Graves' disease), followed by initiation of antithyroid therapy (methimazole or propylthiouracil), beta-blocker for symptomatic relief, and endocrinology referral.
If vanco traough level is high after stopping treatment when do we repeat trough level
vancomycin high trough after stopping when to recheck repeat level guidelines 2024
vancomycin supratherapeutic trough after stopping dose hold when to restart recheck half-life renal function
Vancomycin: High Trough After Stopping - When to Recheck
The Core Principle: Half-Lives
Vancomycin Half-Life by Renal Function
| CrCl (mL/min) | Approximate t½ | Time to Steady State (5 x t½) |
|---|---|---|
| > 120 mL/min | 4-6 hours | 20-30 hours |
| 90-120 mL/min | ~8 hours | ~40 hours |
| 60-90 mL/min | ~12 hours | ~60 hours |
| 30-60 mL/min | ~24 hours | 72-96 hours |
| 15-30 mL/min | ~48 hours | ~1 week |
| < 15 mL/min / Anuric | 72-96+ hours | 2+ weeks |
| Dialysis | Very prolonged | Dose by level only |
When to Recheck After a High Trough
Context 1: Treatment is CONTINUING - dose held due to high trough
| Trough Level | Action | When to Recheck |
|---|---|---|
| 21-25 mg/L | Reduce dose | Recheck at 36-48 h after dose adjustment |
| > 25 mg/L | Hold dose 24 h, reduce dose | Recheck 24 h after hold before restarting |
| > 30 mg/L | Stop, seek ID/micro advice | Recheck until safe range |
Context 2: Treatment is STOPPED/COMPLETED - high trough found at end of therapy
Wait 1-2 half-lives (until the level is estimated to be in/near the target range), then recheck to confirm clearance before considering any future redosing or assessing nephrotoxicity.
- Normal renal function (CrCl >60): Recheck in 24-48 hours
- Mild-moderate impairment (CrCl 30-60): Recheck in 48-72 hours
- Severe impairment (CrCl <30) or AKI: Recheck in 72-96 hours or longer
- ESRD/anuria: Level may take days to weeks to clear; recheck every 48-72h
The Calculation Approach (Pharmacokinetic Method)
C₂ = C₁ × e^(-ke × t)
Where:
C₁ = current high trough
C₂ = target acceptable level (e.g., 15 mg/L)
ke = elimination rate constant (0.693 / t½)
t = time to wait (solve for this)
- ke = 0.693/12 = 0.058/h
- t = ln(28/15) / 0.058 = 0.624 / 0.058 ≈ ~11 hours → recheck in ~12 hours
Key Points to Remember
- Renal function drives everything - always check current CrCl/creatinine before estimating when to recheck
- AKI worsens accumulation - if creatinine is rising, the drug is clearing slower than expected; recheck sooner rather than later and monitor closely
- "Improving" renal function after AKI can mean the drug clears faster - consider rechecking earlier
- Do NOT restart vancomycin until the level is confirmed to be in the safe range (typically < 15-20 mg/L depending on indication)
- Nephrotoxicity risk: Supratherapeutic troughs > 20 mg/L are associated with vancomycin-induced nephrotoxicity; monitor daily creatinine
- AUC-guided dosing (now preferred over trough-only per 2020 ASHP/IDSA/SIDP guidelines): AUC target 400-600 mg·h/L; if only trough monitoring is available, target trough is 10-20 mg/L depending on indication
Summary Table
| Renal Function | t½ | Recheck Interval After High Trough |
|---|---|---|
| Normal (CrCl >60) | 4-12 h | 24 hours |
| Moderate impairment (CrCl 30-60) | 12-24 h | 48 hours |
| Severe impairment (CrCl <30) | 24-48 h | 72 hours |
| ESRD/Anuric | >72-96 h | Every 48-72 h until cleared |
| Hemodialysis | Cleared by HD | Check pre-HD; redose based on level |
Practical rule of thumb: Wait ~1-2 half-lives (based on renal function) before rechecking. In normal renal function, recheck in 24 hours. In significant renal impairment, recheck in 48-72 hours.
In dengue hemorrhagic shock how fast can give blood transfusion
dengue hemorrhagic shock blood transfusion rate mL/kg WHO guidelines 2024
https://www.cdc.gov/dengue/media/pdfs/342849-A_Dengue_Pocket…
dengue hemorrhagic shock "packed red blood cells" OR "whole blood" transfusion "1-2 hours" OR "over 1 hour" rate WHO 2023 2024
Blood Transfusion in Dengue Hemorrhagic Shock
The Direct Answer
Packed Red Blood Cells (pRBCs): 5-10 mL/kg over 1-2 hours Fresh Whole Blood: 10-20 mL/kg over 1-2 hours
When is Blood Transfusion Indicated?
1st → IV Crystalloid resuscitation (isotonic saline/Ringer's lactate)
2nd → Colloid (albumin, Dextran-40) if refractory to crystalloids
3rd → Blood transfusion - ONLY when:
• Hematocrit FALLS (< 45% or drops significantly)
• Clinically significant/overt hemorrhage is confirmed
• Shock persists despite crystalloids + colloids
| Hematocrit | Interpretation | Action |
|---|---|---|
| Rising Hct (>45%) | Plasma leakage (capillary leak) - no true blood loss | Continue crystalloids/colloids |
| Falling Hct (<45%) | Overt hemorrhage - true blood loss | Transfuse blood |
| Rising Hct despite shock | Persistent capillary leak + occult bleeding | Colloid first, then reassess |
Transfusion Rates - Guidelines Summary
Packed Red Blood Cells (pRBCs)
| Guideline | Dose | Rate |
|---|---|---|
| CDC 2024 | 5-10 mL/kg | Not explicitly specified (implied over 1-2 h) |
| India National Guidelines 2023 | 5 mL/kg | Over 1 hour |
| WHO/PAHO | 5-10 mL/kg | Over 1-2 hours |
| WHO SEARO (Pediatric) | 5-10 mL/kg | Over 1-2 hours |
Fresh Whole Blood
| Guideline | Dose | Rate |
|---|---|---|
| CDC 2024 | 10-20 mL/kg | Not specified (1-2 h implied) |
| India National Guidelines 2023 | 10 mL/kg | Over 1 hour |
| WHO SEARO | 10 mL/kg | Over 1-2 hours |
- Whole blood: 1 unit over 1-2 hours
- pRBCs: 1 unit over 1 hour
Why This Specific Rate? (The Rationale)
- Too slow → patient remains in shock, organ damage progresses
- Too fast → fluid overload once capillary leak stops (reabsorption phase) → pulmonary edema, respiratory failure
What Products to Give (and NOT Give)
| Product | Recommendation |
|---|---|
| pRBCs | ✅ YES - 5-10 mL/kg over 1-2 h |
| Fresh whole blood | ✅ YES - 10-20 mL/kg over 1-2 h (if pRBCs unavailable) |
| Platelets | ❌ NOT routinely recommended (immune-mediated lysis destroys donor platelets) |
| Fresh Frozen Plasma (FFP) | ❌ NOT routinely recommended (CDC 2024) |
| Cryoprecipitate | Considered only in severe coagulopathy with fibrinogen depletion |
Note on platelets: Although not routinely recommended, some experts consider platelet transfusion for persistent severe life-threatening bleeding in patients who are PPI (proton pump inhibitor) responders with refractory thrombocytopenia.
Monitoring After Transfusion
- Vital signs (BP, HR, pulse pressure)
- Hematocrit - should stabilize or rise
- Urine output (target >1 mL/kg/hr)
- Signs of fluid overload (respiratory rate, SpO₂)
Full Shock Management Algorithm
Dengue with Shock
↓
IV Crystalloid: 20 mL/kg over 15-30 min
↓
Improved? → Step down fluids: 10→7→5→3→1.5 mL/kg/hr
↓
Not improved → Repeat crystalloid 20 mL/kg x2
↓
Not improved → Check ABCS:
A = Acidosis B = Bleeding (check Hct)
C = Calcium S = Blood Sugar
↓
Hct FALLING (<45%) = Overt bleeding
→ pRBCs 5-10 mL/kg OR Whole blood 10 mL/kg over 1-2 hrs
↓
Still not improved → Colloid (Dextran-40, albumin) 10 mL/kg
→ Inotropes if refractory
→ ICU / higher care
Ketamine infusion rate for icu intubated patient
ketamine infusion rate ICU intubated sedation analgesia mg/kg/hr SCCM guidelines 2024
ketamine continuous infusion ICU sedation "sub-dissociative" "analgosedation" dose range mg/kg/hr 2023 2024
Ketamine Infusion in ICU - Intubated/Mechanically Ventilated Patients
Dose by Indication (Key Distinction)
1. Analgesia / Analgosedation (Sub-Dissociative Dose)
| Parameter | Detail |
|---|---|
| Infusion rate | 0.05 - 0.5 mg/kg/hr |
| Typical starting dose | 0.1 - 0.2 mg/kg/hr |
| Effective range | 0.06 - 0.6 mg/kg/hr (doses <0.1 mg/kg/hr less likely to be effective) |
| Optional loading dose | 0.3-0.5 mg/kg IV over 15 min before infusion |
| Duration | 24-72 hours typical; can be longer |
| SCCM PADIS Guideline | 0.5 mg/kg IV bolus × 1, then 1-2 µg/kg/min (~0.06-0.12 mg/kg/hr) as opioid adjunct in post-surgical ICU patients |
Note: SCCM PADIS 2018 uses µg/kg/min: 1-2 µg/kg/min = 0.06-0.12 mg/kg/hr
2. Sedation (Dissociative/Anesthetic Dose)
| Parameter | Detail |
|---|---|
| Infusion rate | 0.5 - 5 mg/kg/hr |
| Starting dose | 0.5 - 1 mg/kg/hr |
| Titration target | RASS score (typically -2 to -3 for mechanically ventilated patients) |
| Maximum reported | Up to 5.2 mg/kg/hr in refractory cases |
| Real-world median (ICU study, n=95) | 1.3 mg/kg/hr (IQR 0.96-1.8) |
Full Dosing Reference Table
| Clinical Indication | Loading Dose (IV) | Infusion Rate |
|---|---|---|
| Analgesia adjunct (sub-dissociative) | 0.3-0.5 mg/kg over 15 min (optional) | 0.1-0.3 mg/kg/hr |
| Opioid-sparing (SCCM guideline) | 0.5 mg/kg × 1 | 1-2 µg/kg/min (0.06-0.12 mg/kg/hr) |
| Analgosedation (combined) | 0.5-1 mg/kg | 0.2-0.5 mg/kg/hr |
| Primary ICU sedation | 1-2 mg/kg | 0.5-2 mg/kg/hr |
| Refractory agitation/deep sedation | 1-2 mg/kg | Up to 4-5 mg/kg/hr |
| Alcohol withdrawal (ICU) | 0.3 mg/kg bolus (optional) | 0.15-0.3 mg/kg/hr |
| Status epilepticus (refractory) | 1-2 mg/kg | 0.5-5 mg/kg/hr (titrate to EEG burst suppression) |
| Procedural sedation (intubated) | 1-2 mg/kg IV | Short bolus-based; infusion 1-2 mg/kg/hr |
Why Ketamine is Attractive in the ICU
| Property | Clinical Benefit |
|---|---|
| Maintains airway reflexes | Safer than opioids/propofol alone |
| Sympathomimetic (↑HR, ↑BP via catecholamine release) | Preferred in haemodynamically unstable, septic shock patients |
| Bronchodilator | Ideal in asthma/bronchospasm on ventilator |
| No respiratory depression at sub-dissociative doses | Allows analgesia without over-sedation |
| Reduces opioid requirements | Less opioid-related ileus, delirium, tolerance |
| NMDA antagonist | Prevents central sensitization and opioid tolerance |
| Preserves protective reflexes | Safer during weaning |
Monitoring Parameters
| Parameter | Target/Action |
|---|---|
| RASS | -2 to 0 for light sedation; -3 to -5 for deep sedation (ARDS, etc.) |
| Blood pressure & HR | Monitor - ketamine can cause hypertension and tachycardia |
| Secretions | Can increase - have suction ready; consider glycopyrrolate if excessive |
| Emergence reactions / dysphoria | Less relevant in intubated patients but monitor on waking |
| Liver enzymes | Monitor with prolonged use (>5-7 days) |
| ICP (if neuroICU) | Historically avoided in raised ICP; current evidence suggests it is likely safe at analgesic doses |
Contraindications in ICU
| Contraindication | Reason |
|---|---|
| Uncontrolled hypertension | Ketamine further increases BP and HR |
| Active myocardial ischemia or severe CAD | Increased cardiac oxygen demand |
| Glaucoma | Raises intraocular pressure |
| Severe pulmonary hypertension | May worsen |
| Active psychosis | Worsens psychotomimetic effects (less relevant when intubated/sedated) |
Note on ICP: The historical contraindication in traumatic brain injury/raised ICP has been largely revised. Recent evidence suggests ketamine does not significantly increase ICP in mechanically ventilated patients already receiving appropriate sedation/analgesia.
Practical ICU Protocol Summary
Intubated ICU Patient - Ketamine Infusion
Goal: Analgesia adjunct (opioid-sparing)
→ Start: 0.1-0.2 mg/kg/hr
→ Range: 0.05-0.5 mg/kg/hr
→ Titrate: pain score (CPOT/BPS <3)
Goal: Primary sedation / analgosedation
→ Loading dose: 0.5-1 mg/kg IV over 5-15 min
→ Start infusion: 0.5-1 mg/kg/hr
→ Titrate: RASS target (usually -2 to -3)
→ Max: 4-5 mg/kg/hr
Monitor:
• HR, BP q1h
• RASS q2-4h
• Secretions
• LFTs if >5 days
Role for NAC infusion in acute liver failure and dose
"N-acetylcysteine" AND "acute liver failure" AND "non-acetaminophen"
N-acetylcysteine NAC infusion protocol dose acute liver failure acetaminophen non-acetaminophen AASLD guidelines 2023 2024
"N-acetylcysteine" AND "acute liver failure" AND survival
NAC "21 hour protocol" OR "72 hour" acetaminophen acute liver failure dose "150 mg/kg" "50 mg/kg" "100 mg/kg" IV infusion
N-Acetylcysteine (NAC) in Acute Liver Failure - Role and Dosing
Mechanism of Action
| Mechanism | Effect |
|---|---|
| Glutathione precursor | Replenishes depleted hepatic glutathione; scavenges toxic metabolites (NAPQI in acetaminophen toxicity) |
| Antioxidant | Directly neutralizes free radicals and reactive oxygen species |
| Anti-inflammatory | Reduces NF-κB activation and cytokine-driven hepatocyte injury |
| Improves microcirculation | Enhances hepatic and systemic oxygen delivery |
| Improves hemostasis | Supports coagulation factor synthesis |
| Vasodilatory | Increases hepatic blood flow via NO-mediated mechanisms |
Role in ALF - By Etiology
1. Acetaminophen (Paracetamol)-Induced ALF - ESTABLISHED, LEVEL I
- NAC is the definitive antidote - nearly 100% hepatoprotective if given within 8 hours of ingestion
- Within 12 hours: still prevents most liver injury
- Beyond 24 hours: reduces mortality and complications even in established liver failure
- Start immediately on suspicion - do NOT wait for acetaminophen levels
- Indication: any patient above the treatment line on the Rumack-Matthew nomogram
- Continue beyond 21-hour protocol if liver injury is progressing (elevated/rising INR, ALT, encephalopathy)
2. Non-Acetaminophen ALF (NA-ALF) - EVIDENCE-BASED, RECOMMENDED
- 173 patients with NA-ALF (DILI, viral, autoimmune, indeterminate)
- NAC vs. placebo (72-hour infusion protocol)
- Transplant-free survival: 40% (NAC) vs. 27% (placebo), p=0.043
- Benefit restricted to Grade I-II hepatic encephalopathy (West Haven)
- No benefit in Grade III-IV encephalopathy
Guideline Positions on NA-ALF:
| Guideline Body | Recommendation |
|---|---|
| EASL | ✅ NAC recommended in early-stage ALF of all causes as standard of care |
| AASLD | ✅ NAC may improve survival in early HE; recommended in DILI-induced ALF and when acetaminophen ingestion possible |
| INASL (India) | ✅ NAC recommended IV in all NA-ALF patients |
| AGA (2017) | ⚠️ NAC in NA-ALF should be limited to clinical trials only (controversial) |
Dosing Protocols
Standard 21-Hour IV Protocol (Acetaminophen ALF - Primary)
| Bag | Dose | Volume (D5W or NS) | Duration | Rate |
|---|---|---|---|---|
| Bag 1 (Loading) | 150 mg/kg | 200 mL 5% dextrose | Over 60 min | ~12.5 mg/kg/min equivalent |
| Bag 2 (Maintenance 1) | 50 mg/kg | 500 mL 5% dextrose | Over 4 hours | 12.5 mg/kg/hr |
| Bag 3 (Maintenance 2) | 100 mg/kg | 1000 mL 5% dextrose | Over 16 hours | 6.25 mg/kg/hr |
| Total | 300 mg/kg | - | 21 hours | - |
Max weight cap: Dose calculated on actual body weight up to 100 kg maximum
Children < 20 kg: Use reduced dextrose volumes (3 mL/kg, 7 mL/kg, 14 mL/kg for bags 1, 2, 3 respectively)
Extended Protocol - When to Continue Beyond 21 Hours
- Acetaminophen still detectable in serum
- INR > 1.5
- ALT/AST > 50 IU/L (or not declining toward 50% of peak)
- Ongoing encephalopathy
- Liver injury still progressing
72-Hour Protocol for Non-Acetaminophen ALF (Lee et al. Regimen)
| Phase | Dose | Duration | Rate |
|---|---|---|---|
| Loading | 150 mg/kg | 1 hour | 150 mg/kg/hr |
| Maintenance 1 | 12.5 mg/kg/hr × 4 hours | 4 hours | 12.5 mg/kg/hr |
| Maintenance 2 | 6.25 mg/kg/hr × 67 hours | 67 hours | 6.25 mg/kg/hr |
| Total duration | 72 hours |
72-Hour Oral Protocol (Alternative - Only if IV not feasible)
| Phase | Dose | Frequency |
|---|---|---|
| Loading | 140 mg/kg orally/NGT | Once |
| Maintenance | 70 mg/kg orally | Every 4 hours × 17 doses |
| Total | 1330 mg/kg over 72 hours |
- Dilute to 5% solution; mix with soft drink/juice for palatability
- Re-administer any vomited dose
- IV route is strongly preferred in ALF (vomiting, encephalopathy, GI bleeding make oral unreliable)
Emerging: 2-Bag Simplified Protocol (Growing Use in US)
| Bag | Dose | Duration |
|---|---|---|
| Bag 1 | 150 mg/kg | Over 1 hour |
| Bag 2 | 150 mg/kg | Over 20 hours |
| Total | 300 mg/kg / 21 hours | Same total dose |
- Fewer medication errors (27% → 11% error rate in studies)
- Similar efficacy and adverse event profile
- Not yet universally adopted but gaining acceptance
Criteria to STOP NAC (After Standard Protocol)
- Serum acetaminophen level is undetectable
- INR ≤ 1.5
- ALT/AST < 50 IU/L OR declining toward 50% of peak
- No encephalopathy
- Clinical improvement
Adverse Effects of IV NAC
| Effect | Frequency | Management |
|---|---|---|
| Anaphylactoid reaction (flushing, urticaria, angioedema) | ~15-20% | Slow infusion rate; antihistamine; temporary hold; usually with loading dose |
| Nausea/vomiting | Common (especially oral) | Antiemetics |
| Hypotension | Rare | Supportive; slow infusion |
| Bronchospasm | Rare | Bronchodilators; hold infusion |
Anaphylactoid reactions are not true IgE-mediated anaphylaxis - NAC can be restarted at slower rate after reaction resolves. They are most common with the rapid loading dose (15-minute bag 1 infusion increased reactions vs. 1-hour infusion).
Summary Quick Reference
ACETAMINOPHEN ALF:
→ IV NAC: 150 mg/kg/1h → 50 mg/kg/4h → 100 mg/kg/16h
→ Total: 300 mg/kg over 21 hours
→ Extend if INR >1.5, ALT not normalizing, ongoing encephalopathy
→ Start immediately - do NOT wait for levels
NON-ACETAMINOPHEN ALF (DILI, viral, autoimmune, indeterminate):
→ Same IV protocol for 72 hours
→ Loading: 150 mg/kg/1h → 12.5 mg/kg/hr × 4h → 6.25 mg/kg/hr × 67h
→ Benefits ONLY in Grade I-II hepatic encephalopathy
→ EASL recommends for ALL causes; AASLD recommends for DILI + possible APAP
KEY POINT: IV route always preferred in ALF
Max weight for dosing = 100 kg
Extend beyond standard protocol if liver injury ongoing
In dengue hemorrhagic shock role of albumin infusion as colloid while ongoing dialysis for metabolic acidosis?
albumin colloid dengue hemorrhagic shock refractory AKI metabolic acidosis dialysis role guidelines 2024