Tell me about the cardiac biomarkers and how they are monitored to identify STE-ACS and NSTE-ACS
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cardiac biomarkers" AND "acute coronary syndrome"
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive, well-sourced material to write a detailed answer. Let me compose the full response.
Cardiac Biomarkers in ACS: STE-ACS vs. NSTE-ACS
What is ACS and How is it Classified?
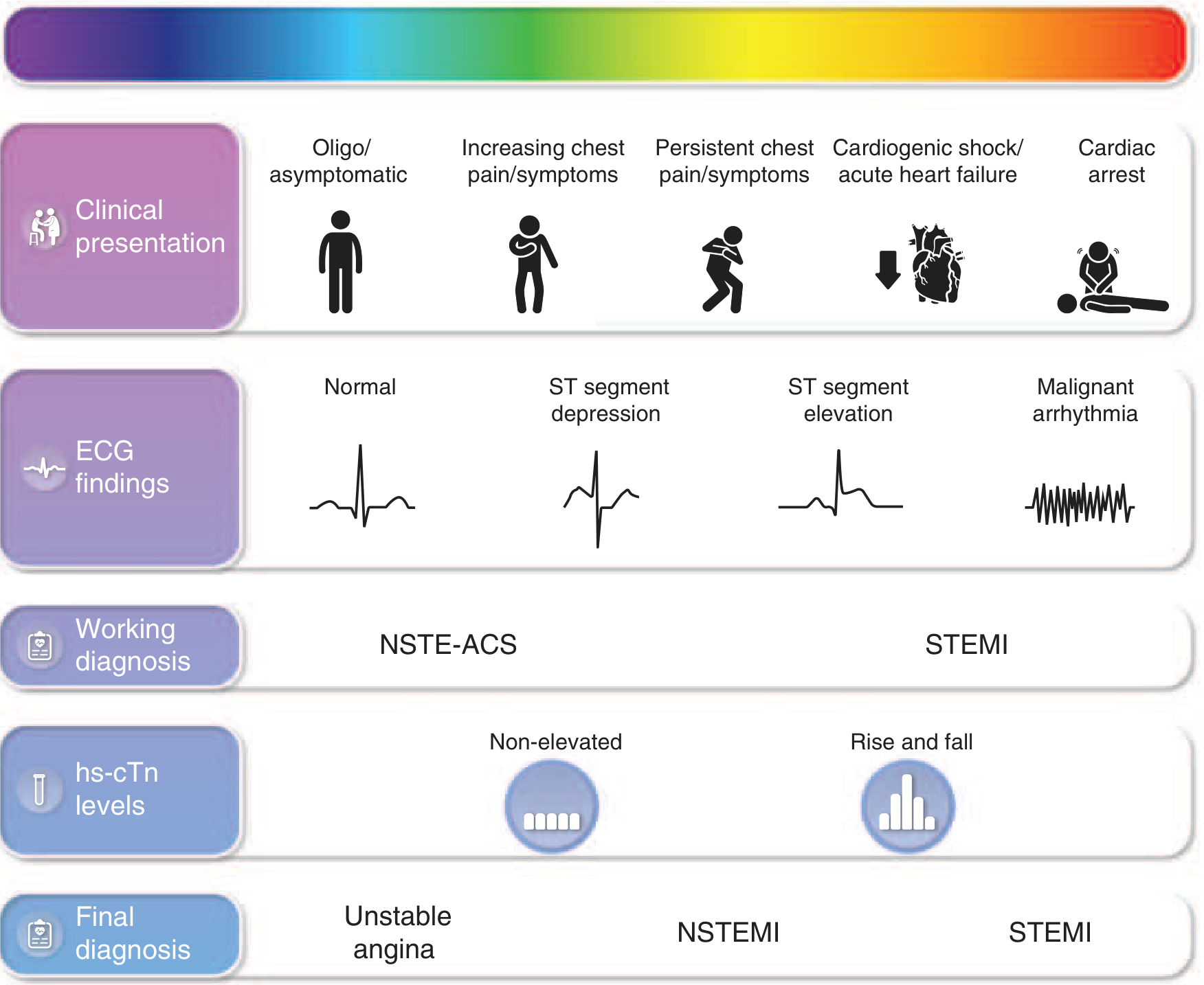
Acute Coronary Syndrome (ACS) is an umbrella term for conditions caused by acute myocardial ischemia, typically from plaque rupture or erosion with superimposed thrombus. It is classified into three subtypes based on ECG findings and biomarker results:
| ACS Subtype | ECG | Troponin | Key Feature |
|---|---|---|---|
| STEMI (STE-ACS) | ST-segment elevation | Elevated (rise & fall) | Complete coronary occlusion; full-thickness infarct |
| NSTEMI (NSTE-ACS) | No ST elevation; ST depression or T-wave changes | Elevated | Partial occlusion; subendocardial infarct |
| Unstable Angina (NSTE-ACS) | No ST elevation; may be normal | Normal | No myonecrosis; ischemia without cell death |
The working diagnosis at presentation is based on the ECG (STEMI vs. NSTE-ACS), while the final diagnosis between NSTEMI and unstable angina depends on whether troponin is elevated. This is illustrated clearly in the spectrum diagram from Harrison's 22nd Edition:
The Key Cardiac Biomarkers
1. Cardiac Troponin (cTnI and cTnT) - The Primary Biomarker
Troponin is the regulatory protein complex in myocardial sarcomeres. Its three subunits - troponin I (TnI), troponin T (TnT), and troponin C (TnC) - coordinate actin-myosin interactions. The cardiac isoforms (cTnI and cTnT) are encoded by different genes than the skeletal muscle isoforms, making them highly cardiac-specific. Notably, cTnI has an additional 31 amino acid N-terminal extension unique to cardiac muscle.
Kinetics after MI:
- Detectable in blood: 2-4 hours after onset of chest pain
- Peak: ~48 hours (or earlier with reperfusion due to rapid washout)
- Returns to normal: 7-10 days (TnI: 5-9 days; TnT: up to 10 days)
This prolonged elevation window allows diagnosis of MI even days after the acute event - something CK-MB cannot offer.
Diagnostic threshold: Any cTn value above the 99th percentile of the upper reference limit (URL) in a reference population indicates myocardial injury. The 4th Universal Definition of MI (Thygesen et al., 2018) requires:
- At least one elevated cTn result (>99th percentile)
- Evidence of a rising and/or falling pattern to confirm an acute (versus chronic) etiology
- Clinical, ECG, or imaging evidence of ischemia to confirm the MI diagnosis
cTnI vs. cTnT: cTnI assays are preferred by many labs because they are exclusively specific to cardiac tissue - cTnT can be elevated in renal failure without MI.
2. High-Sensitivity Cardiac Troponin (hs-cTn) - The Modern Standard
High-sensitivity assays are now preferred over conventional troponin assays. They can:
- Identify 90-100% of AMI patients at the time of ED arrival (albeit with variable specificity of 34-80% at the lowest cut point)
- Enable rapid rule-out protocols using serial testing over as little as 1-2 hours
- Provide a greater negative predictive value (>99% in patients presenting >2-3 hours after symptom onset with a single very low result)
Using hs-cTn, troponin should be measured:
- At presentation (time 0)
- Repeated at 1-3 hours (hs-cTn) or 3-6 hours (conventional troponin)
- Additional measurements beyond 3-6 hours if clinical suspicion persists
The key concept with hs-cTn is the delta (Δ) troponin - the change between serial samples. A rising and/or falling pattern distinguishes acute myocardial injury (ACS) from chronic stable elevation due to underlying structural heart disease, end-stage renal disease, or myocarditis.
3. CK-MB (Creatine Kinase-MB Isoform)
CK-MB was the gold standard for decades before troponin replaced it. It is an isozyme of creatine kinase found predominantly in cardiac muscle (the MB isoform).
Kinetics after MI:
- Rises: 2-4 hours
- Peaks: 24-48 hours
- Returns to normal: ~72 hours (3 days)
Because CK-MB normalizes within 3 days, it is still used in specific clinical scenarios - particularly to detect reinfarction (a second MI within 24-48 hours of the first), where troponin remains persistently elevated and cannot easily signal a new event. A >20% rise in CK-MB in this context suggests reinfarction. Adding CK-MB or myoglobin to cTn for routine ACS evaluation has not been shown to be beneficial.
4. Myoglobin
Myoglobin is a small oxygen-binding/transport protein found in both cardiac and skeletal muscle. Its small size allows for the earliest release from damaged cells.
Kinetics after MI:
- Rises: within 1-2 hours (the earliest of all biomarkers)
- Peaks: ~8 hours
- Returns to normal: within 24 hours
Limitation: Myoglobin cannot distinguish cardiac from skeletal muscle origin, so it cannot diagnose MI by itself. Its main clinical value is as a screening/rule-out tool: a negative myoglobin result early after symptom onset has a high negative predictive value for AMI. Positive results require further workup.
5. Other Biomarkers (Supporting Roles)
- BNP/NT-proBNP (B-type natriuretic peptide): Useful for assessing heart failure and LV dysfunction complicating ACS; used for risk stratification, not primary ACS diagnosis.
- D-dimer: Measured to help exclude pulmonary embolism as an alternative diagnosis in chest pain presentations.
- Lactate dehydrogenase (LDH): Historically used via the "flipped ratio" (LD1:LD2 > 0.75) at 36-48 hours, now largely replaced by troponin.
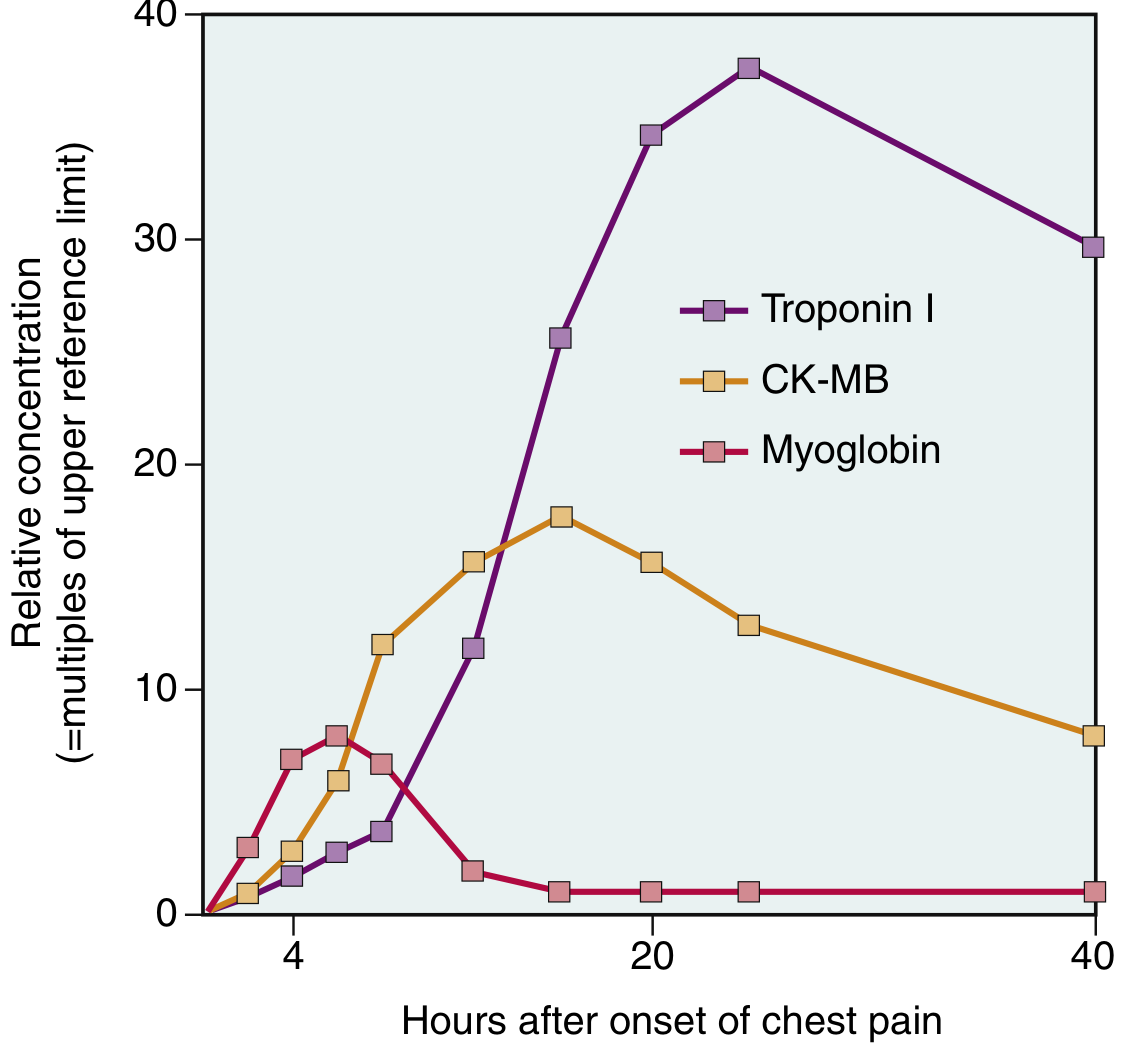
Biomarker Kinetics: Comparative Time Course
This graph from Robbins & Kumar Basic Pathology illustrates the relative concentrations of the three main biomarkers after MI:
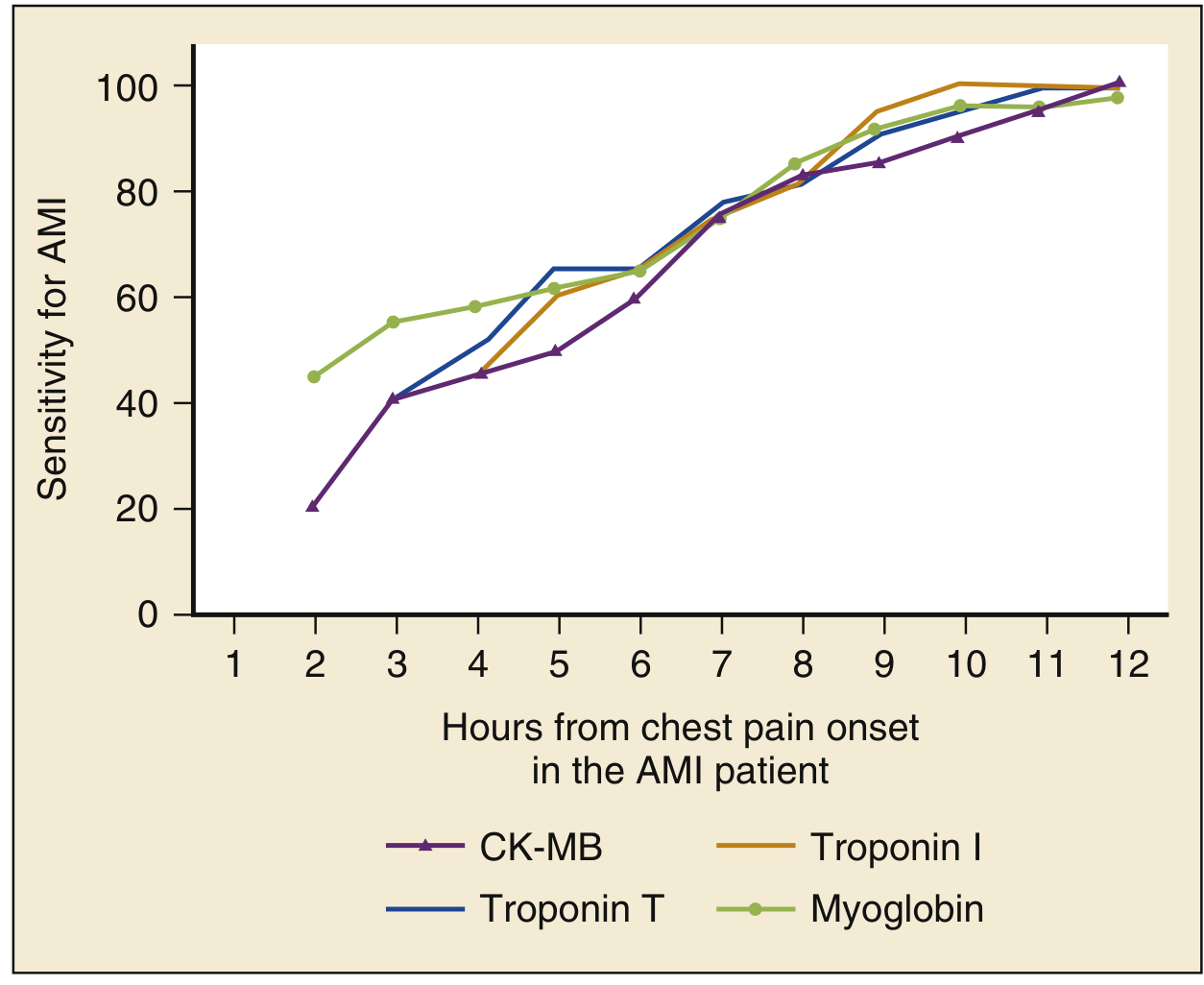
And this graph from Rosen's Emergency Medicine compares the sensitivity of each marker over time:
How Biomarkers Are Used to Differentiate STE-ACS vs. NSTE-ACS
STE-ACS (STEMI)
- ECG is diagnostic: New ST-segment elevation at the J point in ≥2 contiguous leads (≥0.1 mV in most leads; ≥0.2 mV in V2-V3 for men ≥40 years; ≥0.25 mV for men <40; ≥0.15 mV for women)
- Biomarkers are NOT required to initiate treatment: Patients with diagnostic ST-segment elevation do not need a serum biomarker result before being sent for reperfusion therapy
- Biomarkers confirm and quantify: Serial troponin measurements confirm the diagnosis and can estimate infarct size; the rise-and-fall pattern is characteristic (see the 4th Universal Definition criteria table below)
- Troponin typically shows a pronounced rise and fall pattern
NSTE-ACS (NSTEMI vs. Unstable Angina)
This is where biomarkers are the deciding factor. A patient with chest pain, no ST elevation, and:
- Elevated cTn (>99th percentile with rise/fall pattern) = NSTEMI
- Normal cTn on serial testing = Unstable Angina
ECG in NSTE-ACS may show ST-segment depression (in ~1/3 of patients), T-wave inversions (especially deep, ≥0.3 mV new inversions), or may be completely normal. In NSTE-ACS, ST depression may persist for days following NSTEMI.
The 4th Universal Definition of MI: cTn Criteria
From Henry's Clinical Diagnosis and Management by Laboratory Methods (based on Thygesen et al., 2018):
| Diagnosis | Criteria |
|---|---|
| Myocardial injury | Any cTn result >99th percentile of reference population |
| Acute myocardial injury | At least one elevated cTn + evidence of rise and/or fall |
| Acute MI (Types 1, 2, 3) | Acute myocardial injury + clinical, ECG, or imaging evidence of ischemia |
| MI Type 4a (post-PCI) | Within 48h: cTn >5× 99th percentile (or ≥20% increase if pre-procedurally elevated) + ischemic evidence |
| MI Type 5 (post-CABG) | Within 48h: cTn >10× 99th percentile (or ≥20% increase) + ischemic evidence |
| Reinfarction (within 28 days) | >20% increase in cTn over 3-6h from a previously elevated/stable value |
Diagnostic Pathway in the ED
The HEART pathway (Harrison's, 22nd Ed.) is a practical chest pain evaluation protocol:
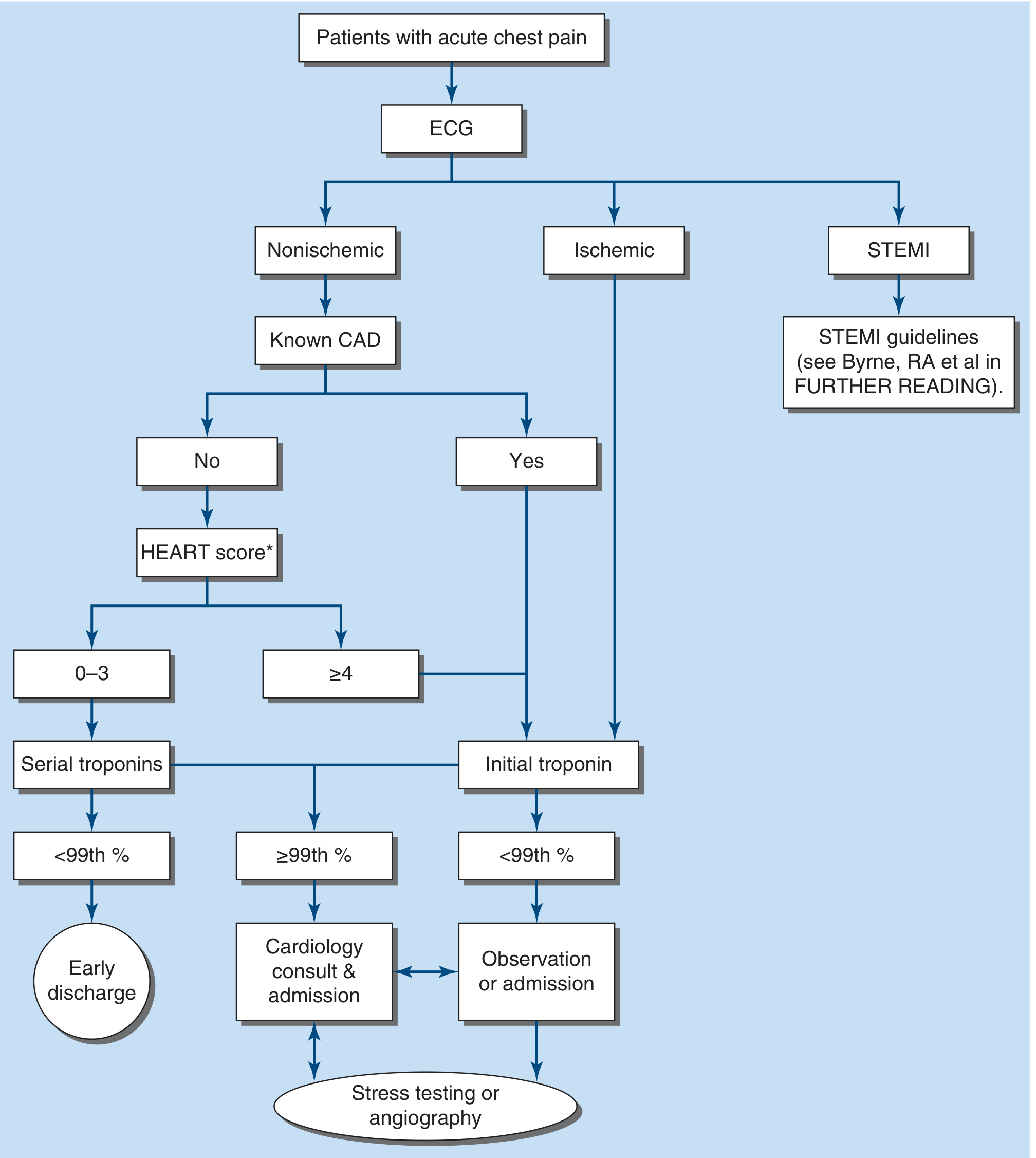
Key decision points:
- ECG is always obtained first and immediately
- STEMI identified → immediate reperfusion pathway (PCI target ≤90 min from first medical contact at PCI-capable center)
- No STEMI → HEART score applied (History, ECG, Age, Risk factors, Troponin)
- HEART 0-3: serial troponins; if <99th percentile → early discharge
- HEART ≥4: initial troponin; if ≥99th percentile → cardiology consult and admission
Important Caveats
- Troponin elevation does not always mean ACS. Many non-ACS conditions elevate troponin: myocarditis, pulmonary embolism, heart failure, sepsis, renal failure, cardiac contusion, Takotsubo cardiomyopathy. The dynamic pattern (acute rise/fall) and the clinical context are what point toward ACS.
- cTnT in renal failure: cTnT can be elevated in chronic kidney disease without MI; cTnI assays are more specific in this population.
- Myocardial injury vs. MI: Elevated troponin = myocardial injury. MI is only diagnosed when that injury is caused by ischemia (Type 1: plaque rupture; Type 2: supply-demand mismatch; Type 3: fatal MI presumed before biomarkers available).
- The incidence of STEMI is declining (due to better primary prevention), while NSTEMI incidence is rising - partly because hs-cTn assays detect smaller degrees of myonecrosis that older assays would have missed.
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapters 15 & 285
- Tintinalli's Emergency Medicine, Chapter 49
- Robbins & Kumar Basic Pathology
- Frameworks for Internal Medicine, Chapter 2
- Henry's Clinical Diagnosis and Management by Laboratory Methods, Chapters 6 & 19
- Sabiston Textbook of Surgery, Chapter on Cardiovascular Biomarkers
- Rosen's Emergency Medicine, Chapter 64
This is a shared conversation. Sign in to Orris to start your own chat.