Aflp
Reading File
Finding Sources
Searching PubMed
"acute fatty liver of pregnancy"
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of Acute Fatty Liver of Pregnancy (AFLP):
Acute Fatty Liver of Pregnancy (AFLP)
Definition & Epidemiology
AFLP is a form of microvesicular fatty liver disease unique to human gestation, presenting as an obstetric emergency that can progress to fulminant hepatic failure. It occurs in approximately 1 in 6,700-10,000 third-trimester pregnancies, though subclinical cases may go unrecognized.
Risk factors:
- Primiparity
- Multiple gestations (twins)
- Male fetus
- Low BMI (<20)
- Fetal LCHAD (long-chain 3-hydroxyacyl-CoA dehydrogenase) deficiency
Pathogenesis
The key mechanism involves a defect in fetal mitochondrial fatty acid oxidation (FAO), specifically mutations in the HADHA gene causing LCHAD deficiency. The affected fetus (homozygous) cannot oxidize long-chain fatty acids, which accumulate and are transferred to the heterozygous mother, overwhelming her hepatic processing capacity and causing lipid microvesicle deposition in hepatocytes. This explains the excess of male fetuses, since males are more commonly affected by recessive FAO disorders.
Renal injury in AFLP is multifactorial: hemodynamic changes similar to hepatorenal syndrome, thrombotic microangiopathy, tubular fatty acid accumulation, and co-existing preeclampsia all contribute.
Clinical Presentation
Timing: Usually 34-37 weeks gestation (rarely as early as 19-20 weeks or postpartum).
Symptoms:
- Nausea, vomiting, abdominal pain (early)
- Jaundice (common but not invariable)
- Pruritus (may overlap with intrahepatic cholestasis of pregnancy)
- Confusion/encephalopathy
- Polydipsia/polyuria (transient diabetes insipidus)
- Premature labor, vaginal bleeding, decreased fetal movement
Complications:
- Acute kidney injury (75% of cases; creatinine >1.5 mg/dL)
- Hypoglycemia (indicates severe synthetic dysfunction)
- DIC and coagulopathy
- Acute pancreatitis (~16%)
- Ascites, pleural effusion
- Respiratory failure
- ICU admission (~14%)
- Maternal mortality (~4%), stillbirth (~12%)
- Rare: myocardial infarction, pulmonary fat emboli
Diagnosis: Swansea Criteria
Diagnosis requires 6 or more of the following criteria in the absence of another explanation:
| Category | Criterion |
|---|---|
| Clinical | Vomiting |
| Abdominal pain | |
| Polydipsia/polyuria | |
| Encephalopathy | |
| Labs | Bilirubin >0.8 mg/dL |
| Hypoglycemia <70 mg/dL | |
| Uric acid >5.7 mg/dL | |
| Leukocytosis >11 x 10^9/L | |
| ALT/AST >42 U/L | |
| Ammonia >47 umol/L | |
| PT >14 s or APTT >34 s | |
| Other | Ascites or bright liver on ultrasound |
| Microvesicular steatosis on biopsy |
Modified from Knight et al., Gut 2008 - Comprehensive Clinical Nephrology, 7th ed.
Liver biopsy is usually not required but is pathognomonic when performed: microvesicular fat in zone 3 hepatocytes (surrounding central veins), sparing the periportal zone. Special stains (oil-red O on frozen sections, or electron microscopy) are needed to confirm, as H&E may appear nearly normal.
Differentiation from HELLP Syndrome
AFLP and HELLP syndrome overlap significantly. Key distinctions:
| Feature | AFLP | HELLP |
|---|---|---|
| Hypoglycemia | Prominent | Rare |
| Coagulopathy/DIC | Severe | Mild-moderate |
| Encephalopathy | Common | Less common |
| Renal failure | Very common | Less common |
| Transaminases | Moderate (~750 U/L) | Elevated |
| Hypertension | In ~21-64% | Defining feature |
| Fibrinogen | Low | Usually normal |
Note: Preeclampsia accompanies 21-64% of AFLP cases.
Management
- Early recognition - high clinical suspicion in any third-trimester patient with nausea, jaundice, coagulopathy
- Prompt delivery - the definitive treatment regardless of gestational age; condition remits after delivery
- Intensive care - ICU setting with multidisciplinary team (MFM, hepatology, nephrology, critical care)
- Supportive care:
- Aggressive correction of coagulopathy (blood products)
- Correction of hypoglycemia (concentrated glucose infusion)
- Hemodialysis for renal failure (dialysis needed in ~2%)
- Mechanical ventilation if needed
- Antibiotic therapy for infections
- Lactulose/bowel evacuation for hepatic encephalopathy
- Desmopressin (DDAVP) for diabetes insipidus
- Avoid heparin and antithrombin III despite DIC
- Emergency liver transplantation - rare but life-saving in refractory hepatic failure
- Neonatal screening - infants should be tested for LCHAD deficiency; may present with nonketotic hypoglycemia
Prognosis
- With prompt diagnosis and delivery: maternal survival approaches ~100%
- Perinatal mortality: <7%
- Most women recover completely with no residual hepatic or renal impairment
- Recurrence is documented, especially in women with LCHAD deficiency
- Genetic testing of mother, father, and child for the G1528C LCHAD mutation is recommended in all cases
Recent Evidence
A 2024 systematic review on plasmapheresis in AFLP (PMID: 39493711) examined its safety and efficacy as an adjunct treatment in severe cases, suggesting potential benefit in refractory disease - though prompt delivery remains the cornerstone.
Sources: Sleisenger & Fordtran's GI and Liver Disease; Creasy & Resnik's Maternal-Fetal Medicine; Comprehensive Clinical Nephrology, 7th ed.
How keto diet works
Finding Sources
Searching PubMed
"ketogenic diet" AND metabolism
Searching the Web
how ketogenic diet works mechanism ketosis physiology
Finding Sources
Reading Web Page
https://www.nature.com/articles/s41392-021-00831-w
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a thorough explanation of how the ketogenic diet works, grounded in biochemistry:
How the Ketogenic Diet Works
What It Is
The ketogenic diet (KD) is a high-fat, very-low-carbohydrate, moderate-protein diet. The typical macro breakdown is roughly:
- Fat: 70-80% of calories
- Protein: 15-20%
- Carbohydrates: <50 g/day (sometimes as low as 20 g/day)
This is the diet your body naturally mimics during prolonged fasting.
Step 1: Glycogen Depletion
When you drastically cut carbs, your body first burns through its glycogen stores:
- The liver holds ~100 g of glycogen, depleted within about 24 hours of carb restriction
- Muscle glycogen is used locally for exercise
Once glycogen runs out, blood glucose drops, insulin levels fall sharply, and glucagon rises. This hormonal shift is the trigger for everything that follows.
Step 2: Fat Mobilization
Low insulin removes the "brake" on fat tissue:
- Lipolysis in adipose tissue accelerates - triglycerides are broken down into free fatty acids (FFAs) and glycerol
- FFAs flood into the bloodstream and are taken up by the liver
- Glycerol enters gluconeogenesis to make a small amount of glucose (enough for tissues that still need it, like red blood cells)
Step 3: Ketogenesis in the Liver
This is the heart of how keto works. In liver mitochondria, the massive influx of fatty acids undergoes beta-oxidation, producing large amounts of acetyl-CoA. Normally, acetyl-CoA enters the TCA (Krebs) cycle by combining with oxaloacetate (OAA) - but here's the key bottleneck:
- High fatty acid oxidation lowers the NAD+/NADH ratio, which converts OAA to malate
- Low carbohydrate intake means OAA is being diverted to gluconeogenesis, not the TCA cycle
- Result: OAA becomes scarce, and acetyl-CoA cannot enter the TCA cycle efficiently
So instead, excess acetyl-CoA is converted to ketone bodies:
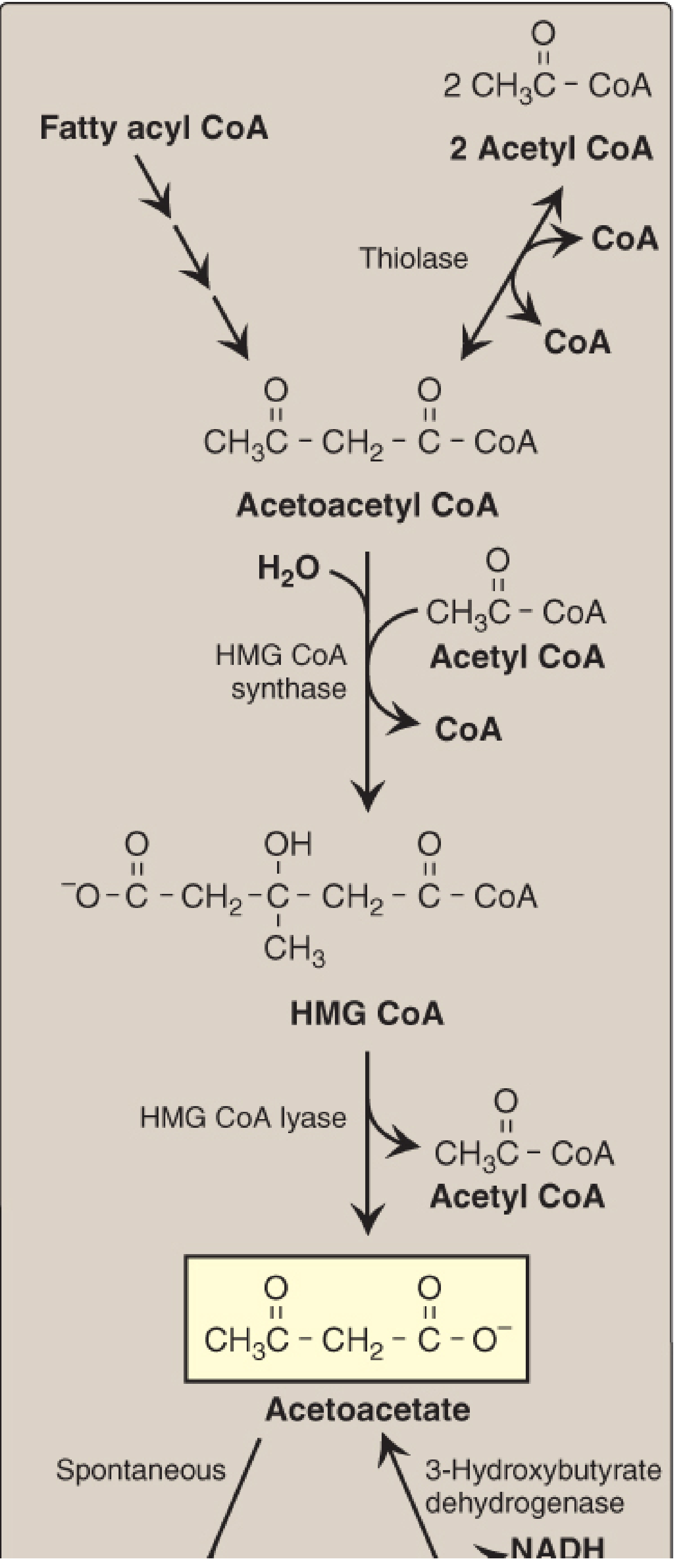
Ketone body synthesis (ketogenesis) in the liver - Lippincott's Biochemistry, 8th ed.
The three ketone bodies produced are:
- Acetoacetate - the primary ketone body
- 3-Hydroxybutyrate (beta-hydroxybutyrate, BHB) - the most abundant in blood; a stable transport form
- Acetone - spontaneously formed from acetoacetate; volatile, exhaled through breath (the "keto breath")
The rate-limiting enzyme in this process is HMG-CoA synthase, found in significant quantities only in the liver.
Step 4: Ketone Bodies as Fuel (Ketolysis)
The liver produces ketone bodies but cannot use them itself (it lacks the enzyme thiophorase). They are exported to peripheral tissues:
- Brain - the primary beneficiary; normally 100% glucose-dependent, but adapts to use BHB for ~70% of its energy needs during ketosis
- Heart and skeletal muscle - efficiently oxidize BHB, actually preferring it over glucose in some states
- Red blood cells - cannot use ketones (no mitochondria), so still need glucose (provided by gluconeogenesis from glycerol and amino acids)
In tissues, ketone bodies are converted back to acetyl-CoA and fed into the TCA cycle to generate ATP.
Why It Produces Weight Loss
Several mechanisms work together:
| Mechanism | How it helps |
|---|---|
| Reduced insulin | Less fat storage, more fat burning |
| Appetite suppression | Ketones (especially BHB) suppress ghrelin (the hunger hormone); high fat and protein are satiating |
| Water loss | Glycogen holds ~3g of water per gram; depleting glycogen releases several kilograms of water initially |
| Lower caloric efficiency | Protein has a high thermic effect; fat metabolism is slightly less efficient than glucose |
| Reduced lipogenesis | Low insulin = minimal conversion of carbs to stored fat |
Other Metabolic Effects
- Blood sugar control: Dramatically reduces glucose and glycated hemoglobin (HbA1c) in type 2 diabetes
- Insulin sensitivity: Improves, partly by reducing glucose transporter resistance pathways
- Inflammation: BHB inhibits the NLRP3 inflammasome and has antioxidant properties
- Gut microbiome: KD reduces Bifidobacteria and lowers pro-inflammatory Th17 cells
- Epilepsy: The original medical use - mechanism not fully clear, but involves reduced neuronal excitability from ketones, lower glucose, elevated GABA, and stabilization of mitochondrial function
- Cancer (experimental): Tumor cells depend heavily on glucose (Warburg effect); KD may starve them while ketones fuel normal cells
Nutritional Ketosis vs. Diabetic Ketoacidosis (DKA)
These are very different states:
| Nutritional Ketosis | DKA | |
|---|---|---|
| Insulin | Low but present | Near zero (Type 1 DM) |
| Blood ketones | 0.5-3 mmol/L | >10-25 mmol/L |
| Blood glucose | Normal or low | Very high |
| pH | Normal | Severely acidic |
| Dangerous? | No | Yes - medical emergency |
Physiological ketosis from a keto diet is tightly regulated by residual insulin and does not cause dangerous acidosis.
Caveats and Limitations
- "Keto flu" - first 1-2 weeks: fatigue, headache, brain fog, as the body adapts (due to electrolyte loss from water excretion and reduced insulin)
- Micronutrient gaps - low intake of fruits, legumes, and whole grains can reduce fiber, potassium, magnesium, and certain vitamins
- Elevated uric acid - can worsen gout
- LDL cholesterol may rise in some individuals (though HDL usually rises and triglycerides fall)
- Long-term sustainability is the main challenge for most people
Sources: Lippincott's Illustrated Reviews: Biochemistry, 8th ed.; Harper's Illustrated Biochemistry, 32nd ed.; Nature Signal Transduction & Targeted Therapy review on KD mechanisms (2021)
??
It looks like your message came through as just "??". Could you clarify what you'd like help with? For example:
- Did something in my previous answer confuse you?
- Do you have a new question?
- Were you testing if I'm still here?
Just let me know and I'll help!
How keto diet works
I just answered this in detail! Here's a quick summary of the full explanation I provided above:
How the Keto Diet Works - Summary
The core idea: Cut carbs drastically (<50g/day) → glucose runs out → body switches to burning fat → liver produces ketone bodies → ketones fuel the brain and body instead of glucose. This metabolic state is called ketosis.
The 4-Step Process:
- Glycogen depletion - Liver glycogen (~100g) runs out within ~24 hours of cutting carbs
- Fat mobilization - Low insulin triggers lipolysis; fatty acids flood the liver
- Ketogenesis - Liver converts excess acetyl-CoA (from fat burning) into 3 ketone bodies: acetoacetate, 3-hydroxybutyrate (BHB), and acetone
- Ketolysis - Brain, heart, and muscles burn ketones for energy (the liver makes them but can't use them itself)
Why it causes weight loss:
- Lower insulin = less fat storage
- Ketones suppress hunger hormones
- Initial rapid water loss (glycogen holds 3g water per gram)
- High satiety from fat and protein
Other effects:
- Improves blood sugar and insulin sensitivity (helpful in Type 2 diabetes)
- Anti-inflammatory (BHB inhibits the NLRP3 inflammasome)
- Original medical use: drug-resistant epilepsy
Key distinction - Ketosis ≠ Ketoacidosis:
Nutritional ketosis (0.5-3 mmol/L ketones, normal pH) is safe. Diabetic ketoacidosis (>10-25 mmol/L, acidic pH) is a medical emergency seen in uncontrolled Type 1 diabetes.
Scroll up to see the full detailed answer with the biochemistry diagram! Is there a specific part you'd like me to go deeper on?
What foods are allowed on keto?
Searching the Web
ketogenic diet allowed foods complete list 2024
Here's a practical breakdown of what you can and can't eat on keto:
Keto Diet: What to Eat
✅ EAT FREELY (Very Low or Zero Carbs)
Meat & Protein
- Beef - steak, ground beef, roast, brisket
- Pork - bacon, ham, pork chops, sausage (check labels)
- Poultry - chicken, turkey, duck (prefer fattier cuts like thighs over breast)
- Lamb, veal, venison
- Eggs - any style (one of the most keto-perfect foods)
Fish & Seafood
- Fatty fish - salmon, mackerel, sardines, tuna, trout (great omega-3 source)
- Shellfish - shrimp, crab, lobster, scallops (low carb but check portions)
- White fish - cod, bass, catfish, halibut
Fats & Oils
- Butter and ghee
- Olive oil, coconut oil, avocado oil
- Animal fats - lard, tallow
- Mayonnaise (full fat, no added sugar)
- Avocado (~2g net carbs each - also a great fat source)
Dairy (Full Fat)
- Heavy cream, sour cream
- Hard cheeses - cheddar, parmesan, gouda, brie (~0-1g carbs per oz)
- Soft cheeses - cream cheese, mozzarella
- Greek yogurt - limit (has some carbs)
- Milk - avoid (too many carbs)
Non-Starchy Vegetables (Low-Carb)
These are your main vegetable sources - leafy and above-ground veggies are usually safe:
- Spinach, kale, arugula, lettuce (~1g net carbs per cup)
- Broccoli, cauliflower, zucchini, cabbage
- Bell peppers, cucumber, celery
- Mushrooms, asparagus, green beans
- Avoid root vegetables (carrots, potatoes, beets) - too starchy
Nuts & Seeds (in moderation)
- Macadamia nuts (~2g net carbs per oz) - best for keto
- Almonds, walnuts, pecans, brazil nuts
- Chia seeds, flaxseeds, hemp seeds
- Avoid cashews and pistachios (higher carb)
⚠️ EAT IN LIMITED AMOUNTS
| Food | Why limit |
|---|---|
| Berries (strawberries, blueberries, raspberries) | ~5-10g carbs per half cup |
| Onions, tomatoes | ~4-5g net carbs each |
| Dark chocolate (>85% cocoa) | ~5g carbs per square |
| Cream cheese, ricotta | moderate carbs |
| Alcohol (dry wine, spirits) | can slow ketosis |
❌ AVOID (High Carb - Kicks You Out of Ketosis)
| Category | Examples |
|---|---|
| Grains | Bread, pasta, rice, oats, cereal, crackers |
| Sugar | Candy, soda, juice, honey, maple syrup, agave |
| Starchy vegetables | Potatoes, sweet potatoes, corn, peas |
| Legumes | Beans, lentils, chickpeas (high carb despite being "healthy") |
| Most fruits | Bananas, apples, oranges, grapes, mango |
| Low-fat "diet" products | Usually replace fat with sugar |
| Beer | Liquid bread - very high carb |
Drinks
- Fine: Water, sparkling water, black coffee, plain tea, bone broth
- In moderation: Coffee/tea with heavy cream, dry red or white wine
- Avoid: Juice, soda, energy drinks, sweetened coffee drinks, beer
A Simple Rule of Thumb
If it grows underground or is sweet - be cautious. If it's fatty, leafy, or from an animal - it's likely fine.
Aim for net carbs (total carbs minus fiber) under 20-50g per day to stay in ketosis. Most people find 20g is the "safe" target when starting out.
Create a 1-week keto meal plan example
Here's a practical 1-week keto meal plan. Each day stays under ~20-25g net carbs, with roughly 70% fat / 25% protein / 5% carbs.
🥑 1-Week Keto Meal Plan
Day 1 - Monday
| Meal | Food | Net Carbs |
|---|---|---|
| Breakfast | 3 scrambled eggs in butter + 3 strips bacon + black coffee | ~1g |
| Lunch | Tuna salad (mayo, celery, onion) in lettuce wraps | ~3g |
| Dinner | Grilled ribeye steak + sautéed spinach in garlic butter | ~2g |
| Snack | 1 oz macadamia nuts | ~2g |
| Daily total | ~8g |
Day 2 - Tuesday
| Meal | Food | Net Carbs |
|---|---|---|
| Breakfast | 2-egg omelette with cheese, mushrooms, and bacon | ~2g |
| Lunch | Chicken Caesar salad (no croutons, full-fat dressing) | ~4g |
| Dinner | Baked salmon + roasted broccoli with parmesan + butter | ~5g |
| Snack | Celery sticks + cream cheese | ~2g |
| Daily total | ~13g |
Day 3 - Wednesday
| Meal | Food | Net Carbs |
|---|---|---|
| Breakfast | Keto smoothie: heavy cream + spinach + almond butter + ice | ~3g |
| Lunch | Ground beef lettuce tacos with cheese, sour cream, avocado | ~5g |
| Dinner | Pork chops + cauliflower mash with butter and cream | ~6g |
| Snack | Hard-boiled egg + a few olives | ~1g |
| Daily total | ~15g |
Day 4 - Thursday
| Meal | Food | Net Carbs |
|---|---|---|
| Breakfast | Bacon and egg cups (eggs baked in bacon-lined muffin tin) | ~1g |
| Lunch | Avocado stuffed with shrimp salad (mayo, lime, cilantro) | ~4g |
| Dinner | Lamb chops + asparagus roasted in olive oil | ~4g |
| Snack | 1 oz cheddar + 5 pepperoni slices | ~1g |
| Daily total | ~10g |
Day 5 - Friday
| Meal | Food | Net Carbs |
|---|---|---|
| Breakfast | Full-fat Greek yogurt (plain) + a few raspberries + walnuts | ~8g |
| Lunch | BLT lettuce wrap (bacon, tomato slice, mayo, lettuce) | ~4g |
| Dinner | Pan-seared chicken thighs + zucchini noodles in pesto | ~6g |
| Snack | Handful of almonds | ~3g |
| Daily total | ~21g |
Day 6 - Saturday
| Meal | Food | Net Carbs |
|---|---|---|
| Breakfast | Smoked salmon + cream cheese + cucumber slices | ~3g |
| Lunch | Bunless cheeseburger with bacon, lettuce, tomato, mayo | ~4g |
| Dinner | Garlic butter shrimp + sautéed green beans + side salad | ~7g |
| Snack | 1-2 squares 85%+ dark chocolate | ~4g |
| Daily total | ~18g |
Day 7 - Sunday
| Meal | Food | Net Carbs |
|---|---|---|
| Breakfast | Keto pancakes (almond flour, eggs, cream cheese) + butter | ~4g |
| Lunch | Egg salad stuffed avocado halves | ~3g |
| Dinner | Slow-cooked beef brisket + roasted cabbage wedges | ~6g |
| Snack | Pork rinds + guacamole | ~3g |
| Daily total | ~16g |
Weekly Snapshot
| Day | Net Carbs | Highlights |
|---|---|---|
| Monday | ~8g | Classic keto start |
| Tuesday | ~13g | Fatty fish day |
| Wednesday | ~15g | Cauliflower as a carb substitute |
| Thursday | ~10g | Seafood focus |
| Friday | ~21g | Near the 20g threshold - fine |
| Saturday | ~18g | Treat day (dark chocolate) |
| Sunday | ~16g | Keto-friendly "comfort" foods |
Practical Tips
- Meal prep: Cook bacon and boil eggs in bulk on Sunday - saves time all week
- Electrolytes: Keto causes water and sodium loss early on - add salt to food, drink bone broth, and consider magnesium and potassium supplements to avoid "keto flu"
- Hunger: If genuinely hungry between meals, add more fat (butter, olive oil, avocado) rather than extra protein
- Eating out: Order bunless burgers, grilled meat with salad/veggies, or ask for sauces on the side (many contain hidden sugar)
- Track net carbs: Total carbs minus fiber = net carbs. Apps like Cronometer or Carb Manager make this easy
This plan is a starting template - portions and calories should be adjusted based on your body weight, activity level, and goals.
This is a shared conversation. Sign in to Orris to start your own chat.