
Screenshot_2026-06-09-12-23-59-84_a1b1bbe5f63d5b96c1a0f87c197ebfae.jpg
Please find answers for this
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I have enough information to provide comprehensive answers to all questions. Let me now compile everything.
Case 2: 62-year-old woman - Community-Acquired Pneumonia (CAP)
Question 1: Most Likely Diagnosis
Community-Acquired Pneumonia (CAP) - specifically bacterial CAP (likely due to Streptococcus pneumoniae).
Clinical reasoning:
- Fever (38.6°C), productive cough with yellow-green sputum, pleuritic right-sided chest pain
- RR 22/min, O2 saturation 92% on room air (hypoxemia)
- WBC 14,500/mm³ with neutrophil predominance (bacterial infection pattern)
- CRP elevated (acute-phase inflammatory marker)
- Chest X-ray: right lower lobe consolidation (hallmark of bacterial lobar pneumonia)
- Crackles on auscultation over the right lower lung field
The combination of fever, productive purulent sputum, neutrophilia, elevated CRP, and lobar consolidation on CXR is classic for bacterial CAP. S. pneumoniae accounts for 5-16% of identified pathogens and is the most common bacterial cause.
Question 2: Most Appropriate Initial Empiric Antibiotic Therapy
This patient requires hospitalization (see Q3). She is non-ICU, nonsevere CAP without risk factors for MRSA or Pseudomonas aeruginosa.
Recommended regimens (Goldman-Cecil Medicine):
| Setting | Regimen |
|---|---|
| Non-severe inpatient (no MRSA/Pseudomonas risk) | Option A: Respiratory fluoroquinolone monotherapy (e.g., levofloxacin 750 mg IV/PO daily) |
| Option B: Beta-lactam (e.g., ampicillin-sulbactam, ceftriaxone) + macrolide (azithromycin) or doxycycline | |
| Outpatient without comorbidities | Amoxicillin, doxycycline, or azithromycin monotherapy x5 days |
For this patient, the most appropriate choice is:
- Ceftriaxone 1-2g IV daily + Azithromycin 500mg IV/PO daily (beta-lactam + macrolide combination), OR
- Levofloxacin 750mg IV/PO daily (respiratory fluoroquinolone monotherapy)
Duration: minimum 5 days (extended if clinically unstable).
Note: Fluoroquinolones should be avoided if QT prolongation is present and carry risks (tendinopathy, C. difficile, peripheral neuropathy).
Question 3: Which CAP Patients Require Hospitalization?
Two validated scoring tools are used:
CURB-65 (Goldman-Cecil Medicine, Table 85-4)
One point for each:
| Factor | Points |
|---|---|
| Confusion | 1 |
| Urea (BUN) ≥ 20 mg/dL | 1 |
| Respiratory rate ≥ 30/min | 1 |
| Blood pressure: systolic <90 mmHg OR diastolic ≤60 mmHg | 1 |
| Age ≥ 65 years | 1 |
- Score 0-1: Outpatient treatment
- Score 2: Consider hospital admission
- Score >2: Hospital admission required; score ≥3 suggests ICU consideration
This patient's CURB-65: Age ≥65? No (62 years). RR 22 (not ≥30). No confusion. BP 130/78 (normal). BUN not stated. Score likely 0-1, but O2 sat of 92% and clinical picture suggest hospitalization is warranted.
PSI (Pneumonia Severity Index)
Divides patients into 5 classes based on demographics, comorbidities, exam findings, and labs. Classes I-II: outpatient; Class III: brief admission or observation; Classes IV-V: hospital/ICU admission.
Additional indications for hospitalization:
- O2 saturation <92% or PaO2 <60 mmHg
- Multi-lobe involvement
- Inability to maintain oral intake
- Significant comorbidities (diabetes, immunosuppression)
- Failure of outpatient therapy
- Social factors (inability to care for self at home)
Case 3: Wound
The image shows a laceration - a linear, clean-edged incised wound on the forearm/wrist.
Question 1: Type of Wound
This is an incised wound (laceration) - a clean-cut, linear wound through the skin and underlying tissue, caused by a sharp object (knife, glass, blade). The edges are well-defined with minimal surrounding tissue damage.
Classification of wounds includes:
- By cause: Incised, lacerated, contused, abrasion, puncture, burn
- By depth: Superficial (skin only), partial-thickness (dermis), full-thickness (through dermis)
- By contamination: Clean, clean-contaminated, contaminated, dirty/infected
- By duration: Acute vs. chronic
Question 2: Types of Wound Healing
(Bailey & Love's Surgery, 28th ed.; Sabiston Textbook of Surgery)
| Type | Description |
|---|---|
| Primary intention (1st intention) | Clean wound edges directly approximated (sutured, stapled, glued). Minimal scarring, best cosmetic result. Example: surgical incision, this laceration if sutured promptly. |
| Secondary intention (2nd intention) | Wound left open, heals by granulation tissue formation, wound contraction, and re-epithelialization from edges inward. Results in broader scar. Used for infected/heavily contaminated wounds. |
| Tertiary intention (delayed primary closure) | Wound initially left open (to allow drainage/debridement of contamination), then surgically approximated later when conditions are favorable. Also called "delayed primary closure." |
Question 3: Factors that Promote Wound Healing
Local factors:
- Adequate blood supply and tissue oxygenation
- Moist wound environment
- Absence of infection/foreign body
- Proper wound closure and minimal dead space
- Adequate debridement of necrotic tissue
Systemic factors:
- Good nutrition: Adequate protein (collagen synthesis), vitamin C (hydroxylation of proline/lysine in collagen), zinc (cofactor for enzymes), vitamin A
- Normal tissue perfusion and oxygenation (oxygen is required for collagen cross-linking and bacterial killing)
- Growth factors: PDGF, TGF-beta, EGF, bFGF, VEGF - all drive proliferation, angiogenesis, and matrix synthesis
- Controlled inflammation: Early, acute inflammatory phase is necessary for debridement and signaling
- Youthful age (growth factors more abundant, faster cellular response)
- Normal immune function
- Negative-pressure wound therapy (NPWT) and hyperbaric oxygen therapy (clinical adjuncts)
Question 4: Factors that Delay Wound Healing
(Bailey & Love's Surgery, 28th ed.; Sabiston Textbook of Surgery)
Systemic:
- Diabetes mellitus - impairs neutrophil function, reduces growth factors, causes microvascular disease and neuropathy
- Malnutrition - deficiency of protein, vitamin C, zinc
- Advancing age - reduced proliferative capacity
- Obesity - poor tissue perfusion, increased wound tension, adipose tissue has poor blood supply
- Smoking - vasoconstriction, reduced tissue oxygenation, impaired collagen synthesis
- Immunocompromised states (HIV, chemotherapy, steroids) - impaired inflammatory and proliferative response
- Medications: Corticosteroids (suppress inflammation and collagen synthesis), NSAIDs (block thromboxane/prostaglandin signaling), immunosuppressants, chemotherapy agents
- Connective tissue diseases
- Anemia and cardiovascular disease - reduced oxygen delivery
Local:
- Infection - prolongs inflammation, destroys new tissue, diverts nutrients
- Ischemia - insufficient oxygen
- Foreign body - perpetuates inflammation
- Excessive wound tension - prevents approximation
- Hematoma/seroma - creates dead space and medium for infection
- Radiation injury - damages microvasculature, fibrosis
Question 5: Phases of Wound Healing
(Sabiston Textbook of Surgery, Biological Basis of Modern Surgical Practice)
There are 4 phases, which may overlap simultaneously:
Phase 1 - Hemostasis (immediate, minutes to hours)
- Triggered by vascular injury
- Vasoconstriction followed by vasodilatation and increased permeability
- Platelet activation and aggregation via GPIIb-IIIa, binding to exposed collagen (requires von Willebrand factor)
- Platelet aggregation and fibrin clot formation seals the wound
- Platelets release growth factors: PDGF, TGF-beta, VEGF, EGF - these recruit inflammatory cells
- Goal: stop bleeding, seal wound surface, remove debris and bacteria
Phase 2 - Inflammatory Phase (hours to days 1-5)
- Increased vascular permeability, cellular migration by chemotaxis
- Neutrophils first responders (first 24-48h): phagocytose bacteria, release proteases and reactive oxygen species; primary role is antimicrobial defense
- Macrophages arrive by day 2-3 and are the master regulators: phagocytose debris, release IL-1, IL-6, TNF-alpha, TGF-beta, PDGF, MMPs
- IL-1 enhances collagenase production, stimulates fibroblast and keratinocyte growth
- TNF-alpha initiates the injury response, upregulates adhesion molecules
- Clinically: rubor, calor, dolor, tumor (redness, warmth, pain, swelling)
Phase 3 - Proliferative Phase (days 3-21)
- Angiogenesis: New capillaries form under VEGF stimulation (granulation tissue is highly vascular)
- Fibroplasia: Fibroblasts migrate in and synthesize collagen (initially type III, later replaced by type I) and extracellular matrix
- Wound contraction: Myofibroblasts pull wound edges together centripetally
- Re-epithelialization: Keratinocytes migrate from wound edges and adnexal structures to resurface the wound; driven by EGF, KGF, IFN-kappa
- Granulation tissue (pink, moist, vascular) fills the wound
- ECM components: collagen, fibronectin, glycosaminoglycans (GAGs)
Phase 4 - Maturation/Remodeling Phase (weeks to 1-2 years)
- Begins around week 3 and continues for up to 2 years
- Type III collagen progressively replaced by type I collagen (stronger)
- Collagen fibers are reorganized, cross-linked, and aligned along stress lines
- Wound vascularity decreases (granulation tissue "matures" into scar)
- Maximum tensile strength is ~80% of original skin, reached around 6-12 months
- MMPs degrade ECM and regulate matrix turnover
- Hypertrophic scars or keloids result if remodeling is dysregulated
Key concept: All four phases may occur simultaneously in a large wound. Failure to progress through phases (as in diabetes) leads to chronic non-healing wounds.
Sources: Goldman-Cecil Medicine (International Ed.), Sabiston Textbook of Surgery (Biological Basis of Modern Surgical Practice), Bailey & Love's Short Practice of Surgery (28th ed.)
You didn't answer me what type of wound is it?
Loading Image
Based on the image provided visually at the start of the conversation, I can describe what I see:
The wound shows two parallel, linear, clean-edged cuts on what appears to be the forearm. The edges are sharp, well-defined, and the cuts run in the same direction.
Type of Wound: Incised Wound
This is specifically an incised wound (also called a cut wound or sharp force injury), characterized by:
- Caused by: A sharp-edged object (knife, razor blade, glass shard)
- Edges: Clean, well-defined, regular margins with minimal surrounding tissue damage
- Length > Depth: The wound is longer than it is deep
- Bleeding: Often profuse (sharp cut severs blood vessels cleanly)
- Surrounding tissue: No bruising, crushing, or tearing
- Healing potential: Excellent if sutured promptly - heals by primary intention
How it differs from other wound types:
| Wound Type | Characteristics |
|---|---|
| Incised wound (this case) | Sharp object, clean edges, length > depth |
| Laceration | Blunt force tearing, irregular ragged edges |
| Abrasion | Superficial scraping, no depth |
| Puncture/Stab | Depth > length, narrow entry |
| Contusion/Bruise | Blunt trauma, intact skin |
| Avulsion | Tissue torn away |
| Burn | Heat/chemical/electrical |
Management:
Since the edges are clean and well-apposed, this wound should be closed by primary intention - irrigation, debridement if needed, then suturing/closure for optimal healing and minimal scarring.

Screenshot_2026-06-09-12-34-26-82_a1b1bbe5f63d5b96c1a0f87c197ebfae.jpg
Answer all the questions
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
I now have all the information needed. Let me compile comprehensive answers for both cases.
Case 2: 50-year-old woman with progressive dyspnea + systemic sclerosis
Question 1: Most Likely Diagnosis
Pulmonary Arterial Hypertension (PAH) - Group 1, associated with systemic sclerosis (connective tissue disease)
Clinical reasoning:
- Progressive exertional dyspnea over 6 months
- Loud P2 (accentuated pulmonic component of S2) = elevated pulmonary artery pressure
- Jugular venous distension + peripheral edema = right heart failure (cor pulmonale)
- Echocardiography: Right ventricular enlargement + estimated pulmonary artery systolic pressure (PASP) 60 mmHg (normal <35 mmHg)
- Background of systemic sclerosis - one of the most common conditions associated with PAH (connective tissue disease is a well-recognized risk factor for Group 1 PAH)
- No chest pain or cough to suggest another etiology
Question 2: Initial Test to Confirm Pulmonary Hypertension
Right Heart Catheterization (RHC) is the gold standard.
"Right heart catheterization is virtually always required to confirm the diagnosis of pulmonary hypertension, assess its severity, and evaluate ventricular function." - Goldman-Cecil Medicine
"Right heart catheterization is required to confirm the diagnosis of pulmonary hypertension, test for important cardiac causes, and in appropriate patients perform acute vasodilator trials to determine an initial approach to therapy." - Fishman's Pulmonary Diseases
Diagnostic criteria on RHC:
- Mean pulmonary artery pressure (mPAP) ≥ 25 mmHg at rest (updated 2022 threshold: ≥20 mmHg)
- Pulmonary capillary wedge pressure (PCWP) ≤ 15 mmHg (to exclude left heart cause)
- Elevated pulmonary vascular resistance (PVR) > 3 Wood units
Screening tool: Doppler echocardiography (as in this patient - PASP >40 mmHg on echo prompts RHC for confirmation). Echo is the first-line screening test; RHC is the confirmatory test.
Additional workup:
- PFTs (spirometry, DLCO - usually reduced in PAH-SSc)
- 6-minute walk test
- NT-proBNP (elevated = marker of RV strain)
- V/Q scan (to rule out chronic thromboembolic disease - Group 4 PH)
- High-resolution CT chest
- ANA, anti-Scl-70, anticentromere antibodies (already known to have SSc)
Question 3: Mainstay of Treatment for Group 1 PAH
Treatment targets three main pathways that are dysregulated in PAH: NO pathway, endothelin axis, and prostacyclin pathway.
Supportive Care (all PAH patients):
- Loop diuretics - reduce pulmonary vascular congestion and RV volume overload
- Supplemental oxygen - attenuates hypoxic pulmonary vasoconstriction
- Digoxin - may improve RV output by ~10% in RV failure
- Supervised exercise/pulmonary rehabilitation - proven benefit
- Vaccinations (influenza, pneumococcal)
- Avoid pregnancy (high maternal mortality)
PAH-Specific Pharmacotherapy (14 FDA-approved agents across 3 pathways):
| Pathway | Drug Class | Examples |
|---|---|---|
| NO pathway | PDE-5 inhibitors | Sildenafil, Tadalafil |
| Soluble guanylate cyclase stimulators | Riociguat | |
| Endothelin pathway | Endothelin receptor antagonists (ERAs) | Ambrisentan (ERA-A), Bosentan, Macitentan |
| Prostacyclin pathway | Prostacyclin analogues | Epoprostenol (IV), Treprostinil (SC/IV/inhaled/oral), Iloprost (inhaled) |
| Prostacyclin receptor agonists | Selexipag (oral) |
Current Evidence-Based Strategy:
Upfront combination oral therapy is now favored for newly diagnosed treatment-naive PAH (without indication for immediate parenteral therapy):
-
AMBITION Trial: Combination of Ambrisentan + Tadalafil showed a 50% reduction in hazard for the composite endpoint (death, hospitalization, disease progression) vs. monotherapy (Braunwald's Heart Disease)
-
For NYHA Class IV / cardiogenic shock / syncope / RV ischemia - immediate continuous IV prostacyclin therapy (epoprostenol) is indicated
-
For patients with positive acute vasoreactivity test (~5% of iPAH): high-dose calcium channel blockers (nifedipine, diltiazem, amlodipine)
For This Patient (SSc-associated PAH):
- PDE-5 inhibitor (sildenafil or tadalafil) + ERA (ambrisentan or macitentan) is the standard initial combination
- Note: SSc-PAH patients rarely show vasoreactivity, so CCBs are generally not used
- Lung transplantation should be considered if the disease progresses despite maximal medical therapy
Case 3: 50-year-old male - Road Traffic Accident
The image shows bilateral periorbital ecchymosis (bruising around both eyes) with subconjunctival hemorrhage.
Question 1: Name of This Sign
"Raccoon Eyes" (Periorbital Ecchymosis)
Also called "Panda eyes" or the "Raccoon sign"
This is bilateral periorbital bruising/ecchymosis without a direct blow to the eye socket itself, caused by blood tracking forward along tissue planes from a fracture at the anterior skull base.
Question 2: Diagnosis
Basilar Skull Fracture - specifically an anterior cranial fossa fracture
"Hemotympanum, mastoid ecchymosis (Battle sign), periorbital ecchymosis ('raccoon eyes'), and CSF otorrhea/rhinorrhea are indicative of a basilar skull fracture." - Washington Manual of Medical Therapeutics
"A fracture of the anterior skull base can result in anosmia, CSF drainage from the nose (rhinorrhea), or periorbital ecchymosis, known as raccoon eyes." - Schwartz's Principles of Surgery
Other signs of basilar skull fracture to look for:
- Battle's sign - bruising over mastoid process (middle fossa fracture)
- Hemotympanum - blood behind tympanic membrane
- CSF rhinorrhea (anterior fossa) or CSF otorrhea (middle fossa)
- Anosmia (olfactory nerve damage)
- CN VII or VIII palsy (petrous temporal bone fracture)
Question 3: Common Types of Skull Fractures
(Grainger & Allison's Diagnostic Radiology; Harrison's Principles; Schwartz's Surgery)
| Type | Description |
|---|---|
| Linear fracture | Most common. Single crack in skull without bone displacement. Extends from point of impact toward skull base. Usually benign but increases risk of epidural hematoma if it crosses meningeal artery grooves. |
| Depressed fracture | Fragment pushed inward below the level of surrounding skull. Associated with higher rates of underlying brain parenchymal injury. Requires surgical elevation if depressed >thickness of skull. |
| Comminuted fracture | Multiple fragments - skull shattered into >2 pieces. Often from high-energy direct blow. May be depressed or non-depressed. |
| Diastatic fracture | Fracture along a suture line, causing widening of sutures. More common in children. |
| Basilar skull fracture | Fracture of the skull base (anterior, middle, or posterior fossa). Diagnosed clinically (raccoon eyes, Battle's sign, CSF leak) - often invisible on plain X-ray; CT is needed. |
| Open/compound fracture | Skull fracture communicating with external environment (laceration over fracture). High risk of infection and meningitis. |
| Ping-pong (growing) fracture | Pediatric only - inward buckling without complete break, like denting a ping-pong ball. |
Question 4: Investigations to Confirm the Presence of CSF
CSF can leak from the nose (rhinorrhea) or ear (otorrhea) after a basilar skull fracture. Distinguishing CSF from blood/mucus is important.
Bedside Test:
Halo Sign (Ring/Target Sign):
- A drop of the bloody/clear fluid is placed on filter paper or a bed sheet
- CSF has lower viscosity than blood and migrates faster outward, forming a clear outer ring ("halo") surrounding a central bloody/red spot
- Positive halo = CSF present
- (Rosen's Emergency Medicine)
Laboratory Tests:
| Test | Details |
|---|---|
| Beta-2 transferrin (β2-transferrin) | Gold standard for confirming CSF. Beta-2 transferrin is a protein found almost exclusively in CSF (not in blood, nasal secretions, or tears). Highly sensitive and specific. Requires electrophoresis. |
| Beta-trace protein (prostaglandin D synthase) | Another CSF-specific protein. High sensitivity/specificity. Faster than beta-2 transferrin. |
| Glucose concentration | CSF glucose is similar to blood glucose (~60-70% of serum). Nasal secretions normally have very low glucose. A glucose level >30 mg/dL in nasal/ear fluid suggests CSF. However, low specificity (blood contamination can give false positive). |
| CT head | Identifies skull fractures, pneumocephalus, intracranial hemorrhage. CT cisternography (with intrathecal contrast) can localize the CSF leak site. |
| MRI with CISS/FIESTA sequences | Best for identifying CSF leak location (e.g., cribriform plate defect). |
| Fluorescein | Intrathecal fluorescein injection can detect occult CSF leaks intraoperatively. |
Most practical workflow: Halo sign at bedside → beta-2 transferrin to confirm → CT head to identify fracture and complications.
Sources: Goldman-Cecil Medicine (International Ed.), Braunwald's Heart Disease, Rosen's Emergency Medicine, Harrison's Principles of Internal Medicine 22e, Schwartz's Principles of Surgery (11th ed.), Grainger & Allison's Diagnostic Radiology, Washington Manual of Medical Therapeutics
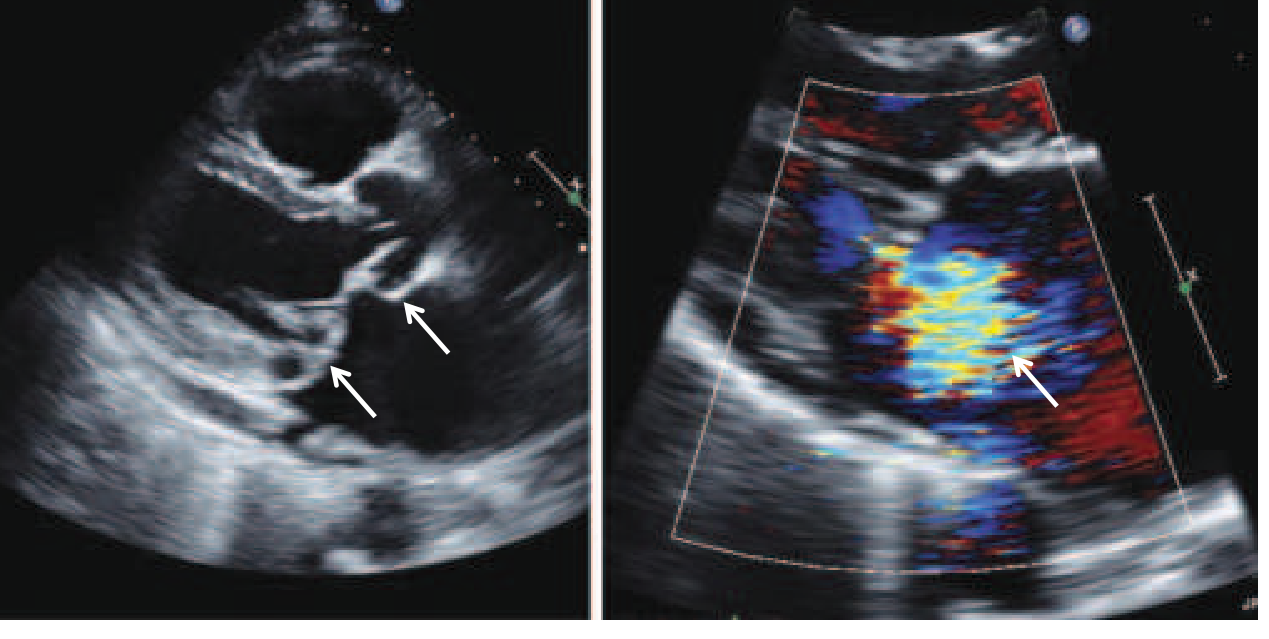
Mitral valve prolapse
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, structured overview of Mitral Valve Prolapse (MVP):
Mitral Valve Prolapse (MVP)
Definition
MVP occurs when one or both mitral valve leaflets prolapse (bulge) during systole beyond the mitral valve annular plane back into the left atrium. It is the most common valvular disorder in developed countries, affecting approximately 2-3% of the general population.
(Goldman-Cecil Medicine; Harrison's Principles, 22nd ed.)
Etiology & Pathophysiology
Primary MVP (Myxomatous Degeneration)
- The most common form. Leaflets undergo myxomatous degeneration - accumulation of mucopolysaccharides in the spongiosa layer of the valve, leading to leaflet thickening, redundancy, and elongation of chordae tendineae
- Chordae become elongated, slack, or rupture - allowing leaflets to billow back into the LA
- Posterior leaflet is more commonly affected than the anterior
- The mitral annulus is often dilated
Genetics & Associated Conditions
- Can be familial - autosomal dominant with variable penetrance (BMPR2, LMCD1, SPTBN1, TGFB2 gene loci identified)
- Associated with heritable connective tissue disorders:
- Marfan syndrome (most strongly associated)
- Ehlers-Danlos syndrome
- Osteogenesis imperfecta
- Other associations: skeletal deformities (high-arched palate, pectus excavatum, straight back syndrome), Ostium secundum ASD (~20% of cases), inguinal hernias
Secondary MVP
- Seen in: coronary artery disease, rheumatic heart disease, cardiomyopathies, acute rheumatic fever
Pathophysiologic consequences:
- Prolapsing leaflets cause excessive papillary muscle stress → localized ischemia → fibrosis (visible as late gadolinium enhancement on CMR) → nidus for ventricular arrhythmias
- Progressive annular dilation and calcification cause worsening mitral regurgitation (MR)
- Chordae rupture → flail leaflet → sudden severe MR
Epidemiology
- More common in women than men
- Most frequent between ages 15-30 years
- Older men (>50 years) tend to have more severe disease with chordal rupture
- MVP is now the most common cause of isolated severe MR requiring surgery in North America
Clinical Features
Symptoms
Most patients are asymptomatic and remain so throughout life. When present:
- Palpitations (most common - due to ventricular premature contractions, SVT, AF)
- Chest pain - often substernal, prolonged, not exertion-related; rarely resembles angina. May be due to papillary muscle ischemia
- Dizziness, presyncope, syncope - linked to autonomic dysfunction
- Dyspnea and fatigue - if significant MR develops
- Panic attacks - commonly described
- Rarely: transient cerebral ischemic attacks (emboli from mitral valve endothelial disruption)
Physical Examination - Classic Signs:
| Sign | Mechanism |
|---|---|
| Mid-systolic click | Sudden tensing of elongated chordae when prolapse reaches maximal excursion (0.14s or more after S1) |
| Late systolic crescendo-decrescendo murmur | MR begins as leaflets move past coaptation point; heard best at apex; occasionally "whooping" or "honking" |
Dynamic Auscultation - Diagnostic Maneuvers:
| Maneuver | Effect on LV volume | Click/Murmur effect |
|---|---|---|
| Standing / Valsalva (strain phase) | Decreases LV volume | Click moves earlier, murmur becomes louder and more holosystolic |
| Squatting / Isometric exercise | Increases LV volume | Click moves later, murmur may disappear |
| Supine position | Increases LV volume | Click and murmur move later |
Key concept: A smaller LV = more relative redundancy of leaflets and chordae = more prolapse = earlier click.
Investigations
ECG
- Usually normal
- May show: biphasic or inverted T waves in leads II, III, aVF
- Supraventricular or ventricular premature beats
Echocardiography (Diagnostic Gold Standard)
Transthoracic Echo (TTE):
- Diagnostic criterion: Systolic displacement of mitral valve leaflet belly by ≥2 mm into the LA above the mitral annular plane on parasternal long-axis view
- Leaflet thickening ≥5 mm (myxomatous change) = higher risk of complications
- Color Doppler: assess severity of MR (often eccentric jet)
- Identifies flail leaflet, chordal rupture, annular dilation
Transesophageal Echo (TEE):
- Used when more precise anatomic detail is needed
- Mandatory for intraoperative guidance during surgical/transcatheter repair
Cardiac MRI
- Detects papillary muscle fibrosis (late gadolinium enhancement)
- Precise LV volume assessment
- Identifies mitral annular disjunction
Complications
| Complication | Notes |
|---|---|
| Mitral regurgitation | Most common significant complication; progressive; may become severe |
| Infective endocarditis | Risk in patients with MR and/or leaflet thickening |
| Arrhythmias | VPCs, PSVT, ventricular tachycardia, AF |
| Sudden cardiac death | Rare; most often in patients with severe MR + LV dysfunction; also associated with flail leaflet, mitral annular disjunction, papillary muscle fibrosis |
| Stroke / TIA | Emboli from mitral valve (endothelial disruption); less clearly supported by recent data |
| Chordae rupture | Leads to flail leaflet and acute severe MR |
~10% of patients with thickened leaflets experience serious complications (endocarditis, stroke, severe MR, or sudden death). Men are ~2x more likely to progress to severe MR than women.
Treatment
Asymptomatic MVP (most patients):
- No treatment required
- Infective endocarditis prophylaxis NOT routinely recommended (unless prior history of endocarditis)
- Regular follow-up with echocardiography to monitor MR progression
Symptomatic MVP:
- Beta-blockers - for chest pain, palpitations, and autonomic dysfunction
- Anticoagulation (warfarin/DOAC) - if AF present (guided by CHA2DS2-VASc score); not routinely for MVP alone
Surgical / Interventional Indications (for severe primary MR due to MVP):
| Indication | Details |
|---|---|
| Symptomatic severe MR (NYHA III/IV) | Surgery clearly indicated |
| Asymptomatic severe MR + LV dysfunction (EF <60% or LVESD >40mm) | Surgery indicated |
| AF or pulmonary hypertension with severe MR | Surgery indicated |
| Low-risk asymptomatic patient with ≥95% chance of durable repair | Surgery may be considered |
Mitral valve repair is preferred over replacement - lower mortality, better LV function preservation, no need for lifelong anticoagulation.
- Posterior leaflet prolapse: straightforward repair (resection/plication)
- Anterior/bileaflet prolapse (Barlow's): requires advanced surgical skills
Transcatheter edge-to-edge repair (TEER - MitraClip/PASCAL): For patients with severe MR at prohibitive/high surgical risk.
Lung transplantation: Not applicable for MVP; bilateral lung transplant is considered only for end-stage PAH - not for MVP.
Prognosis
- The vast majority of patients have a benign, lifelong course
- By age 50: ~1 in 200 men require surgery for MR
- By age 70: risk rises to ~3%
- Patients with thickened, redundant leaflets on echo carry higher risk and warrant closer surveillance
Sources: Harrison's Principles of Internal Medicine (22nd ed.), Goldman-Cecil Medicine (International Ed.), Textbook of Family Medicine (9th ed.)

IMG_20260610_111459.jpg
Answer this questions concisely
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Case 2 (Page 1): 25-year-old female, 3 days post-delivery - Painful red fluctuant right breast mass, USG shows collection
Q1. Diagnosis
Puerperal (Lactational) Breast Abscess
Painful, red, fluctuant breast mass + USG showing a collection (hypoechoic fluid with absent vascular signals) 3 days post-delivery = breast abscess complicating mastitis.
Q2. Anatomy & Function of the Breast
Anatomy:
- The breast lies between the 2nd-6th ribs, overlying the pectoralis major and serratus anterior
- Composed of 15-20 lobes of glandular tissue arranged radially, each draining into a lactiferous duct that opens at the nipple
- Lobes are separated by Cooper's suspensory ligaments (connect skin to deep fascia)
- Tail of Spence = axillary extension of breast tissue
- Blood supply: internal mammary artery, lateral thoracic artery, intercostal perforators
- Lymphatic drainage: primarily to axillary nodes (75%); also to internal mammary and supraclavicular nodes
- Innervation: intercostal nerves T4-T6
Function:
- Lactation (milk production and secretion)
- Secondary sexual characteristic
- Nipple-areola complex contains smooth muscle for milk ejection via oxytocin
Q3. Most Common Microorganism
Staphylococcus aureus (40% of puerperal mastitis/abscess cases)
- Other organisms: E. coli, Streptococcus species
- Consider CA-MRSA (community-acquired MRSA) in resistant cases
(Tintinalli's Emergency Medicine)
Q4. Triple Assessment of the Breast
Triple assessment is the standard evaluation for any breast lump, combining three components:
| Component | Details |
|---|---|
| 1. Clinical examination | History + inspection + palpation by a clinician |
| 2. Imaging | Ultrasound (preferred <35 years / abscess); Mammography (≥35 years); MRI if needed |
| 3. Pathological (tissue) | Fine needle aspiration cytology (FNAC), core needle biopsy, or open biopsy |
All three findings should be concordant. Discordance between any two components requires further investigation or surgical excision.
Q5. Management
- Analgesia (regular, adequate)
- Antibiotics - antistaphylococcal:
- Oral: cephalosporins (e.g., cefalexin) or flucloxacillin
- If MRSA suspected: clindamycin or IV vancomycin
- Continue breastfeeding - do NOT stop; emptying the breast is therapeutic
- Drainage - first-line for confirmed abscess:
- USG-guided needle aspiration (preferred, avoids milk fistula)
- Surgical incision & drainage - reserved as last resort in lactating women (risk of milk fistula)
- Wound care post-drainage
Case 3 (Page 1): 46-year-old male, hematemesis, alcohol + heroin abuse, splenomegaly, caput medusae, spider angiomata, ascites, abnormal LFTs
Q1. Most Likely Diagnosis
Decompensated Liver Cirrhosis with Esophageal Variceal Hemorrhage
Evidence: hematemesis + alcohol history + splenomegaly + caput medusae (portal hypertension sign) + spider angiomata + ascites (fluid wave) + elevated bilirubin (3.0 mg/dL) + elevated liver enzymes + prolonged PT (25 sec) + low albumin (2.0 g/dL).
Caput medusae specifically indicates portal hypertension with reversal of flow in periumbilical veins. The source of bleeding is most likely esophageal varices.
Q2. Tests / Imaging to Confirm Diagnosis
| Investigation | Purpose |
|---|---|
| Upper GI Endoscopy (EGD) | Gold standard - visualizes and grades varices; confirms variceal bleed; allows band ligation |
| Abdominal Ultrasound + Doppler | Shows cirrhotic liver texture, portal vein diameter, splenomegaly, ascites, flow direction |
| CT Abdomen | Assesses liver parenchyma, varices, splenomegaly, ascites |
| Liver Biopsy | Confirms cirrhosis histologically (if diagnosis uncertain) |
| Child-Pugh / MELD score | Assesses severity and prognosis |
| FBC, Coagulation (INR/PT) | Already done: PT prolonged, indicates synthetic dysfunction |
| AFP | Screens for hepatocellular carcinoma complicating cirrhosis |
| Hepatitis B/C serology | Identifies underlying etiology |
Q3. Most Appropriate Treatment
Acute variceal hemorrhage management (ABCDE approach):
- Resuscitation - IV access, fluid resuscitation, blood transfusion (target Hb ~7-8 g/dL - avoid over-transfusion)
- Vasoactive drugs (start immediately, before endoscopy):
- Terlipressin (preferred) or octreotide/somatostatin - reduce portal pressure
- Prophylactic antibiotics - IV ceftriaxone (reduces bacterial infection risk, improves survival)
- Urgent endoscopy (EGD) within 12 hours - Endoscopic variceal band ligation (EVL) is treatment of choice
- Correction of coagulopathy - Vitamin K, FFP, platelets as needed
- Avoid hepatotoxic drugs and lactulose for encephalopathy prevention
- If bleeding uncontrolled: TIPS (Transjugular Intrahepatic Portosystemic Shunt)
- Secondary prophylaxis after acute episode: Non-selective beta-blockers (propranolol/carvedilol) + repeat EVL until variceal eradication
Case 2 (Page 2): 20-year-old male, right iliac fossa pain, positive Rovsing & Psoas signs, leukocytosis 14.5 × 10⁹/L
Q1. Diagnosis
Acute Appendicitis
Classic triad: periumbilical pain migrating to RIF + fever + leukocytosis + positive Rovsing and Psoas signs.
Q2. Anatomy & Function of the Appendix
- A blind-ended tubular structure arising from the posteromedial wall of the cecum, 2-3 cm below the ileocecal valve
- Length: average 9 cm (range 2-20 cm)
- Lies at McBurney's point (junction of medial 2/3 and lateral 1/3 of line between umbilicus and right ASIS) - classic site of maximum tenderness
- Variable positions: retrocecal (most common, 65%), pelvic, pre-ileal, post-ileal, subcecal
- Blood supply: appendicular artery (branch of ileocolic artery from SMA) - an end artery
- Contains abundant lymphoid tissue (part of GALT - gut-associated lymphoid tissue); acts as an immune organ
Q3. Alvarado Score
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease)
| Feature | Points |
|---|---|
| Migration of pain to RIF | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| Tenderness in RLQ | 2 |
| Rebound tenderness | 1 |
| Elevated temperature | 1 |
| Leukocytosis | 2 |
| Left shift (neutrophilia) | 1 |
| Total | 10 |
Interpretation:
- 1-4: Appendicitis unlikely
- 5-6: Possible appendicitis - imaging needed
- 7-8: Probable appendicitis - surgical consultation
- 9-10: Very likely appendicitis - operate
This patient: Migration(1) + Nausea(1) + RLQ tenderness(2) + Temp(1) + Leukocytosis(2) = at least 7 → probable appendicitis.
Q4. Rovsing & Psoas Signs
Rovsing's Sign:
- Pressure applied to the left lower quadrant causes pain felt in the right lower quadrant
- Positive due to: gas/peritoneal fluid shifting and causing peritoneal irritation at the site of the inflamed appendix
- Indicates peritoneal irritation from appendicitis
Psoas Sign (Iliopsoas sign):
- With patient lying on left side, extension of the right hip (or with patient supine, passive extension of right leg) causes pain in RIF
- Positive when: the inflamed appendix lies retrocecally and is irritating the underlying psoas/iliacus muscle
- Also elicited by: asking patient to flex right hip against resistance
Q5. Types of Incisions for Appendectomy
| Incision | Details |
|---|---|
| Gridiron (McBurney's) incision | Oblique incision through McBurney's point, perpendicular to a line from umbilicus to ASIS. Most classic open approach. |
| Lanz incision | Transverse incision at McBurney's point. Better cosmesis, preferred in females. |
| Rutherford-Morrison incision | Extended gridiron toward iliac crest - for large/complicated appendices |
| Midline laparotomy | Used when diagnosis uncertain, generalized peritonitis, or perforation with abscess |
| Pfannenstiel incision | Low transverse - used especially in women when gynecological cause cannot be excluded |
| Laparoscopic (3-port) | Now the gold standard: umbilical port (camera) + two working ports. Better cosmesis, fewer wound complications, faster recovery |
Case 3 (Page 2): 65-year-old woman, right knee pain, osteophytes, joint space narrowing, subchondral cysts on X-ray, ESR 8 mm/hr, leukocytes 6000
Q1. Most Likely Diagnosis
Osteoarthritis (OA) of the Right Knee
Evidence: elderly female, 5-year progressive mechanical joint pain, decreased ROM, joint effusion (not warm/red = non-inflammatory), osteophytes + subchondral bone cysts + joint space narrowing on X-ray, normal ESR (8 mm/hr) and WBC (rules out inflammatory/infective arthritis).
Q2. Typical Radiographic Findings
The classic 4 X-ray features of OA (mnemonic: LOSS):
| Finding | Explanation |
|---|---|
| L - Loss of joint space | Asymmetric joint space narrowing (medial compartment of knee most often affected) due to cartilage loss |
| O - Osteophytes | Bony spurs at joint margins; pathologic activation of periarticular endochondral ossification |
| S - Subchondral sclerosis (Eburnation) | Increased bone density beneath the cartilage as bone thickens in response to stress |
| S - Subchondral cysts ("Geodes") | Cystic lucencies in bone below the cartilage, formed by synovial fluid forced into bone through cartilage defects |
Additional: varus or valgus deformity, loose bodies.
Q3. Most Appropriate Treatment
Conservative (first-line):
- Weight loss - single most effective intervention; reduces load on joint
- Physiotherapy - quadriceps strengthening, ROM exercises
- Walking aids (cane/walker if needed)
- NSAIDs (topical first - diclofenac gel; oral if needed - with PPI cover)
- Paracetamol (acetaminophen) - for mild-moderate pain
- Intra-articular corticosteroid injection - for acute flares with effusion
- Intra-articular hyaluronic acid - viscosupplementation
- Activity modification (avoid high-impact activities)
Surgical (when conservative fails, severe disease):
- Total Knee Arthroplasty (TKA) - gold standard surgical treatment; indicated when pain significantly impairs quality of life and conservative measures fail
- High tibial osteotomy - for younger patients with unicompartmental OA and varus deformity
- Unicompartmental (partial) knee replacement - if only one compartment affected
- Arthroscopic washout - limited evidence, rarely indicated now
(Miller's Review of Orthopaedics, 9th ed.; Tintinalli's; Goldman-Cecil Medicine)
Can you make it more short answers
Here are all the answers in concise form:
Case 2 (Breast) — Post-delivery breast abscess
Q1. Diagnosis: Puerperal (Lactational) Breast Abscess
Q2. Anatomy & Function of Breast:
- 15-20 glandular lobes draining via lactiferous ducts to the nipple
- Supported by Cooper's ligaments; axillary tail of Spence
- Blood supply: internal mammary + lateral thoracic arteries
- Lymph drains mainly to axillary nodes
- Function: milk production (lactation), secondary sexual characteristic
Q3. Most Common Organism: Staphylococcus aureus (40% of cases); also E. coli, Streptococcus
Q4. Triple Assessment:
- Clinical examination
- Imaging (USG <35 yrs; Mammogram ≥35 yrs)
- Pathology (FNAC or core needle biopsy)
Q5. Management:
- Analgesics + antistaphylococcal antibiotics (cefalexin/flucloxacillin; vancomycin if MRSA)
- USG-guided needle aspiration (first-line)
- Surgical I&D only if aspiration fails
- Continue breastfeeding throughout
Case 3 (Liver) — Hematemesis + cirrhosis signs
Q1. Diagnosis: Decompensated Liver Cirrhosis with Esophageal Variceal Hemorrhage
Q2. Tests:
- Upper GI Endoscopy (gold standard - confirms varices, allows treatment)
- Abdominal Ultrasound + Doppler (portal hypertension)
- LFTs, PT/INR, FBC, albumin (already done)
- Child-Pugh/MELD score (severity)
Q3. Treatment:
- Resuscitate (IV fluids, blood transfusion target Hb ~7-8 g/dL)
- Terlipressin IV (vasoactive drug, start immediately)
- IV Ceftriaxone (prophylactic antibiotics)
- Urgent EGD + Endoscopic Variceal Band Ligation (EVL) within 12 hours
- If uncontrolled: TIPS
- Secondary prophylaxis: non-selective beta-blockers + repeat EVL
Case 2b (Appendix) — RIF pain, Rovsing+, Psoas+, WBC 14.5
Q1. Diagnosis: Acute Appendicitis
Q2. Anatomy & Function:
- Blind-ended tube from posteromedial cecum, ~9 cm long
- Located at McBurney's point (lateral 1/3 of line from umbilicus to ASIS)
- Most common position: retrocecal (65%)
- Blood supply: appendicular artery (end artery from ileocolic)
- Function: contains lymphoid tissue (immune/GALT role)
Q3. Alvarado Score (max 10):
| Feature | Points |
|---|---|
| Pain migration to RIF | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| RLQ tenderness | 2 |
| Rebound tenderness | 1 |
| Fever | 1 |
| Leukocytosis | 2 |
| Left shift | 1 |
- ≤4: unlikely; 5-6: possible; 7-8: probable; 9-10: definite
Q4. Rovsing & Psoas Signs:
- Rovsing's sign: Pressure on LIF → pain felt in RIF (peritoneal irritation at appendix site)
- Psoas sign: Extension of right hip causes RIF pain → indicates retrocecal appendix irritating iliopsoas muscle
Q5. Incisions for Appendectomy:
- Gridiron (McBurney's): oblique through McBurney's point — classic
- Lanz: transverse at McBurney's — better cosmesis
- Midline laparotomy: generalized peritonitis/perforation
- Laparoscopic (3-port): now the gold standard
Case 3b (Knee) — Elderly woman, joint space narrowing, osteophytes, subchondral cysts
Q1. Diagnosis: Osteoarthritis (OA) of the Right Knee
Q2. X-ray Findings (mnemonic LOSS):
- L - Loss of joint space (asymmetric narrowing)
- O - Osteophytes (bony spurs at joint margins)
- S - Subchondral Sclerosis/Eburnation
- S - Subchondral cysts (geodes)
Q3. Treatment:
- Conservative: Weight loss, physiotherapy, NSAIDs (topical → oral), paracetamol, intra-articular steroid injection
- Surgical (when conservative fails): Total Knee Arthroplasty (TKA) — gold standard

IMG_20260610_111229.jpg
Give me short answers
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here are short, concise answers for all three cases:
Case 2: 50-year-old man, BP 148/92 on two visits, all labs normal
Q1. Diagnosis: Primary (Essential) Hypertension - Stage 1 (BP ≥140/90 on 2 separate visits, no secondary cause identified)
Q2. Lifestyle Interventions:
- Weight loss (target BMI <25)
- DASH diet (low salt <2g/day, high fruits/vegetables)
- Regular aerobic exercise (30 min/day, 5 days/week)
- Limit alcohol (<2 drinks/day men)
- Stop smoking
- Stress reduction
Q3. First-line Pharmacologic Treatment:
- Thiazide diuretic (e.g., hydrochlorothiazide) — or
- ACE inhibitor (e.g., lisinopril) — or
- ARB (e.g., losartan) — or
- Calcium channel blocker (e.g., amlodipine) (Any of these is acceptable first-line for Stage 1 HTN without comorbidities)
Case 3: Post-amputation — Red, brawny, swollen limb with crepitus in intramuscular planes
(The image shows a surgical wound with crepitus = gas in tissues)
Q1. Diagnosis: Gas Gangrene (Clostridial Myonecrosis)
Q2. Microorganism: Clostridium perfringens (most common, ~80%); also C. septicum, C. novyi
- Gram-positive, anaerobic, spore-forming bacillus
- Produces exotoxins (alpha-toxin - lecithinase) causing muscle necrosis and gas production
Q3. Treatment:
- Emergent surgical debridement - wide excision of ALL necrotic tissue; re-amputation if needed
- IV antibiotics - Penicillin G (first-line) + Clindamycin (inhibits toxin production)
- Hyperbaric oxygen therapy (adjunct - inhibits anaerobic growth)
- Resuscitation (IV fluids, blood transfusion, ICU monitoring)
- Antitoxin (limited availability)
Case 2b: 45-year-old sheep farmer, right upper abdomen lump, hepatomegaly, eosinophilia 12%, USG shows cystic lesion with daughter cysts
Q1. Diagnosis & Organism:
- Hepatic Hydatid Disease (Cystic Echinococcosis)
- Caused by Echinococcus granulosus (tapeworm larval stage)
- Sheep farmer + eosinophilia + hepatomegaly + cystic liver lesion = classic
Q2. Sign Shown (USG):
"Daughter cysts" / Water lily sign - multiple smaller cysts within a large cyst (pathognomonic of hydatid disease on USG)
Q3. Investigation of Choice:
- Abdominal Ultrasound - first-line (WHO classification: CE1-CE5)
- CT Abdomen - better delineation, detects calcification, daughter cysts, biliary communication
- Serology - ELISA for anti-Echinococcus antibodies (confirms diagnosis)
- Note: NEVER aspirate without precaution (risk of anaphylaxis and seeding)
Q4. Treatment:
- If surgery indicated: PAIR procedure (Puncture, Aspiration, Injection of scolicide, Re-aspiration) or surgical cystectomy/pericystectomy
- If not surgery: Albendazole (400 mg BD x cycles) - medical treatment of choice, used preoperatively and for inoperable/small cysts
Case 3: 50-year-old woman, 2 weeks post-knee replacement, sudden dyspnea + pleuritic pain, SpO2 89%, tachycardia, tachypnea, normal CXR
Q1. Most Likely Diagnosis: Pulmonary Embolism (PE)
Classic: sudden dyspnea + pleuritic chest pain + tachycardia + tachypnea + hypoxia + normal CXR + recent surgery (immobility) = PE until proven otherwise.
Q2. Risk Factors:
- Recent surgery (especially orthopaedic/lower limb)
- Immobility (not attending physiotherapy)
- Obesity
- Age >40
- Prior DVT/PE
- Malignancy
- Oral contraceptives/HRT (she is on hormone replacement therapy)
- Hypercoagulable states (thrombophilia)
- Long travel, dehydration
Q3. Confirmatory Tests:
| Test | Role |
|---|---|
| CT Pulmonary Angiography (CTPA) | Gold standard - directly visualizes clot in pulmonary arteries |
| D-dimer | Highly sensitive (if low probability - rules out PE); not specific |
| V/Q scan | Alternative if CTPA contraindicated (renal failure, contrast allergy) |
| Bilateral lower limb Doppler USG | Detects DVT (source of PE) |
| Echocardiogram | Shows RV strain/dilation in massive PE |
| ABG | Hypoxia, hypocapnia, respiratory alkalosis |
| ECG | Sinus tachycardia (most common); S1Q3T3 pattern (classic but rare) |
| Troponin + BNP | Risk stratification of PE severity |

IMG_20260610_111141.jpg
Give short answers
I can see 4 cases. Let me identify them and answer concisely from knowledge — these are all classic presentations.
Case 2: 12-year-old boy, bronchial asthma, severe attack
Q1. Most Likely Diagnosis:
Acute Severe Asthma (Status Asthmaticus)
- Silent chest + accessory muscle use + SpO₂ 86% + peak flow 35% predicted = life-threatening attack
Q2. ABG Pattern Indicating Impending Respiratory Failure:
- pH 7.32 (acidosis) + PaCO₂ 52 mmHg (rising CO₂ = exhaustion)
- Normal/rising PaCO₂ in an asthmatic = Type II respiratory failure (hypercapnic) = impending respiratory arrest
- Worsening acidosis despite oxygen = intubation threshold
Q3. Immediate Treatment Algorithm (ED/ICU):
- High-flow oxygen (target SpO₂ 94-98%)
- Nebulized Salbutamol (every 20 min or continuous) + Ipratropium bromide
- IV/oral Corticosteroids (prednisolone 1-2 mg/kg or IV hydrocortisone)
- IV Magnesium Sulphate (single dose - bronchodilator)
- IV fluids (avoid dehydration)
- Monitor peak flow, SpO₂, ABG
Q4. Criteria for ICU Admission/Intubation:
- Rising PaCO₂ (>45 mmHg) / worsening acidosis
- Deteriorating consciousness / exhaustion
- SpO₂ <92% despite maximal therapy
- Silent chest, cyanosis
- Peak flow <33% predicted
- Failure to respond to initial treatment
Q5. Long-term Prevention After Stabilization:
- Daily inhaled corticosteroid (ICS) (e.g., budesonide) - step-up therapy
- Long-acting beta-2 agonist (LABA) if ICS alone insufficient
- Short-acting beta-2 agonist (SABA) as rescue inhaler
- Identify and avoid triggers (allergens, viral infections, exercise)
- Written asthma action plan
- Regular follow-up + spirometry
- Consider leukotriene receptor antagonist (montelukast)
Case 3: 50-year-old male, dysphagia + halitosis + regurgitation — X-ray shows posterior outpouching at pharyngo-esophageal junction
Q1. Diagnosis:
Pharyngeal (Zenker's) Diverticulum
- Classic triad: dysphagia + halitosis (food stasis) + regurgitation of undigested food
Q2. Investigation:
- Barium swallow (gold standard) — shows posterior pouch at pharyngo-esophageal junction
- Endoscopy (with caution — risk of perforation)
Q3. Anatomical Explanation:
- Occurs at Killian's dehiscence — a natural weak point in the posterior pharyngeal wall between the thyropharyngeus and cricopharyngeus muscles (both parts of inferior pharyngeal constrictor)
- Increased intraluminal pressure during swallowing forces mucosa to herniate through this gap posteriorly → false (pulsion) diverticulum
Q4. Treatment of Choice:
- Endoscopic cricopharyngeal myotomy (with diverticulotomy/septotomy) — minimally invasive, preferred
- Open surgical approach: diverticulectomy + cricopharyngeal myotomy — for large pouches or failed endoscopic treatment
Case 2b: 40-year-old male, recurrent painful nodules on buttocks with serous discharge
(Image shows perianal/buttock region with a sinus opening)
Q1. Diagnosis:
Pilonidal Sinus Disease
- Recurrent painful nodules + serous discharge in natal cleft/buttock region = pilonidal sinus/abscess
Q2. Most Common Type:
Acquired (Primary) Pilonidal Sinus — most common
- Hair penetrates the skin in the natal cleft → foreign body reaction → sinus tract formation
Q3. Classification (Bascom Classification):
| Type | Description |
|---|---|
| Acute pilonidal abscess | Acute infection, fluctuant |
| Chronic pilonidal sinus | Persistent sinus with discharge |
| Complex/recurrent | Multiple sinuses, previous surgery |
(Also: Gupta classification by number and location of pits/openings)
Q4. Investigation of Choice:
- Clinical diagnosis (inspection and probing of sinus tract)
- MRI — if complex/recurrent disease to map extent of sinus tracts
- No routine imaging needed for straightforward cases
Case 3: 5-year-old boy, fever + vomiting + headache + drowsiness + neck stiffness + Kernig's sign + CSF: cloudy, WBC 1800/μL (neutrophils), protein 2.0 g/L, glucose 1.1 mmol/L, Gram-negative diplococci
Q1. Preliminary Diagnosis:
Bacterial Meningitis caused by Neisseria meningitidis (Meningococcal Meningitis)
- Gram-negative diplococci + CSF findings + age + clinical picture = N. meningitidis
Q2. Meaning of Analysis Results:
| CSF Finding | This Patient | Significance |
|---|---|---|
| Appearance | Cloudy | Purulent = bacterial |
| WBC 1800/μL (neutrophils 90%) | ↑↑ | Bacterial (neutrophilic pleocytosis) |
| Protein 2.0 g/L | ↑↑ (normal <0.45) | BBB breakdown, inflammation |
| Glucose 1.1 mmol/L | ↓↓ (normal ~2/3 serum) | Bacteria consuming glucose |
| Serum glucose 5.4 → CSF ratio 0.2 | <0.5 | Confirms bacterial meningitis |
| Gram-negative diplococci | N. meningitidis | Causative organism identified |
Q3. Emergency Therapy:
- IV Ceftriaxone immediately (100 mg/kg/day) — do NOT delay for LP if patient deteriorating
- IV Dexamethasone (0.15 mg/kg q6h x 4 days) — reduces inflammation, prevents complications (deafness)
- IV fluids + monitoring
- Isolation (droplet precautions)
- Notify public health + chemoprophylaxis for close contacts: Rifampicin or Ciprofloxacin
- Monitor for complications: Waterhouse-Friderichsen syndrome, DIC, cerebral herniation
This is a shared conversation. Sign in to Orris to start your own chat.