Central line
Reading File
search_medical_text
central venous catheter types indications placement
search_medical_image
central line catheter anatomy placement sites
GradeResponse
GradeResponse
Here is a comprehensive overview of central lines (central venous catheters, CVCs):
Central Venous Catheters (Central Lines)
Definition
A central line is a catheter placed into a large central vein — typically the superior vena cava (SVC), inferior vena cava (IVC), or right atrium — allowing reliable vascular access for monitoring, infusions, and sampling.
Types
| Type | Description | Best For |
|---|---|---|
| Non-tunneled CVC | Short-term, placed percutaneously at bedside | ICU/acute care |
| Tunneled CVC (e.g., Hickman, Broviac) | Subcutaneous tunnel reduces infection risk; most common long-term option | TPN, chemotherapy, intestinal failure |
| PICC (Peripherally Inserted Central Catheter) | Inserted via arm vein (basilic/cephalic), tip in SVC | Medium-term IV access; lower pneumothorax risk |
| Implanted port | Fully subcutaneous reservoir accessed via needle; lowest infection risk | Infrequent intermittent access (e.g., oncology) |
Per "Management of Central Venous Access in Children With Intestinal Failure" (p. 2), tunneled CVCs are the most common long-term option due to stability and durability. Ports carry lower infection risk but are reserved for infrequent access due to required needle sticks.
Common Insertion Sites
- Internal jugular (IJ) — high success rate, ultrasound-guided preferred
- Subclavian — lower infection rates, higher pneumothorax risk
- Femoral — easiest access in emergencies, highest infection/thrombosis risk
- Axillary — alternative to subclavian with similar landmark
Indications
- Hemodynamic monitoring (CVP, ScvO₂)
- Vasopressor/inotrope infusion
- Total parenteral nutrition (TPN)
- Rapid large-volume resuscitation (introducer sheath)
- Chemotherapy / long-term medications
- Hemodialysis / plasmapheresis
- Poor peripheral access
- Pulmonary artery catheter introduction
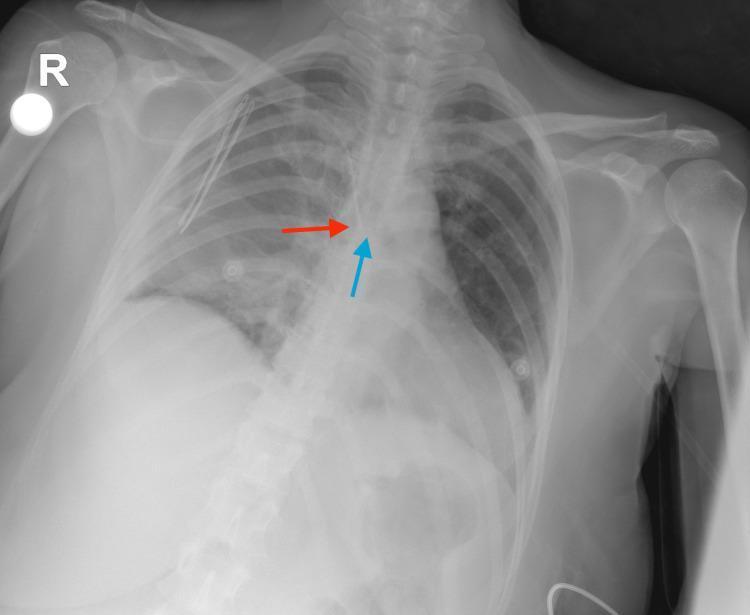
Correct Tip Position
The distal tip should rest at the cavoatrial junction (distal SVC), which radiographically corresponds to just below the carina on chest X-ray.
Complications
Immediate (procedural):
- Pneumothorax (especially subclavian)
- Arterial puncture / hematoma
- Air embolism
- Arrhythmia (tip too deep in right heart)
- Malposition
Delayed:
- CLABSI (Central Line-Associated Bloodstream Infection) — most serious; tunneled CVCs have lower rates than PICCs in adult studies
- Central venous thrombosis
- Catheter occlusion / fibrin sheath
- Venous stenosis (more common with PICCs)
CLABSI Prevention (Bundle)
- Hand hygiene
- Maximal sterile barrier precautions during insertion
- Chlorhexidine skin antisepsis
- Optimal site selection (avoid femoral when possible)
- Daily review of line necessity → remove when no longer needed
PICC vs. Tunneled CVC Trade-offs
- PICC: lower rates of central venous thrombosis, but higher peripheral clot, venous stenosis, line breakage, and site infection/phlebitis risk
- Cuffed PICCs have lower infection, malposition, and thrombus rates vs. uncuffed (p. 2)
- Infection rate comparisons between PICCs and tunneled CVCs are conflicting across studies
Is there a specific aspect you want to go deeper on — insertion technique, troubleshooting, a specific catheter type, or complications management?
Indication of central lines
search_medical_text
central venous catheter indications clinical
GradeResponse
search_medical_text
indications for central line insertion vasopressors TPN hemodialysis monitoring
GradeResponse
Here is a structured breakdown of the indications for central line insertion:
Indications for Central Lines
1. Hemodynamic Monitoring
- Central venous pressure (CVP) measurement
- Central venous oxygen saturation (ScvO₂) monitoring — used to guide resuscitation in shock
- Advanced parameters: cardiac output, stroke volume variation, systemic vascular resistance (via CVC-linked computer algorithms)
- When shock is not quickly resolving or there is a persistent need for vasopressors, a central line is indicated for both monitoring and drug delivery (Harrison's, p. 8172)
2. Vasoactive Drug Administration
- Vasopressors (norepinephrine, vasopressin, phenylephrine) — must be given centrally to avoid peripheral tissue necrosis
- Inotropes (dobutamine, milrinone)
- Concentrated potassium or calcium infusions
3. Poor Peripheral Venous Access
- Patients with difficult or exhausted peripheral veins (e.g., chronic IV drug users, oncology patients, obese patients)
4. Total Parenteral Nutrition (TPN)
- Hyperosmolar formulations are sclerosing to peripheral veins and require a central vessel
5. Renal Replacement Therapy
- Hemodialysis and continuous renal replacement therapy (CRRT) require large-bore, high-flow catheters (dialysis catheters / Vascath)
- Plasmapheresis / therapeutic plasma exchange
6. Chemotherapy & Long-Term Medications
- Vesicant chemotherapy agents must be delivered centrally
- Long-term antibiotics, antifungals, or immunoglobulin infusions
7. Rapid Volume Resuscitation
- Large-bore introducer sheaths (e.g., 8.5 Fr Cordis) allow very rapid fluid delivery in massive hemorrhage or resuscitation scenarios
8. Pulmonary Artery Catheter (PAC) Introduction
- The central sheath provides access for PAC insertion for advanced right heart monitoring
9. Cardiac Pacing
- Temporary transvenous pacing wires are inserted via a central vein (usually internal jugular or subclavian)
10. Aspiration of Air Embolism
- A CVC positioned in the right atrium can be used to aspirate air in suspected air embolism
Key Principle
Lines should be inserted under sterile conditions using a protocolized checklist, and removed as soon as no longer needed to minimize risk of central line-associated bloodstream infection (CLABSI) (Harrison's, p. 8172).
Would you like detail on any specific indication, or move on to contraindications and site selection?
This is a shared conversation. Sign in to Orris to start your own chat.