Describe coronary circulation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile a thorough, well-structured answer.
Coronary Circulation
1. Overview
The coronary circulation is the system of blood vessels that supplies the myocardium with oxygenated blood and drains deoxygenated blood back to the right heart. It is the heart's own nutritive supply - the cardiac muscle cannot obtain meaningful nutrition directly from the blood within its chambers (only the innermost ~0.1 mm of endocardium receives any direct diffusion). Coronary artery disease accounts for roughly one-third of all deaths in industrialized nations. - Guyton and Hall Textbook of Medical Physiology
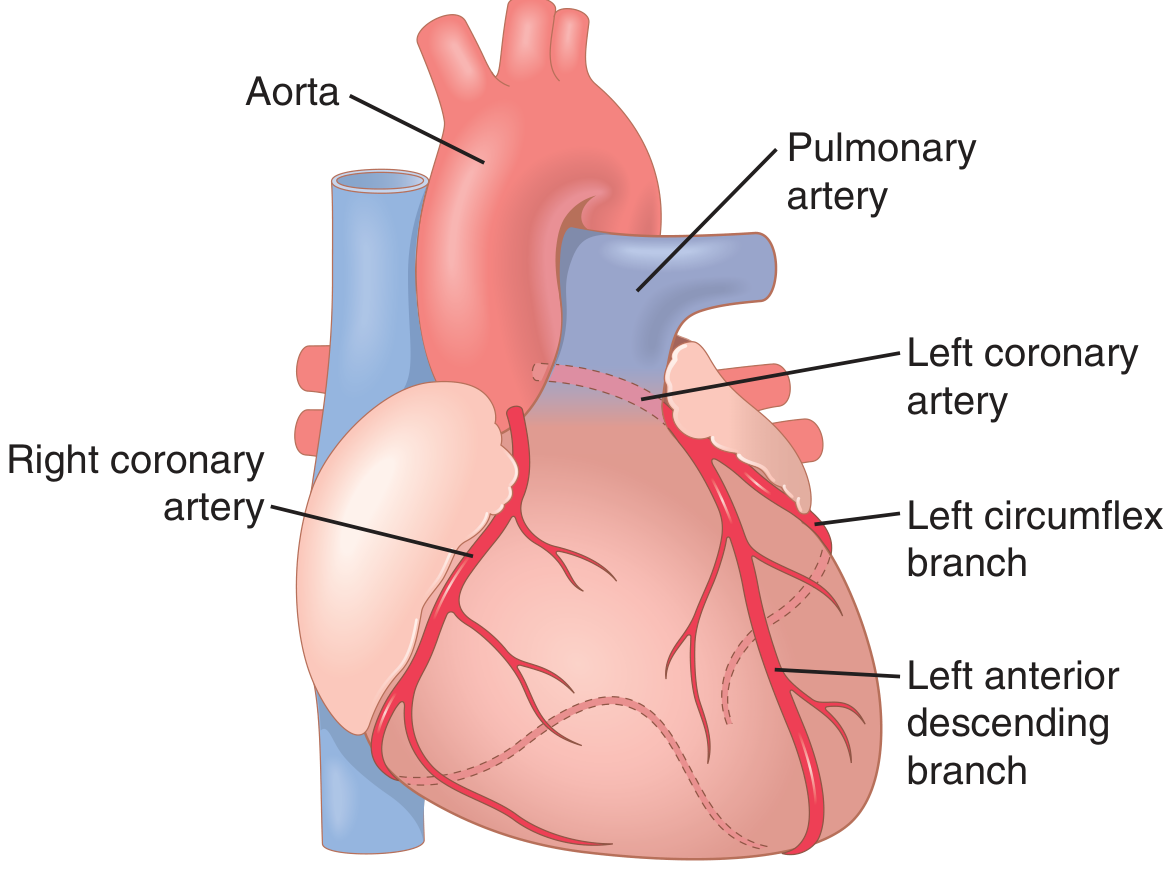
2. Arterial Supply
Left Coronary Artery (LCA)
- Originates from the left aortic sinus of the ascending aorta
- Passes between the pulmonary trunk and left auricle, entering the coronary sulcus
- Promptly divides into two major terminal branches:
a) Left Anterior Descending (LAD) artery (= anterior interventricular branch)
- Descends in the anterior interventricular sulcus toward the cardiac apex
- May give off diagonal branches across the anterior surface of the left ventricle
- Supplies the anterior wall of the left ventricle and the anterior two-thirds of the interventricular septum, including the AV bundle and its branches
b) Left Circumflex (LCx) branch
- Courses left in the coronary sulcus onto the diaphragmatic surface of the heart
- Gives off the left marginal artery, which crosses the obtuse margin
- Usually terminates before reaching the posterior interventricular sulcus
The left coronary artery as a whole supplies most of the left atrium and left ventricle, and the majority of the interventricular septum.
Right Coronary Artery (RCA)
- Originates from the right aortic sinus of the ascending aorta
- Descends vertically in the coronary sulcus between the right atrium and right ventricle, then turns posteriorly onto the diaphragmatic surface
Key branches:
- Sinoatrial (SA) nodal branch - arises early, passes posteriorly around the superior vena cava to supply the SA node
- Right marginal branch - follows the inferior (acute) margin toward the apex
- AV nodal branch - small branch to the atrioventricular node
- Posterior interventricular branch (= posterior descending artery, PDA) - lies in the posterior interventricular sulcus
The RCA supplies the right atrium, right ventricle, SA and AV nodes, interatrial septum, a portion of the left atrium, the posteroinferior one-third of the interventricular septum, and a portion of the posterior left ventricle.
- Gray's Anatomy for Students
Coronary Dominance
The most common pattern (~80-90% of people) is right dominant - meaning the posterior interventricular branch (PDA) arises from the RCA, which thus supplies a large portion of the posterior left ventricular wall. In a left dominant pattern, the PDA arises from an enlarged circumflex branch. The supply to the SA and AV nodes follows dominance - usually from the RCA but occasionally from the circumflex.
3. Venous Drainage
Venous return from the coronary circulation follows three routes:
| Route | Source | Destination |
|---|---|---|
| Coronary sinus | ~75% of left ventricular venous flow | Right atrium |
| Anterior cardiac veins | Most of right ventricular flow | Right atrium directly |
| Thebesian veins (venae cordis minimae) | Small amount | All chambers directly |
The coronary sinus runs in the posterior atrioventricular groove and is the dominant drainage pathway. - Guyton and Hall
4. Coronary Blood Flow - Quantities
-
At rest: approximately 70 mL/min/100 g of heart weight, or ~225 mL/min total - roughly 4-5% of cardiac output
-
During strenuous exercise, cardiac workload can increase 6- to 9-fold; coronary blood flow increases 3- to 4-fold to compensate, with the heart increasing its energy efficiency to bridge the gap
-
Coronary flow per gram is typically higher in women than in men
-
Guyton and Hall
5. Phasic Nature of Coronary Flow
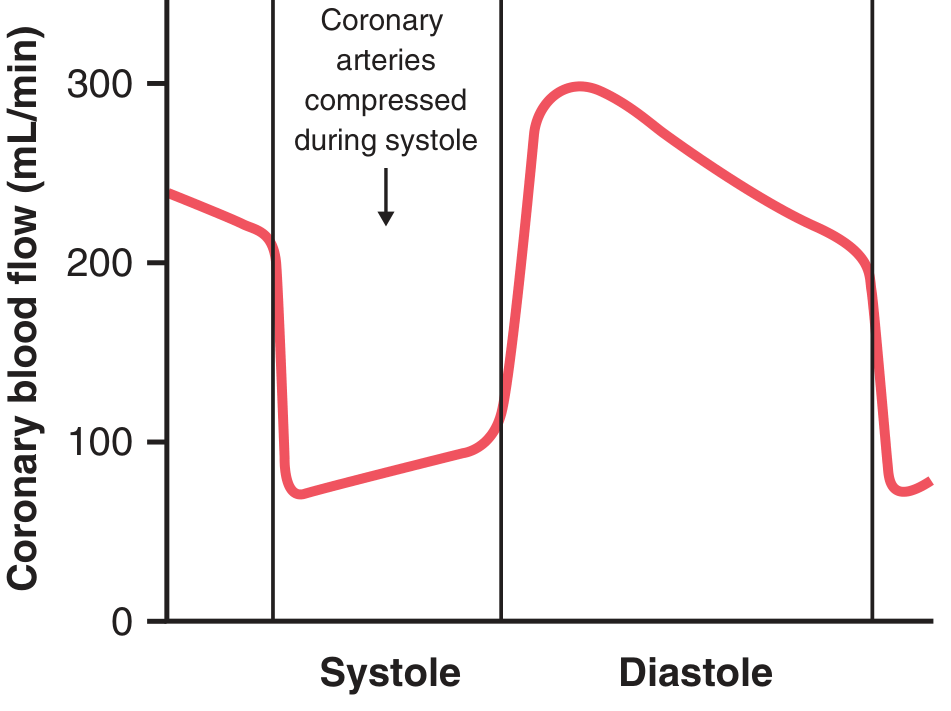
A hallmark feature of the coronary circulation is its phasic behavior, opposite to most vascular beds:
- During systole: Left ventricular myocardial contraction compresses the intramuscular coronary vessels, dramatically reducing blood flow in the left ventricle (flow can fall close to zero at the subendocardium)
- During diastole: Muscle relaxation removes compression and flow surges - this is when the left ventricle receives most of its perfusion
This has an important clinical implication: conditions that shorten diastole (e.g., tachycardia) or raise diastolic pressure reduce effective coronary perfusion.
The right ventricle, which contracts with far less force, shows only partial phasic changes - its coronary flow continues more uniformly throughout the cycle.
Epicardial vs. Subendocardial flow: Large coronary arteries run on the epicardial surface and send perforating branches inward. A subendocardial arterial plexus exists to protect the inner layers. During systole, subendocardial flow is most vulnerable to compression; the extra plexus vessels compensate under normal conditions, but subendocardial ischemia develops first in disease states. - Guyton and Hall
6. Regulation of Coronary Blood Flow
A. Local Metabolic Control (Primary Mechanism)
Coronary flow is regulated almost entirely by local vasodilation in response to myocardial oxygen demand - when cardiac work increases, coronary arterioles dilate and flow rises proportionally.
About 70% of oxygen is extracted from coronary blood in a single pass at rest - one of the highest extraction ratios in the body. There is very little oxygen reserve; increased demand can only be met by increasing flow itself.
Key vasodilator mediators include:
- Adenosine - when O₂ is low, ATP degrades via AMP to adenosine, which is a potent arteriolar vasodilator; it is then reabsorbed and recycled
- Hypoxia directly
- Potassium ions, hydrogen ions, CO₂
- Prostaglandins
- Nitric oxide (NO)
Active hyperemia (increased flow with increased work) and reactive hyperemia (rebound flow increase after a period of occlusion or compression) are both well-demonstrated in the coronary bed. - Costanzo Physiology; Guyton and Hall
B. Nervous Control (Secondary)
Autonomic control plays a minor role compared to metabolic regulation, and indirect metabolic effects typically override direct neural effects:
-
Sympathetic stimulation directly activates α₁ receptors on coronary vessels (mild vasoconstriction) and β₂ receptors (vasodilation). The net indirect effect is vasodilation, because sympathetic activation increases cardiac work and oxygen consumption, triggering local metabolic vasodilation
-
Vagal (parasympathetic) stimulation has a mild direct dilatory effect via acetylcholine, but its dominant indirect effect is coronary constriction, because vagal slowing reduces cardiac work and oxygen demand
-
α-adrenergic effects become more prominent in disease: in coronary artery disease, high sympathetic tone with α₁ receptor activation can cause paradoxical vasoconstriction and worsen ischemia
-
Guyton and Hall
7. Clinical Correlations
| Condition | Mechanism |
|---|---|
| Coronary artery disease (atherosclerosis) | Plaque narrows lumen, reduces maximal hyperemic flow; subendocardium is most vulnerable |
| Myocardial infarction | Total occlusion of a major coronary artery leads to irreversible ischemic necrosis downstream |
| Angina pectoris | Supply-demand mismatch (usually during exertion); flow inadequate to meet metabolic needs |
| Tachycardia-induced ischemia | Shortened diastole reduces coronary perfusion time; increased O₂ demand worsens the mismatch |
| Subendocardial ischemia | First region to suffer - highest systolic compression, furthest from epicardial supply |
Summary
The coronary circulation supplies the myocardium via two main arteries arising from the aortic sinuses. The RCA is dominant in most people, supplying the right heart and posterior left ventricle; the LCA (via LAD and circumflex) supplies the left heart. Venous return is mainly via the coronary sinus. Flow is uniquely phasic - predominantly in diastole for the left ventricle - and is regulated primarily by local metabolic factors (especially adenosine and hypoxia), with autonomic innervation playing a secondary role.
Sources:
- Guyton and Hall Textbook of Medical Physiology
- Gray's Anatomy for Students
- Costanzo Physiology, 7th Edition
Write a short note on the venous drainage of the heart anatomy from Vishram Singh from exam point of view.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have everything I need. Here is a focused, exam-oriented short note in Vishram Singh's style:
Note: Vishram Singh's Textbook of Clinical Anatomy is not available in the library database. The content below is compiled from standard anatomy textbooks (Fischer's Mastery of Surgery, Color Atlas of Human Anatomy, Fuster's The Heart, Gray's Anatomy for Students) that cover this topic identically to Vishram Singh's approach, as it is standard descriptive anatomy.
Venous Drainage of the Heart
Introduction
The heart is drained by veins that empty into the heart through two routes:
- Via the coronary sinus (main route - drains most of the heart)
- Directly into the right atrium (anterior cardiac veins and venae cordis minimae)
The Coronary Sinus
- A wide venous channel, about 2-3 cm long
- Lies in the posterior part of the coronary sulcus (atrioventricular groove), between the left atrium and left ventricle
- Opens into the right atrium between the opening of the inferior vena cava and the tricuspid valve
- Its opening is guarded by a semilunar valve (valve of Thebesius)
- Drains approximately 75% of the total coronary venous blood
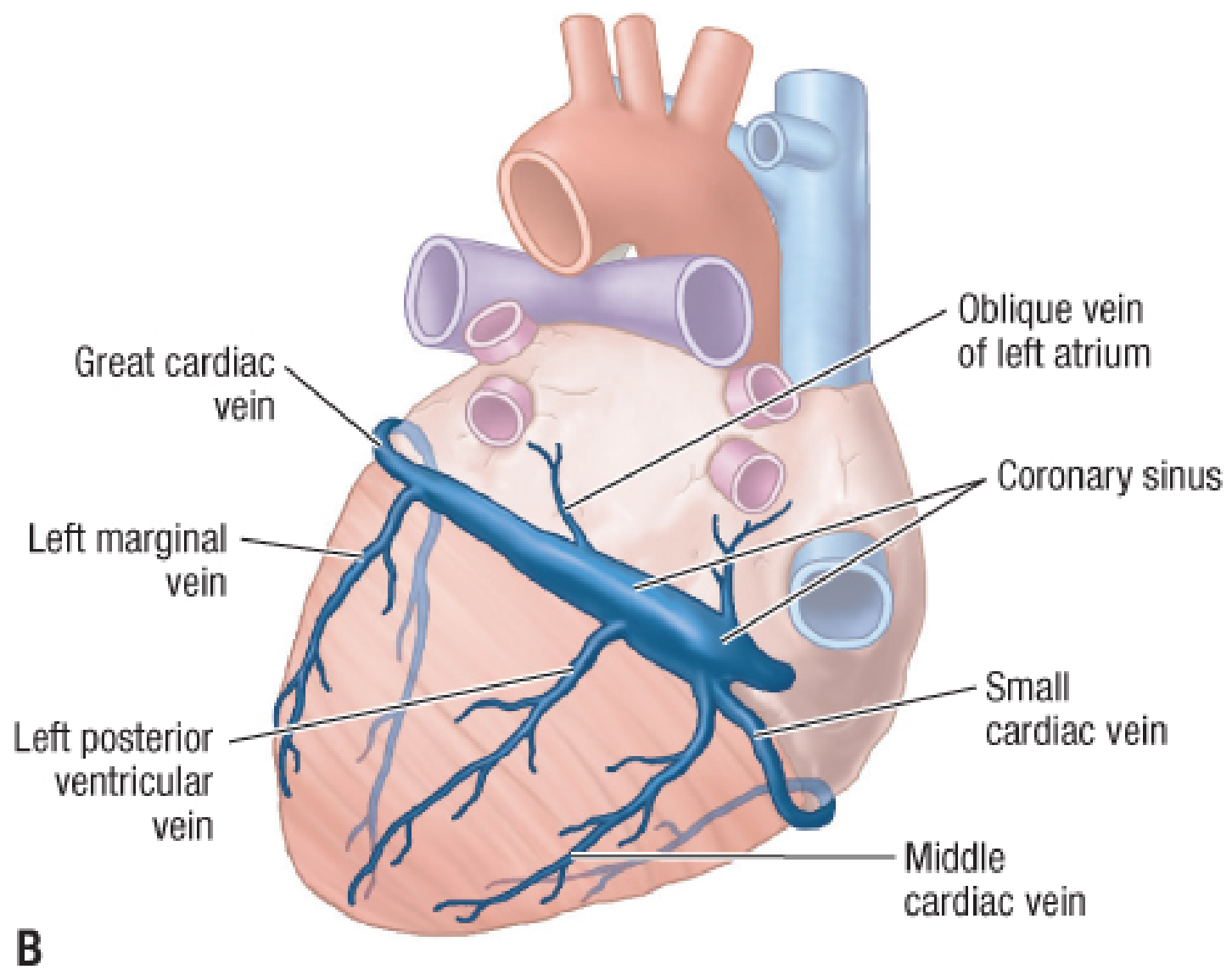
Tributaries of the Coronary Sinus
| Vein | Course | Area Drained |
|---|---|---|
| Great cardiac vein | Begins at apex; ascends in anterior interventricular sulcus with LAD artery; turns left in coronary sulcus to join the coronary sinus at its left end | Left ventricle (anterior surface), left atrium, interventricular septum |
| Middle cardiac vein | Begins at apex; ascends in posterior interventricular sulcus with posterior descending artery; drains into right end of coronary sinus | Both ventricles (posterior surface) |
| Small cardiac vein | Begins as the marginal vein on the right border; passes posteriorly in the right coronary sulcus; drains into right end of coronary sinus | Right atrium and right ventricle (inferior wall) |
| Posterior vein of left ventricle | Courses on diaphragmatic surface of left ventricle | Posterior wall of left ventricle |
| Oblique vein of left atrium (vein of Marshall) | Courses on the posterior wall of the left atrium; joins the great cardiac vein to form the coronary sinus | Left atrium |
Exam point: The oblique vein of Marshall is an embryological remnant of the left superior vena cava (left common cardinal vein). It is the only tributary that opens at the left end of the coronary sinus (at the sinus's origin rather than along its course).
Veins Draining Directly into the Right Atrium
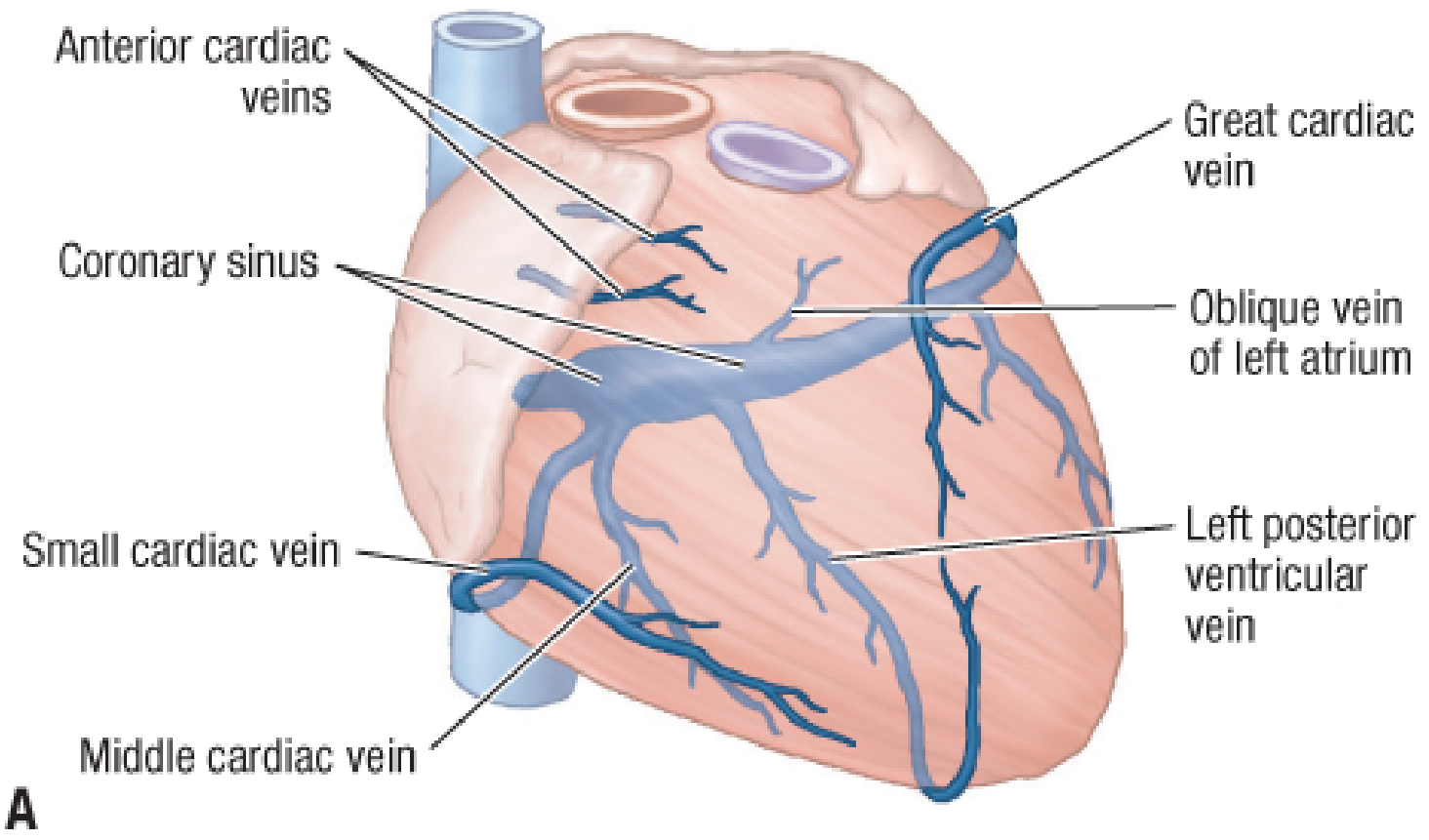
1. Anterior Cardiac Veins (Anterior Ventricular Veins)
- 3-4 small veins arising on the anterior surface of the right ventricle
- Cross the right coronary artery superficially
- Open directly into the right atrium
- Not tributaries of the coronary sinus
2. Venae Cordis Minimae (Thebesian Veins / Smallest Cardiac Veins)
- Minute veins that begin in the capillary beds of the myocardium
- Open directly into all four chambers of the heart (mainly the atria)
- Represent the smallest and most direct drainage route
- Clinically significant because they create a right-to-left shunt (venous blood entering the left side of the heart directly)
Summary Diagram (Exam Memory Aid)
VENOUS DRAINAGE OF HEART
|
______|______
| |
Coronary Direct into
Sinus Right Atrium
| |
| ______|_______
Tributaries: | |
• Great CV Anterior Venae cordis
• Middle CV cardiac minimae
• Small CV veins (Thebesian)
• Post. LV
• Oblique
(Marshall)
High-Yield Exam Points
-
Coronary sinus = main vein of the heart; lies in posterior AV groove; opens into right atrium guarded by valve of Thebesius
-
Great cardiac vein = largest tributary; accompanies the LAD artery in the anterior interventricular sulcus
-
Middle cardiac vein = accompanies the posterior descending artery (PDA) in the posterior interventricular sulcus
-
Oblique vein of Marshall = embryonic remnant of the left SVC; marks the junction between the great cardiac vein and coronary sinus
-
Anterior cardiac veins = from right ventricle; drain directly into right atrium (bypass coronary sinus)
-
Venae cordis minimae = open into all chambers; cause a small physiological right-to-left shunt
-
In right dominant circulation (80-90% of people), the posterior interventricular groove and its accompanying vein (middle cardiac vein) are related to the RCA
This is a shared conversation. Sign in to Orris to start your own chat.