thyroid long answeer
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed for a comprehensive MBBS-level long answer. Let me compile it.
Thyroid Gland — Anatomy & Physiology
MBBS Long Answer
1. Introduction
The thyroid gland is the largest purely endocrine gland in the body. It secretes two iodine-containing hormones — thyroxine (T4) and triiodothyronine (T3) — and calcitonin. These hormones regulate the body's metabolic rate, growth, development, and calcium homeostasis.
2. Embryology
The thyroid originates from two separate embryological precursors:
- Median thyroid anlage — a midline endodermal outgrowth from the floor of the pharynx at the level of the foramen cecum (between the 1st and 2nd pharyngeal pouches), which descends along the thyroglossal duct.
- Lateral thyroid anlage — derivatives of the 4th/5th pharyngeal pouches that contribute the parafollicular C cells (from neural crest origin).
Both fuse to form the definitive single gland. The thyroglossal duct normally obliterates, but remnants can give rise to a thyroglossal duct cyst. A lingual thyroid (failure of descent) is the most common ectopic thyroid.
3. Gross Anatomy
| Feature | Details |
|---|---|
| Location | Anterior neck, at the level of C5–T1 vertebrae |
| Shape | Butterfly-shaped; two lateral lobes connected by an isthmus |
| Weight | ~25–30 g in adults |
| Isthmus | Overlies 2nd–4th tracheal rings |
| Pyramidal lobe | Present in ~50% of individuals; extends superiorly from isthmus |
| Capsule | Dense fibroelastic capsule sending septa into the gland |
Relations
- Anteriorly: Strap muscles (sternohyoid, sternothyroid, thyrohyoid)
- Posteriorly: Trachea, oesophagus, recurrent laryngeal nerves (in the tracheoesophageal groove)
- Superiorly: Larynx (thyroid cartilage)
- Posterolaterally: Carotid sheath contents
- Posterior surface: Four parathyroid glands embedded within (or close to) the gland
Blood Supply
| Vessel | Origin |
|---|---|
| Superior thyroid artery | First branch of external carotid artery |
| Inferior thyroid artery | Thyrocervical trunk (from subclavian) |
| Thyroidea ima (occasional) | Brachiocephalic trunk / aortic arch |
Venous drainage occurs via the superior, middle, and inferior thyroid veins into the internal jugular and brachiocephalic veins. The blood flow is ~5× the gland's weight per minute — among the highest of any organ.
Nerve Supply
- Vasomotor supply from the superior and inferior cervical sympathetic ganglia.
- The external branch of the superior laryngeal nerve runs near the superior pole vessels (risk during thyroidectomy).
- The recurrent laryngeal nerve (branch of vagus) ascends in the tracheoesophageal groove and is at risk during lower-pole dissection.
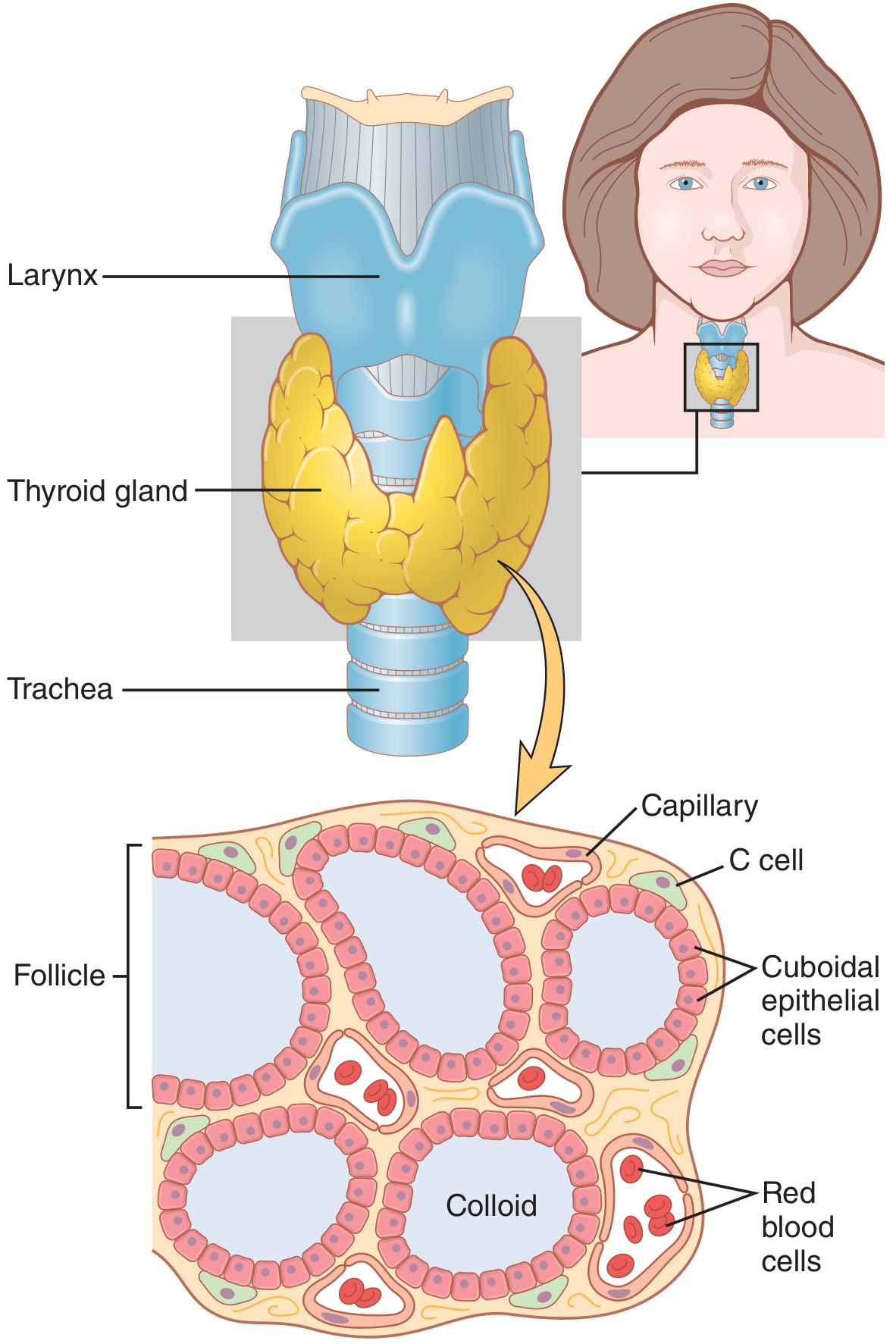
4. Histology
The thyroid contains two epithelial cell types:
a) Follicular cells (Thyrocytes)
- Cuboidal to columnar epithelium lining spherical follicles (100–300 µm diameter)
- Synthesize, store, and secrete T3 and T4
- Active gland: tall columnar cells, scanty colloid
- Inactive gland: flat cells, abundant colloid
b) Parafollicular C cells
- Located in the interfollicular stroma, mainly in the lateral mid-to-upper lobes
- Secrete calcitonin — involved in calcium regulation
- Neural crest origin
Colloid
- Fills the follicular lumen
- Composed chiefly of thyroglobulin (Tg) — a large glycoprotein (MW ~660,000 Da) that serves as the precursor and storage form of thyroid hormones
- Acts as a reservoir; iodine can be stored for 2–3 months' hormone supply
5. Thyroid Hormone Synthesis — Step-by-Step
Iodine Requirement
About 50 mg/year (1 mg/week) of dietary iodine is required. Iodide is absorbed from the GIT, most is excreted by the kidney, and ~1/5 is selectively taken up by the thyroid.
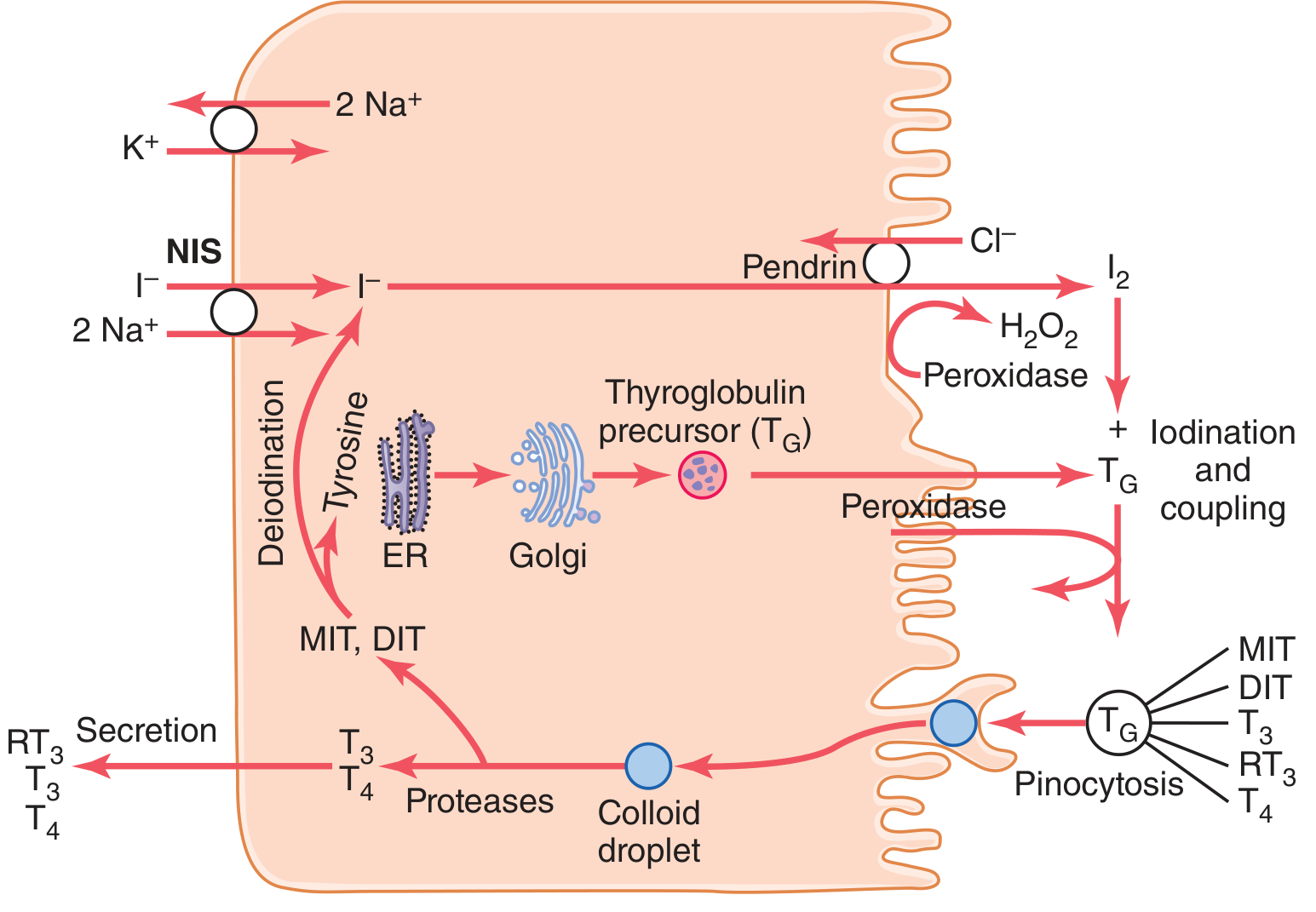
Steps
Step 1 — Iodide Trapping (Active Transport)
- The Na⁺/I⁻ symporter (NIS) on the basolateral membrane of thyrocytes co-transports 1 I⁻ with 2 Na⁺ into the cell, driven by the Na⁺-K⁺-ATPase pump.
- Normal intracellular iodide concentration is ~30× plasma; rises to 250× when maximally stimulated by TSH.
Step 2 — Transfer to Colloid
- Iodide crosses the apical membrane into the follicular lumen via pendrin (a Cl⁻/I⁻ counter-transporter).
Step 3 — Thyroglobulin Synthesis
- Thyrocytes synthesise Tg in the endoplasmic reticulum and Golgi apparatus, then secrete it into the follicular lumen by exocytosis. Each Tg molecule has ~70 tyrosine residues (Ganong's says 123 residues; ~4–8 are actually incorporated into hormones).
Step 4 — Organification (Oxidation + Iodination)
- Thyroid peroxidase (TPO) at the apical membrane oxidises I⁻ → I₂ (nascent iodine) using H₂O₂.
- Iodine attaches to tyrosine residues on Tg:
- 1 iodine + tyrosine → Monoiodotyrosine (MIT)
- 2 iodines + tyrosine → Diiodotyrosine (DIT)
Step 5 — Coupling (Condensation)
- Also catalysed by TPO:
- DIT + DIT → T4 (tetraiodothyronine, thyroxine) + alanine
- MIT + DIT → T3 (triiodothyronine) + alanine
- DIT + MIT → rT3 (reverse T3, biologically inactive)
- In normal thyroid: ~3% MIT, 33% DIT, 35% T4, 7% T3
Step 6 — Storage
- Hormones remain covalently bound within Tg in the colloid.
Step 7 — Endocytosis and Secretion
- On TSH stimulation, thyrocytes endocytose colloid droplets by pinocytosis/endocytosis.
- Lysosomes fuse with colloid droplets; proteases hydrolyse Tg to release free T4, T3, MIT, and DIT.
- Free T4 and T3 diffuse into capillaries.
- MIT and DIT are deiodinated intracellularly by iodotyrosine deiodinase, recycling the iodine.
Key enzyme: Thyroid peroxidase (TPO) is essential for both organification and coupling. Blocked by propylthiouracil (PTU) and carbimazole/methimazole.
6. Daily Secretion
| Hormone | Daily secretion |
|---|---|
| T4 | ~80 µg/day (primary secretory product) |
| T3 | ~4 µg/day |
| rT3 | ~2 µg/day |
7. Transport in Blood
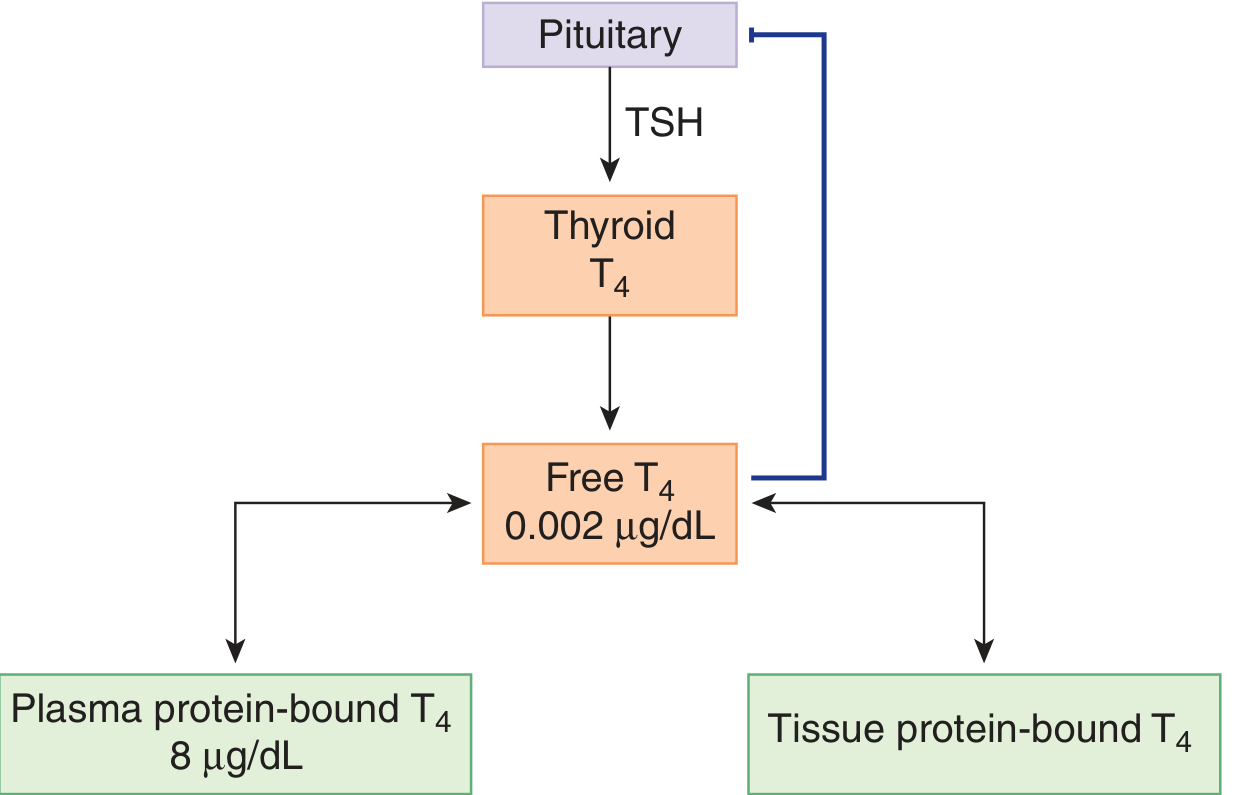
T4 and T3 are highly lipophilic and are transported bound to plasma proteins:
| Protein | T4 bound | Notes |
|---|---|---|
| Thyroxine-binding globulin (TBG) | ~70% | Highest affinity, lowest capacity |
| Transthyretin (TTR/prealbumin) | ~20% | |
| Albumin | ~10% | Lowest affinity, highest capacity |
- 99.98% of T4 is protein-bound; free T4 = only ~2 ng/dL
- 99.8% of T3 is protein-bound (less than T4 → T3 acts faster and has shorter half-life)
- Only free (unbound) hormone is biologically active and exerts negative feedback
Half-life: T4 ~ 7 days; T3 ~ 1 day (due to lesser protein binding)
Factors altering TBG
| Increase TBG | Decrease TBG |
|---|---|
| Oestrogen, pregnancy, OCP | Androgens, glucocorticoids |
| Hepatitis, cirrhosis | Nephrotic syndrome |
| Hypothyroidism | Hyperthyroidism |
Important: Changes in TBG alter total T4/T3 but not free hormone levels (compensatory TSH adjusts output). The patient remains euthyroid.
8. Peripheral Conversion (Metabolism)
- ~80% of circulating T3 is derived from peripheral deiodination of T4 (not direct thyroid secretion)
- Three deiodinase enzymes (all contain selenocysteine):
| Deiodinase | Location | Action |
|---|---|---|
| D1 | Liver, kidney, thyroid, pituitary | T4 → T3 (outer ring removal); maintains T3 pool |
| D2 | Brain, pituitary, placenta, brown fat | T4 → T3 (high affinity); local T3 supply to CNS |
| D3 | Brain, placenta, skin | T4 → rT3; T3 → T2 (inactivation) |
- D1 and D2 remove the 5' iodine (outer ring) → active T3
- D3 removes the 5 iodine (inner ring) → inactive rT3
- In illness, starvation, and surgery: D1 is decreased → more rT3, less T3 (Euthyroid Sick Syndrome / Low T3 syndrome)
9. Mechanism of Action
T3 (and T4 converted to T3 intracellularly) enters the cell and binds to nuclear thyroid hormone receptors (TR-α and TR-β), which are ligand-activated transcription factors. The receptor forms a heterodimer with Retinoid X Receptor (RXR) and binds to Thyroid Hormone Response Elements (TREs) on target genes → activation of gene transcription → new protein synthesis.
Nongenomic actions also exist (rapid effects within minutes): regulation of ion channels, mitochondrial oxidative phosphorylation, activation of cAMP/protein kinase pathways.
More than 90% of cellular thyroid hormone activity is mediated by T3 (higher receptor affinity than T4).
10. Physiological Effects of Thyroid Hormones
A. Metabolic Effects
- Calorigenic effect: Increases BMR by 60–100% when excess; decreases ~50% in absence
- Stimulates Na⁺-K⁺-ATPase → increased oxygen consumption and heat production
- Increases carbohydrate metabolism: enhanced glycolysis, gluconeogenesis, GI glucose absorption, insulin secretion
- Increases fat metabolism: lipid mobilisation, free fatty acid oxidation
- Decreases plasma cholesterol, triglycerides, phospholipids (by upregulating hepatic LDL receptors and increasing biliary cholesterol excretion) — hence hypothyroidism → hypercholesterolaemia
B. Cardiovascular Effects
- Increased cardiac output, heart rate, stroke volume
- Decreased peripheral vascular resistance (due to heat production and vasodilation)
- Thyroid hormones have direct positive chronotropic and inotropic effects on the heart (upregulate β-adrenergic receptors)
C. CNS and Development
- Essential for brain development in fetal life and first 2–3 years of life
- Deficiency → cretinism (mental retardation, short stature, deaf-mutism, coarse features)
- In adults: hypothyroidism → slow mentation, depression; hyperthyroidism → anxiety, tremor
D. Growth
- Promotes linear growth and bone maturation (synergistic with GH and IGF-1)
- Hypothyroidism in children → growth retardation, delayed bone age
- Hyperthyroidism → accelerated bone maturation → premature epiphyseal closure → short final height
E. Reproductive System
- Required for normal menstrual cycles and fertility
- Hypothyroidism → menorrhagia or oligomenorrhoea; hyperthyroidism → oligomenorrhoea or amenorrhoea
F. Neuromuscular
- Excess → muscle weakness, tremor, hyperreflexia
- Deficiency → slowness of movements, delayed relaxation of deep tendon reflexes (Woltman's sign)
G. GI Tract
- Increase motility → hyperthyroidism causes diarrhoea
- Decrease motility → hypothyroidism causes constipation
11. Regulation of Thyroid Hormone Secretion — HPT Axis
Hypothalamus
↓ TRH (thyrotropin-releasing hormone)
Anterior Pituitary
↓ TSH (thyroid-stimulating hormone)
Thyroid Gland
↓ T3 & T4
↑ Negative feedback on both hypothalamus and pituitary
TRH
- Tripeptide (pyro-Glu–His–Pro–NH₂) secreted from the paraventricular nucleus
- Stimulates TSH synthesis and secretion (acts via IP₃/DAG pathway)
- Stimulated by cold (especially in neonates); inhibited by stress and glucocorticoids
TSH
- Glycoprotein (α + β subunits); α subunit shared with LH, FSH, hCG
- Acts via G-protein-coupled receptor → activates adenylyl cyclase (cAMP) and phospholipase C
- Effects on thyroid: ↑ iodide trapping, ↑ Tg synthesis, ↑ organification, ↑ endocytosis of colloid, ↑ T3/T4 release, ↑ vascularity → goitre with prolonged excess
- Normal TSH: 0.4–4.0 mIU/L
- TSH is the best single test for thyroid function (log-linear relationship with free T4)
Negative Feedback
- Free T3 and T4 inhibit TSH and TRH secretion
- The pituitary expresses high levels of D2 deiodinase → converts T4 → T3 locally → the pituitary is largely regulated by T3
- This feedback is exquisitely sensitive; small changes in free T4 cause large, log-linear changes in TSH
Autoregulation (Intrinsic)
- High iodide load initially increases hormone synthesis, but with prolonged excess, organification is blocked — Wolff-Chaikoff effect
- Normal glands escape from this block within ~1–2 weeks
- Diseased glands (e.g., Hashimoto's) may fail to escape → hypothyroidism
12. Calcitonin
- Secreted by parafollicular C cells
- 32-amino acid polypeptide
- Secreted in response to hypercalcaemia
- Actions:
- Inhibits osteoclast activity → decreases bone resorption
- Increases renal calcium and phosphate excretion
- In humans, calcitonin plays a minor role in calcium homeostasis (hyperparathyroidism causes more significant hypercalcaemia than calcitonin deficiency causes hypocalcaemia)
- Clinical importance: Calcitonin is a tumour marker for medullary thyroid carcinoma (MTC)
13. Thyroid Hormone in Pregnancy
- TBG increases due to oestrogen → total T4 and T3 rise
- Free T4 and T3 remain normal → mother is euthyroid
- hCG (peak at 10–12 weeks) has weak TSH-like activity → TSH transiently suppressed in first trimester
- Maternal thyroid hormones cross the placenta and are critical for fetal brain development until the fetal thyroid matures (~12–16 weeks)
- Iodine requirements increase in pregnancy; deficiency → cretinism
14. Euthyroid Sick Syndrome
In critical illness, trauma, starvation, and sepsis:
- Low T3: Decreased D1 activity → less peripheral T4-to-T3 conversion
- Elevated rT3: D3 shunts T4 → rT3 (inactive)
- TSH: Normal or slightly low
- No clinical thyroid dysfunction; T4 supplementation is NOT indicated
- Resolves when the underlying illness resolves
15. Summary Table
| Parameter | Value |
|---|---|
| Weight of thyroid | 25–30 g |
| Iodine requirement | 150 µg/day (WHO), ~50 mg/year |
| Daily T4 secretion | 80 µg |
| Daily T3 secretion | 4 µg |
| % T3 from peripheral conversion | ~87% |
| Free T4 | ~0.002 µg/dL (2 ng/dL) |
| T4 bound to TBG | ~70% |
| T4 half-life | ~7 days |
| T3 half-life | ~1 day |
| Normal TSH | 0.4–4.0 mIU/L |
| NIS concentration ratio (I⁻) | 30× normal; 250× maximal |
References
- Guyton and Hall Textbook of Medical Physiology, 14th Ed., Ch. 77
- Ganong's Review of Medical Physiology, 26th Ed., Ch. 20
- Sabiston Textbook of Surgery, 21st Ed., Ch. 73
This is a shared conversation. Sign in to Orris to start your own chat.