Refernce park textbook of spm John snow role - ,8 marks Appropriate diagrams if needed
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Let me compile the comprehensive 8-mark answer.
John Snow's Role in Epidemiology
(Park's Textbook of Preventive and Social Medicine)
Introduction
John Snow (1813-1858) was an English physician and epidemiologist whose meticulous investigation of cholera epidemics in London between 1848 and 1854 laid the foundation for modern epidemiology. His work established the waterborne transmission of cholera long before the bacteriological era - the causative organism Vibrio cholerae was not identified until 1884 by Robert Koch. Park's SPM refers to him as a classic example across multiple epidemiological concepts.
1. Rise of Public Health (Historical Contribution)
Cholera, often called the "father of public health", appeared repeatedly in the western world during the 19th century. John Snow studied the epidemiology of cholera in London from 1848 to 1854 and established the role of polluted drinking water in the spread of cholera. This discovery was all the more remarkable because the causative agent had not yet been identified. His work generated public demand for clean water and contributed directly to sanitary reforms and public health legislation.
2. The Classic Epidemic Investigation - Golden Square, 1854
The Setting
In September 1854, a severe cholera epidemic broke out in the Golden Square district (Soho), London.
Method - Spot Mapping
Snow used a spot map (geographic distribution) to plot every fatal cholera case on a street map of the area. This technique revealed a striking clustering of cases around a single point. The cluster was centered on the Broad Street water pump.
Here is the original spot map from Park's textbook:
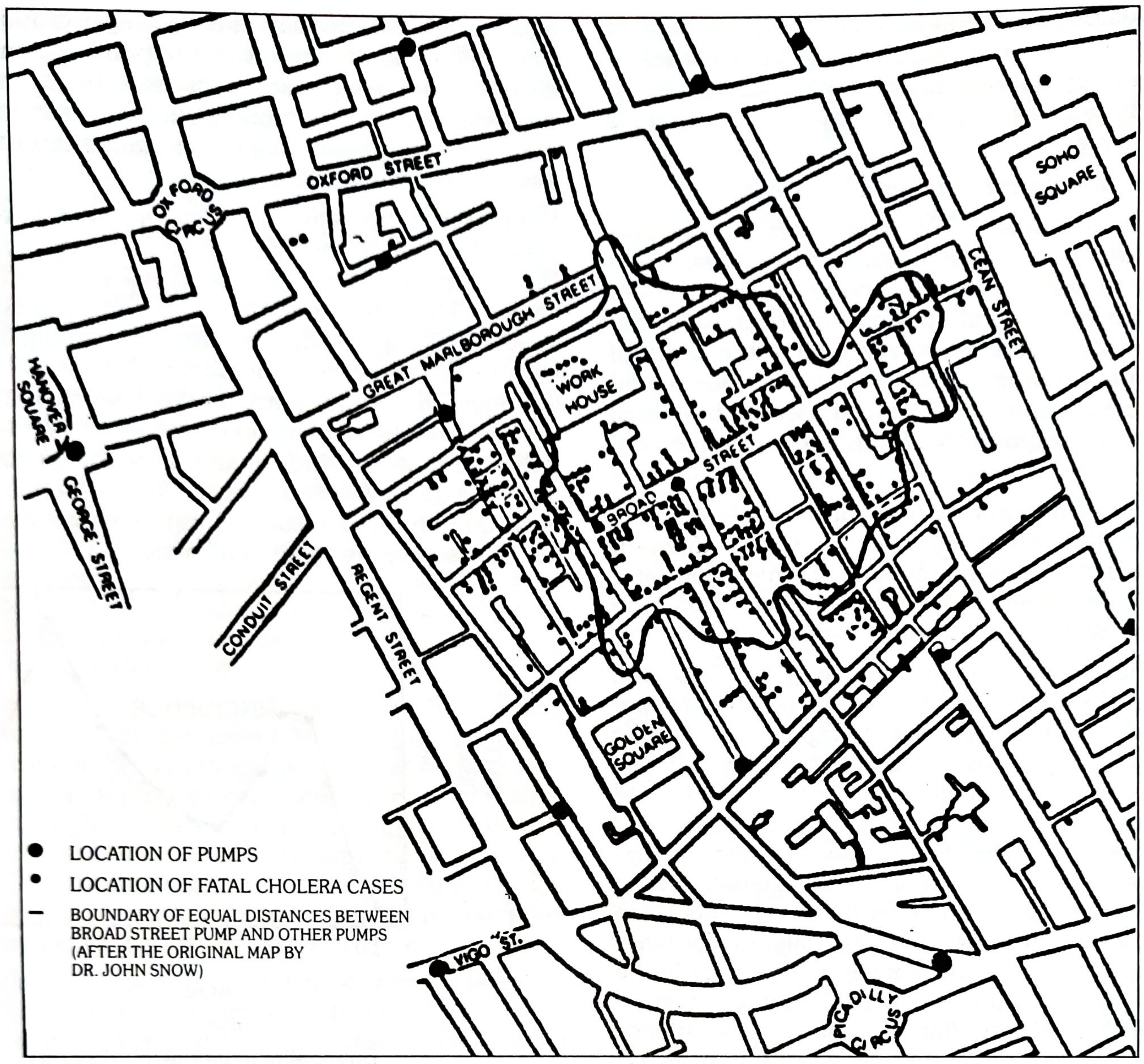
Fig. 6 - Spot map of Asiatic cholera in London (after the original map by Dr. John Snow). Filled circles = location of pumps; dotted areas = location of fatal cholera cases; boundary lines = equal distances from Broad Street pump and other pumps.
Action Taken - Removal of the Pump Handle
Based on this spot map analysis, Snow concluded that the Broad Street pump was the source of infection. He persuaded the local authorities to remove the handle of the pump, thereby cutting off the source of contaminated water. This single public health action controlled the epidemic - the classic example cited in Park's for disease control by breaking the weakest link in the chain of transmission.
"The classic example is that of John Snow controlling the cholera epidemic in London, by removing the handle of the incriminated water pump."
- Park's Textbook of Preventive and Social Medicine
3. The "Grand Experiment" - Natural Experiment
Snow's work is also the classic example of a natural experiment in epidemiology. He identified two randomly mixed populations in London that were alike in all important respects except their source of water supply.
| Source of Water Supply | Number of Houses | Deaths from Cholera | Deaths per 10,000 Houses |
|---|---|---|---|
| Southwark & Vauxhall Co. (sewage-polluted Thames) | 40,046 | 1,263 | 315 |
| Lambeth Co. (clean intake above London) | 26,107 | 98 | 37 |
(Data from London, 1853 - Table 23, Park's SPM)
Inference: The Lambeth company drew water from the River Thames well above London (clean), whereas the Southwark and Vauxhall company drew from a sewage-polluted basin. The great difference in cholera mortality gave clear demonstration that cholera is a waterborne disease - long before the advent of bacteriology.
This also constitutes a "before and after comparison study" - Snow's investigation of cholera in 1854 is cited alongside James Lind's scurvy studies (1750) and the Salk/Sabin polio vaccines as classic examples of this study design.
4. Epidemiological Contributions - Summary
| Contribution | Significance |
|---|---|
| Spot mapping of cases | Pioneered geographic/place distribution analysis in descriptive epidemiology |
| Identification of water source | Established waterborne transmission without knowing the causative agent |
| Removal of pump handle | Classic intervention by breaking the chain of transmission |
| Natural experiment design | Forerunner of analytical epidemiology |
| Before-and-after study | Early example of quasi-experimental epidemiological study design |
5. Significance in Descriptive Epidemiology - Place Distribution
Park's cites Snow's work under "Local Distributions" as the foundational example of place-related epidemiological analysis:
"It was by such a study (spot map of fatal cases), John Snow of England in his classic investigation of cholera epidemic in 1854 in the Golden Square district of London was able to focus attention on the common water pump in Broad Street as the source of infection."
This showed that when a spot map shows clustering of cases, it may suggest a common source of infection or a shared risk factor. The same principle later helped Maxcy hypothesize a rodent reservoir for typhus fever (1920s) and identify AIDS as an infectious disease through clustering by sexual contact and blood product use.
Summary
John Snow's role, as described in Park's SPM, spans multiple domains:
- Historian of public health - helped trigger sanitary reforms
- Pioneer epidemiologist - used spot maps and natural experiments before germ theory
- Public health interventionist - proved that removing a single weak link (the pump handle) can control an epidemic even without complete aetiological knowledge
- Methodologist - laid groundwork for descriptive epidemiology, natural experiments, and before-after study designs
His work remains the most frequently cited historical example throughout Park's SPM, appearing in chapters on history of public health, descriptive epidemiology, study designs, disease prevention, and epidemic investigation.
Source: Park's Textbook of Preventive and Social Medicine (Park's SPM), relevant blocks from ISBN 9789382219163
Add a note on chain of transmission of disease
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the material needed. Here is the comprehensive note on the chain of transmission, directly from Park's SPM:
NOTE: Chain of Transmission of Disease
(Park's Textbook of Preventive and Social Medicine)
Definition and Overview
Communicable diseases are transmitted from the reservoir/source of infection to a susceptible host. Park's SPM describes the medical model of an infectious disease as having three fundamental links in the chain of transmission:

FIG. 16 - Chain of Infection (Park's Textbook of Preventive and Social Medicine)
"Basically there are three links in the chain of transmission, viz, the reservoir, modes of transmission and the susceptible host."
Link 1: Source or Reservoir of Infection
Source of infection is defined as "the person, animal, object or substance from which an infectious agent passes or is disseminated to the host."
Reservoir is defined as "any person, animal, arthropod, plant, soil or substance in which an infectious agent lives and multiplies, on which it depends primarily for survival, and where it reproduces itself in such manner that it can be transmitted to a susceptible host."
Note: Reservoir and source are not always the same. Example - in typhoid fever, the reservoir is a case or carrier, but the source may be contaminated food, milk or water.
Types of Reservoir:
| Type | Examples |
|---|---|
| Human reservoir (most important) | Cases (clinical/subclinical) and Carriers (healthy, incubatory, convalescent, chronic) |
| Animal reservoir (zoonoses) | Rabies (dog/bat), brucellosis (cattle), plague (rats) |
| Non-living reservoir | Soil - tetanus, histoplasmosis; Water - cholera, typhoid |
Homologous reservoir - another member of the same species (e.g., man for cholera).
Heterologous reservoir - infection from another species (e.g., animals/birds for salmonellosis).
Link 2: Modes of Transmission
Infectious agents travel from reservoir to susceptible host via two broad routes:
A. Direct Transmission
| Route | Description | Examples |
|---|---|---|
| Direct contact | Skin-to-skin, mucosa-to-mucosa, sexual intercourse | STDs, AIDS, leprosy |
| Droplet infection | Spray of droplets during coughing/sneezing (range: 30-60 cm, particles >5 µm) | Common cold, TB, COVID-19, diphtheria |
| Contact with soil | Exposure to infective agents in soil | Tetanus, hookworm |
| Inoculation into skin/mucosa | Needle-stick, bites, cuts | Hepatitis B, rabies |
| Transplacental (vertical) | Mother to fetus across placenta | Congenital rubella, HIV, syphilis |
B. Indirect Transmission
| Route | Description | Examples |
|---|---|---|
| Vehicle-borne | Contaminated water, food, milk, blood, fomites | Cholera, typhoid, hepatitis A |
| Vector-borne (mechanical) | Passive carriage by arthropod (no multiplication) | Flies carrying typhoid |
| Vector-borne (biological) | Multiplication/development in vector | Malaria (mosquito), plague (flea) |
| Airborne - droplet nuclei | Evaporated droplets (<5 µm) that float in air | TB, measles, chickenpox |
| Airborne - dust | Dried secretions in dust particles | Q fever, histoplasmosis |
| Fomite-borne | Inanimate objects (utensils, clothing, instruments) | Smallpox, trachoma |
| Unclean hands and fingers | Faecal-oral route via unwashed hands | Dysentery, hepatitis A |
As a rule, an infectious disease is transmitted by only one route (e.g., typhoid by vehicle), but some can use multiple routes (e.g., AIDS, hepatitis B, salmonellosis) - enhancing the agent's survival.
Link 3: The Susceptible Host
The third and final link. A susceptible host is a person who lacks sufficient immunity to resist infection. Susceptibility depends on:
- Age, sex, nutritional status
- Genetic/constitutional factors
- Previous exposure or immunization
- Immune status (immunosuppression, HIV, etc.)
Breaking the Chain - Disease Control
Every disease has weak points susceptible to attack. The basic principle is to identify and break the weakest link. This is where John Snow's contribution is directly relevant:
"The classic example is that of John Snow controlling the cholera epidemic in London, by removing the handle of the incriminated water pump." - breaking the mode of transmission (vehicle-borne - contaminated water) without even knowing the causative agent.
Control measures at each link:
| Link | Control Strategy |
|---|---|
| Reservoir | Early diagnosis, notification, isolation, treatment, quarantine, surveillance, disinfection |
| Mode of transmission | Water treatment, food hygiene, vector control, hand washing, environmental sanitation |
| Susceptible host | Active immunization, passive immunization, chemoprophylaxis, health education, nutrition improvement |
"Although effective control of a disease requires knowledge of its multifactorial causation, removal or elimination of a single known essential link or the weakest link may be sufficient to control a disease, even if complete knowledge about the aetiology is lacking."
Control measures should not be delayed because of incomplete or lack of accurate aetiological knowledge - as Snow himself demonstrated in 1854.
Source: Park's Textbook of Preventive and Social Medicine, ISBN 9789382219163 - Chapter on Dynamics of Disease Transmission and Disease Prevention & Control
Don't use tables on u r own use only if they are present in park and now generate another response
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the content I need. Here is the full rewritten response - no self-made tables, written in flowing text exactly as Park's presents it.
NOTE: Chain of Transmission of Disease
(Park's Textbook of Preventive and Social Medicine)
Overview
Communicable diseases are transmitted from the reservoir/source of infection to a susceptible host. Park's SPM illustrates this as the medical model of an infectious disease (Fig. 16). Basically there are three links in the chain of transmission:
- The Reservoir / Source of Infection
- Modes of Transmission
- The Susceptible Host
FIG. 16 - Chain of Infection (Park's SPM)
LINK 1: Sources and Reservoir
The starting point for the occurrence of a communicable disease is the existence of a reservoir or source of infection.
The source of infection is defined as "the person, animal, object or substance from which an infectious agent passes or is disseminated to the host."
A reservoir is defined as "any person, animal, arthropod, plant, soil or substance (or combination of these) in which an infectious agent lives and multiplies, on which it depends primarily for survival, and where it reproduces itself in such manner that it can be transmitted to a susceptible host." In short, the reservoir is the natural habitat in which the organism metabolizes and replicates.
The terms reservoir and source are not always synonymous. For example, in hookworm infection the reservoir is man, but the source of infection is the soil contaminated with infective larvae. In tetanus, the reservoir and source are the same - soil. In typhoid fever, the reservoir may be a case or carrier, but the source may be faeces, urine, or contaminated food, milk or water.
The term homologous reservoir is applied when another member of the same species is the victim - e.g., man is the principal reservoir for Vibrio cholerae. The term heterologous is applied when the infection is derived from a reservoir other than man - e.g., animals and birds infected with salmonella.
The reservoir may be of three types:
1. Human Reservoir
By far the most important source or reservoir of infection for humans is man himself. He may be a case or a carrier. Man is often described as his own enemy because most communicable diseases are contracted from human sources.
- A case is defined as "a person in the population or study group identified as having the particular disease, health disorder or condition under investigation." Cases may be clinical (manifest) or subclinical (inapparent/missed).
- A carrier is a person who harbours the infectious agent without clinically recognizable illness and serves as a source of infection. Types include: healthy carriers, incubatory carriers, convalescent carriers, and chronic carriers (e.g., typhoid Mary).
2. Animal Reservoir
When an infectious disease is transmissible under natural conditions from vertebrate animals to man, the disease is called a zoonosis. Examples include rabies (dog/bat), brucellosis (cattle), plague (rodents), and leptospirosis.
3. Reservoir in Non-Living Things
Some infectious agents live and multiply in soil, water or other inanimate matter. For example, tetanus and gas gangrene organisms survive in soil; Legionella in water cooling systems.
LINK 2: Modes of Transmission
Communicable diseases may be transmitted from the reservoir or source to a susceptible individual in many different ways, depending upon the infectious agent, portal of entry and local ecological conditions. As a rule, an infectious disease is transmitted by only one route (e.g., typhoid fever by vehicle transmission, common cold by direct contact). However, some are transmitted by several routes - e.g., AIDS, salmonellosis, hepatitis B, brucellosis - which enhances the survival of the infectious agent.
The mode of transmission may be classified as:
A. Direct Transmission
- Direct contact
- Droplet infection
- Contact with soil
- Inoculation into skin or mucosa
- Transplacental (vertical)
(1) Direct contact: Infection transmitted by direct contact from skin to skin, mucosa to mucosa, or mucosa to skin - e.g., touching, kissing, sexual intercourse. This reduces the time the organism must survive outside the host and ensures a larger dose of infection. Diseases: STDs, AIDS, leprosy, leptospirosis, skin and eye infections.
(2) Droplet infection: Direct projection of a spray of droplets of saliva and nasopharyngeal secretions during coughing, sneezing, or speaking. Droplet spread is limited to a distance of 30-60 cm between source and host. Particles of 10 µm or greater are filtered by the nose; those 5 µm or less penetrate deeply to the alveoli. Diseases: respiratory infections, eruptive fevers, common cold, diphtheria, whooping cough, tuberculosis, COVID-19, meningococcal meningitis.
FIG. 17 - Droplets sprayed into the air from a sneeze
(3) Contact with soil: The disease agent is acquired by direct exposure of susceptible tissue to the agent in soil, compost or decaying vegetable matter - e.g., tetanus, mycoses, hookworm larvae.
(4) Inoculation into skin or mucosa: The disease agent is inoculated directly into the skin or mucosa - e.g., rabies virus by dog bite, hepatitis B through contaminated needles and syringes.
(5) Transplacental (vertical) transmission: Disease agents transmitted transplacentally. Examples include the TORCH agents (Toxoplasma gondii, rubella virus, cytomegalovirus, herpes virus), varicella, syphilis, hepatitis B, and AIDS. Some non-living agents (e.g., thalidomide) can also be transmitted vertically, producing malformations of the embryo.
B. Indirect Transmission
This embraces a variety of mechanisms including the traditional 5 F's - "flies, fingers, fomites, food and fluid." An essential requirement is that the infectious agent must be capable of surviving outside the human host in the external environment and retain pathogenicity until it finds a new host.
(1) Vehicle-borne: Transmission through water, food (including raw vegetables, fruits, milk and milk products), ice, blood, serum, plasma, or other biological products such as tissues and organs. The agent may multiply in the vehicle (e.g., S. aureus in food) or be passively carried (e.g., hepatitis A virus in water). Diseases: acute diarrhoeas, typhoid, cholera, polio, hepatitis A, food poisoning, intestinal parasites (water/food); hepatitis B, malaria, syphilis (blood).
(2) Vector-borne: Two types -
- Mechanical transmission: The infectious agent is mechanically transported by a crawling or flying arthropod through soiling of feet or proboscis, or passage through its gastrointestinal tract. There is no development or multiplication of the agent within the vector - e.g., housefly carrying typhoid bacilli.
- Biological transmission: The agent undergoes replication or development (or both) within the vector, which requires an incubation period before transmission. Three subtypes:
- Propagative - agent merely multiplies but no change in form (e.g., plague bacilli in rat fleas)
- Cyclo-propagative - agent changes in both form and number (e.g., malaria parasites in mosquito)
- Cyclo-developmental - agent undergoes development but no multiplication (e.g., microfilaria in mosquito)
(3) Airborne:
- Droplet nuclei - tiny particles (1-10 microns range) representing the dried residue of droplets. They remain airborne for long periods and are disseminated by air currents. Particles in the 1-5 micron range are drawn into the alveoli and retained. Diseases: tuberculosis, influenza, chickenpox, measles, Q fever, COVID-19, many respiratory infections.
- Dust - larger droplets settle on floors, furniture, bedding and become part of dust. Tubercle bacilli may survive in dust for considerable periods. Diseases transmitted via infected dust particles.
(4) Fomite-borne: Transmission through inanimate objects (fomites) such as soiled clothing, bedding, toys, surgical instruments, dressings. Diseases: smallpox, trachoma.
(5) Unclean hands and fingers: Faecal-oral route through failure to wash hands after defaecation or before handling food - e.g., dysentery, hepatitis A, typhoid.
LINK 3: The Susceptible Host
The third link in the chain of transmission is the susceptible host or people at risk. They may be protected by one or more of the following strategies:
(1) Active immunization: Strengthening host defences by active immunization - one of the most powerful and cost-effective weapons of modern medicine. Some diseases are controlled solely by immunization (e.g., polio, tetanus, diphtheria, measles). By reducing the number of susceptibles in the community, it augments herd immunity, making infection more difficult to spread.
(2) Passive immunization: Providing ready-made antibodies (immunoglobulins) for immediate short-term protection - e.g., post-exposure prophylaxis for rabies, hepatitis B.
(3) Chemoprophylaxis: Use of drugs to prevent infection or disease in susceptible individuals - e.g., antimalarials, INH for tuberculosis contacts.
Breaking the Chain - The John Snow Connection
The basic approach in controlling disease is to identify the weak points and break the weakest link in the chain of transmission. A major aspect of communicable disease control relates to "breaking the chain of transmission" or interruption of transmission (Fig. 16).
"The classic example is that of John Snow controlling the cholera epidemic in London, by removing the handle of the incriminated water pump."
Although effective control requires knowledge of multifactorial causation, removal of a single known essential link - the weakest link - may be sufficient to control a disease, even if complete knowledge about the aetiology is lacking. This is the foundational lesson John Snow demonstrated in 1854: control measures should not be delayed because of incomplete aetiological knowledge.
Source: Park's Textbook of Preventive and Social Medicine, ISBN 9789382219163 - Chapter: Dynamics of Disease Transmission and Disease Prevention & Control
No need of this much large trim a few points
Got it. Here is a trimmed, focused version:
Chain of Transmission of Disease
(Park's Textbook of Preventive and Social Medicine)
Communicable diseases are transmitted from the reservoir/source of infection to a susceptible host. Basically there are three links in the chain of transmission - the reservoir, modes of transmission, and the susceptible host.
FIG. 16 - Chain of Infection (Park's SPM)
Link 1: Sources and Reservoir
The source of infection is defined as "the person, animal, object or substance from which an infectious agent passes or is disseminated to the host."
A reservoir is defined as "any person, animal, arthropod, plant, soil or substance in which an infectious agent lives and multiplies, on which it depends primarily for survival, and where it reproduces itself in such manner that it can be transmitted to a susceptible host."
The terms reservoir and source are not always synonymous - e.g., in typhoid fever the reservoir is the case or carrier, but the source may be contaminated food or water.
The reservoir may be of three types:
1. Human reservoir - the most important. Man may be a case (clinical or subclinical) or a carrier - a person who harbours the agent without clinically recognizable illness. Carrier types include: healthy, incubatory, convalescent, and chronic carriers.
2. Animal reservoir (Zoonoses) - infection naturally transmissible from vertebrate animals to man, e.g., rabies (dog/bat), brucellosis (cattle), plague (rodents).
3. Non-living reservoir - agents that live in soil or water, e.g., tetanus in soil, Legionella in water.
Link 2: Modes of Transmission
As a rule, an infectious disease is transmitted by only one route, but some (e.g., AIDS, hepatitis B, salmonellosis) use multiple routes, enhancing agent survival.
A. Direct Transmission
- Direct contact - skin-to-skin, mucosa-to-mucosa; e.g., STDs, leprosy, AIDS
- Droplet infection - spray of droplets during coughing/sneezing, limited to 30-60 cm; particles ≤5 µm penetrate alveoli; e.g., TB, COVID-19, diphtheria
- Contact with soil - e.g., tetanus, mycoses
- Inoculation into skin/mucosa - e.g., rabies by dog bite, hepatitis B by needles
- Transplacental (vertical) - TORCH agents, syphilis, hepatitis B, AIDS
B. Indirect Transmission
Embraces the traditional 5 F's - "flies, fingers, fomites, food and fluid." The agent must survive outside the host in the external environment.
- Vehicle-borne - water, food, blood, biological products; e.g., cholera, typhoid, hepatitis A
- Vector-borne
- Mechanical - agent passively carried on arthropod feet/proboscis, no multiplication; e.g., housefly carrying typhoid
- Biological - agent multiplies or develops within vector; three subtypes: propagative (plague in rat fleas), cyclo-propagative (malaria in mosquito), cyclo-developmental (microfilaria in mosquito)
- Airborne - droplet nuclei (1-10 microns, float in air; e.g., TB, measles) and dust (settled dried secretions; e.g., Q fever)
- Fomite-borne - inanimate objects like soiled clothing, bedding, instruments; e.g., smallpox, trachoma
- Unclean hands and fingers - faecal-oral route; e.g., dysentery, hepatitis A
Link 3: The Susceptible Host
The third link is the susceptible host or people at risk. Protection strategies include:
- Active immunization - augments herd immunity by reducing the number of susceptibles in the community; e.g., polio, tetanus, diphtheria
- Passive immunization - ready-made antibodies for immediate short-term protection; e.g., post-exposure rabies, hepatitis B
- Chemoprophylaxis - drugs to prevent infection; e.g., antimalarials, INH for TB contacts
Breaking the Chain - John Snow's Lesson
The basic approach in disease control is to identify and break the weakest link in the chain. This is the principle John Snow applied in 1854 - by removing the handle of the Broad Street pump, he broke the vehicle-borne transmission link and controlled the cholera epidemic, without even knowing the causative organism.
"Although effective control requires knowledge of multifactorial causation, removal of a single known essential link may be sufficient to control a disease, even if complete knowledge about the aetiology is lacking."
- Park's SPM
Source: Park's Textbook of Preventive and Social Medicine, ISBN 9789382219163

1000046835.png
Refer park for given questions in pictures for 4 marks each
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here are all 12 VSAQ answers (4 marks each), directly from Park's SPM, no self-made tables:
VSAQs - 4 Marks Each
(Park's Textbook of Preventive and Social Medicine)
1. PQLI (Physical Quality of Life Index)
The concept of quality of life is difficult to define and even more difficult to measure. The Physical Quality of Life Index (PQLI) consolidates three indicators:
- Infant mortality
- Life expectancy at age one
- Literacy
These three components measure the results rather than inputs, and lend themselves to international and national comparison. For each component, the performance of individual countries is placed on a scale of 0 to 100, where 0 represents an absolutely defined "worst" performance and 100 represents the "best." The composite index is calculated by averaging the three indicators, giving equal weight to each of them. The resulting PQLI is also scaled 0 to 100.
PQLI has not taken per capita GNP into consideration, showing that "money is not everything." For example, the oil-rich countries of the Middle East with high per capita incomes have not very high PQLIs. At the other extreme, Sri Lanka and Kerala state in India have low per capita incomes with high PQLIs. PQLI does not measure economic growth; it measures the results of social, economic and political policies. The ultimate objective is to attain a PQLI of 100.
2. HDI (Human Development Index)
HDI is defined as "a composite index focusing on three basic dimensions of human development":
- To lead a long and healthy life - measured by life expectancy at birth
- The ability to acquire knowledge - measured by mean years of schooling and expected years of schooling
- The ability to achieve a decent standard of living - measured by gross national income per capita in PPP US$
The concept of HDI reflects achievements in the most basic human capabilities - leading a long life, being knowledgeable and enjoying a decent standard of living. The HDI values range between 0 to 1. The HDI value for a country shows the distance already travelled towards the maximum possible value of 1, and also allows comparisons with other countries.
HDI is a more comprehensive measure than per capita income alone. Income is only a means to human development, not an end. By focusing on areas beyond income and treating income as a proxy for a decent standard of living, the HDI provides a more comprehensive picture of human life than income does.
3. Rehabilitation and Types
Rehabilitation has been defined as "the combined and coordinated use of medical, social, educational and vocational measures for training and retraining the individual to the highest possible level of functional ability." It includes all measures aimed at reducing the impact of disabling and handicapping conditions and at enabling the disabled and handicapped to achieve social integration - the active participation of disabled and handicapped people in the mainstream of community life.
Types (Areas of concern in rehabilitation):
(a) Medical rehabilitation - restoration of function.
(b) Vocational rehabilitation - restoration of the capacity to earn a livelihood.
(c) Social rehabilitation - restoration of family and social relationships.
(d) Psychological rehabilitation - restoration of personal dignity and confidence.
The current view is that the responsibility of the doctor does not end when the "temperature touches normal and stitches are removed." The patient must be restored and retrained "to live and work within the limits of his disability but to the hilt of his capacity." Examples include: schools for the blind, provision of aids for the crippled, reconstructive surgery in leprosy, muscle re-education in neurological disorders. The purpose of rehabilitation is to make productive people out of non-productive people.
4. Monitoring and Surveillance
According to standard dictionaries, these words are almost synonymous, but in public health practice they have taken on rather specific and somewhat different meanings.
Monitoring is defined as "the performance and analysis of routine measurements aimed at detecting changes in the environment or health status of population." Examples include monitoring of air pollution, water quality, growth and nutritional status. In management, monitoring refers to the episodic oversight of the implementation of an activity, seeking to ensure that input deliveries, work schedules, targeted outputs and other required actions are proceeding according to plan.
Surveillance is defined as - continuous analysis, interpretation, and feedback of systematically collected data, generally using methods distinguished by their practicality, uniformity, and rapidity rather than by accuracy or completeness. By observing trends in time, place, and persons, changes can be observed or anticipated and appropriate action - including investigative or control measures - can be taken. Sources of data may include mortality and morbidity reports, hospital records, laboratory diagnosis, outbreak reports, vaccine uptake and side effects, sickness absence records, changes in disease agents, vectors or reservoirs, and serological surveillance through serum banks.
Surveillance programmes can assume any character - epidemiological surveillance, demographic surveillance, nutritional surveillance, etc. Monitoring is one specific and essential part of the broader concept embraced by surveillance. Surveillance requires professional analysis and sophisticated judgement of data leading to recommendations for control activities.
5. Social Medicine
The term "social medicine" was first introduced by Jules Guerin, a French physician, in 1848. In 1911, the concept was revived by Alfred Grotjahn of Berlin who stressed the importance of social factors as determinants of health and disease.
By derivation, social medicine is "the study of man as a social being in his total environment." It is concerned with all the factors affecting the distribution of health and ill-health in populations, including the use of health services. Social medicine is not a new branch of medicine, but rather an extension of the public health idea reflecting the strong relationship between medicine and social sciences.
Professor Crew of Edinburgh defined it as: "Social medicine stands upon two pillars, medicine and sociology... The laboratory to practice social medicine is the whole community; the tools for diagnosing community ills are epidemiology and biostatistics; and social therapy does not consist in administration of drugs, but social and political action for the betterment of conditions of life of man."
Social medicine had achieved academic respectability in England when John Ryle was appointed professor of social medicine at Oxford. The pre-eminent concern of social medicine has been the development of epidemiological methods and their application to the investigation of disease.
6. Sentinel Surveillance
No routine notification system can identify all cases of infection or disease. A method for identifying the missing cases and thereby supplementing the notified cases is required - this is known as "sentinel surveillance."
The sentinel data is extrapolated to the entire population to estimate the disease prevalence in the total population. The advantages of such a system are:
- Reporting biases are minimized
- Feedback of information to the providers is simplified
Sentinel surveillance agencies could be interested and competent physicians (or institutions) in selected areas who report the cases of disease in their areas. This system provides more valuable and detailed information than could be obtained from the traditional notification system. These sentinel sites could be developed into a notification system for providing more detailed information, which in some settings may be less costly than developing and maintaining an ongoing notification system.
7. Impairment, Disability and Handicap
The sequence of events is stated as:
Disease → Impairment → Disability → Handicap
The WHO has defined these terms as follows:
(i) Impairment: "Any loss or abnormality of psychological, physiological or anatomical structure or function" - e.g., loss of foot, defective vision or mental retardation. An impairment may be visible or invisible, temporary or permanent, progressive or regressive. One impairment may lead to "secondary" impairments - as in leprosy where damage to nerves (primary impairment) may lead to plantar ulcers (secondary impairment).
(ii) Disability: Because of an impairment, the affected person may be unable to carry out certain activities considered normal for his age and sex. Disability has been defined as "any restriction or lack of ability to perform an activity in the manner or within the range considered normal for a human being."
(iii) Handicap: As a result of disability, the person experiences certain disadvantages in life and is not able to discharge obligations required of him. Handicap is defined as "a disadvantage for a given individual, resulting from an impairment or a disability, that limits or prevents the fulfilment of a role that is normal (depending on age, sex, and social and cultural factors) for that individual."
While impairment (earliest stage) has a large medical component, disability and handicap (later stages) have large social and environmental components in terms of dependence and social cost.
8. Contributions of Louis Pasteur
Louis Pasteur (1822-1895) was a French bacteriologist whose contributions marked a turning point in the history of medicine.
- In 1860, he demonstrated the presence of bacteria in air and disproved the theory of "spontaneous generation."
- In 1873, Pasteur advanced the "Germ Theory of Disease."
- His discoveries (along with Robert Koch) confirmed the germ theory and ushered in the golden age of bacteriology - microbe after microbe was discovered in quick succession.
- Pasteur's specific contributions to preventive medicine include: anti-rabies treatment (1883), cholera vaccine (1892), diphtheria antitoxin (1894), and anti-typhoid vaccine (1898).
- He also contributed to antiseptics and disinfectants.
- The process of pasteurization of milk - an enduring public health measure - is named after him.
His work caused all attention to focus on microbes and their role in disease causation. The germ theory supplanted earlier theories and medicine finally "shed the rags of dogma and superstition and put on the robes of scientific knowledge."
9. Contributions of Edward Jenner
Edward Jenner (1749-1823) of Great Britain was a pupil of John Hunter. He discovered vaccination against smallpox in 1796, marking the beginning of a new era - the era of disease prevention by specific measures.
His contribution was all the more remarkable because it came into existence before the causative agents of disease were known. Jenner observed that milkmaids who contracted cowpox did not develop smallpox and used this observation to develop vaccination.
His discovery of vaccination against smallpox, along with James Lind's work on scurvy, marked the birth of preventive medicine. Eventually, following the global immunization programme based on Jenner's principle, smallpox was declared eradicated in 1977 - the first and only disease to be eradicated from the world to date.
10. Lifestyle and Health
The term "lifestyle" is a diffuse concept often used to denote "the way people live," reflecting a whole range of social values, attitudes and activities. It is composed of cultural and behavioural patterns and lifelong personal habits (e.g., smoking, alcoholism) that have developed through processes of socialization. Lifestyles are learnt through social interaction with parents, peer groups, friends, siblings, school and mass media.
Health requires the promotion of healthy lifestyle. A considerable body of evidence indicates an association between health and the lifestyle of individuals. Many current-day health problems especially in developed countries - coronary heart disease, obesity, lung cancer, drug addiction - are associated with lifestyle changes. In developing countries such as India where traditional lifestyles persist, risks are connected with lack of sanitation, poor nutrition, personal hygiene and cultural patterns.
It may be noted that not all lifestyle factors are harmful. Many can actually promote health - examples include adequate nutrition, enough sleep and sufficient physical activity. In short, the achievement of optimum health demands adoption of healthy lifestyles. Health is both a consequence of an individual's lifestyle and a factor in determining it.
11. Germ Theory of Disease
For long, man was groping in darkness about the causation of disease. Several theories were advanced - the supernatural theory, the theory of humors, the theory of contagion, the miasmatic theory (which attributed disease to noxious air and vapours), and the theory of spontaneous generation.
The breakthrough came in 1860 when Louis Pasteur demonstrated the presence of bacteria in air and disproved spontaneous generation. In 1873, Pasteur advanced the "Germ Theory of Disease." In 1877, Robert Koch (1843-1910) showed that anthrax was caused by a bacterium. The discoveries of Pasteur and Koch confirmed the germ theory.
This was the golden age of bacteriology. Microbe after microbe was discovered - gonococcus (1847), typhoid bacillus and pneumococcus (1880), tubercle bacillus (1882), cholera vibrio (1883), diphtheria bacillus (1884), and so on. All attention was focused on microbes and their role in disease causation. The germ theory came to the forefront, supplanting earlier theories. Medicine finally shed the rags of dogma and superstition and put on the robes of scientific knowledge.
However, the germ theory eventually gave place to the newer concept of "multifactorial causation" of disease, as modern diseases like cancer, cardiovascular disease and mental illness could not be explained on the basis of the germ theory alone.
12. Sullivan's Index
Sullivan's Index refers to Disability-Free Life Expectancy (DFLE), also known as active life expectancy. It is defined as "the average number of years an individual is expected to live free of disability if current pattern of mortality and disability continue to apply."
It is a "person-type" disability indicator that combines mortality data and disability prevalence to give a single composite measure of population health. It represents the number of years a person can expect to live without disability.
This concept is related to HALE (Health-Adjusted Life Expectancy), which was formerly called disability-adjusted life expectancy (DALE). HALE is based on life expectancy at birth but includes an adjustment for time spent in poor health. It is most easily understood as "the equivalent number of years in full health that a newborn can expect to live based on current rates of ill-health and mortality."
Sullivan's index is useful because it supplements conventional mortality and morbidity indicators, as death rates alone have not changed markedly despite massive health expenditures. It reflects both the quantity and quality of life in a population.
Source: Park's Textbook of Preventive and Social Medicine, ISBN 9789382219163
Describe briefly no need of this much
Got it - brief and to the point, 4 marks each.
VSAQs – Brief Answers (4 Marks Each)
(Park's Textbook of Preventive and Social Medicine)
1. PQLI (Physical Quality of Life Index)
PQLI consolidates three indicators:
- Infant mortality
- Life expectancy at age one
- Literacy
Each component is placed on a scale of 0 to 100. The composite index is the average of the three, giving equal weight to each. PQLI does not measure economic growth - it measures the results of social, economic and political policies. It has not taken per capita GNP into consideration, showing "money is not everything." The ultimate objective is to attain a PQLI of 100.
2. HDI (Human Development Index)
HDI is a composite index focusing on three basic dimensions:
- Long and healthy life - measured by life expectancy at birth
- Knowledge - measured by mean and expected years of schooling
- Decent standard of living - measured by GNI per capita (PPP US$)
HDI values range from 0 to 1. It is a more comprehensive measure than per capita income alone, as income is only a means to human development, not an end.
3. Rehabilitation and Types
Rehabilitation is defined as "the combined and coordinated use of medical, social, educational and vocational measures for training and retraining the individual to the highest possible level of functional ability."
Types:
- (a) Medical rehabilitation - restoration of function
- (b) Vocational rehabilitation - restoration of capacity to earn a livelihood
- (c) Social rehabilitation - restoration of family and social relationships
- (d) Psychological rehabilitation - restoration of personal dignity and confidence
The purpose is to make productive people out of non-productive people.
4. Monitoring and Surveillance
Monitoring - "the performance and analysis of routine measurements aimed at detecting changes in the environment or health status of population." It is episodic and uses standardized procedures.
Surveillance - continuous analysis, interpretation and feedback of systematically collected data using methods distinguished by practicality, uniformity and rapidity. By observing trends in time, place and persons, changes can be anticipated and appropriate action taken.
Monitoring is one specific and essential part of the broader concept embraced by surveillance. Surveillance requires professional analysis and sophisticated judgement leading to recommendations for control.
5. Social Medicine
Term first introduced by Jules Guerin (1848). Revived by Alfred Grotjahn of Berlin (1911) who stressed social factors as determinants of health and disease.
Defined as "the study of man as a social being in his total environment." It stands on two pillars - medicine and sociology (Prof. Crew). It is not a new branch of medicine but a new orientation, reflecting the strong relationship between medicine and social sciences. Its pre-eminent concern has been the development of epidemiological methods and their application to disease investigation.
6. Sentinel Surveillance
No routine notification system can identify all cases. Sentinel surveillance is a method for identifying the missing cases and supplementing the notified cases.
Sentinel data is extrapolated to the entire population to estimate total disease prevalence. Sentinel agencies are interested and competent physicians or institutions in selected areas who report cases. Advantages: reporting biases are minimized and feedback to providers is simplified. It can be less costly than maintaining a full ongoing notification system.
7. Impairment, Disability and Handicap
Sequence: Disease → Impairment → Disability → Handicap
- Impairment - "any loss or abnormality of psychological, physiological or anatomical structure or function" e.g., loss of foot, defective vision.
- Disability - "any restriction or lack of ability to perform an activity in the manner or within the range considered normal for a human being."
- Handicap - "a disadvantage for a given individual, resulting from an impairment or a disability, that limits or prevents the fulfilment of a role that is normal for that individual."
Impairment has a large medical component; disability and handicap have large social and environmental components.
8. Contributions of Louis Pasteur
- (1860) - Demonstrated bacteria in air; disproved the theory of spontaneous generation
- (1873) - Advanced the Germ Theory of Disease
- Together with Koch, confirmed germ theory and ushered in the golden age of bacteriology
- Developed anti-rabies treatment (1883), cholera vaccine (1892), diphtheria antitoxin (1894), anti-typhoid vaccine (1898)
- Pasteurization of milk is named after him - an enduring public health measure
9. Contributions of Edward Jenner
- Edward Jenner (1749-1823) of Great Britain, pupil of John Hunter
- Discovered vaccination against smallpox in 1796 - before causative agents of disease were known
- Observed that milkmaids who contracted cowpox did not develop smallpox
- His discovery marked the beginning of the era of disease prevention by specific measures
- Based on his principle, the global smallpox eradication programme was carried out and smallpox was declared eradicated in 1977 - the first disease ever eradicated
10. Lifestyle and Health
Lifestyle denotes "the way people live" - a whole range of social values, attitudes and activities; composed of cultural and behavioural patterns and lifelong personal habits learnt through socialization.
A considerable body of evidence shows an association between health and lifestyle. Many current-day health problems - coronary heart disease, obesity, lung cancer, drug addiction - are associated with lifestyle changes. Not all lifestyle factors are harmful; adequate nutrition, sleep and physical activity promote health. Achievement of optimum health demands adoption of healthy lifestyles. Health is both a consequence of lifestyle and a factor in determining it.
11. Germ Theory of Disease
Earlier theories of disease included supernatural theory, theory of humours, miasmatic theory and spontaneous generation. The breakthrough came when:
- (1860) - Pasteur demonstrated bacteria in air, disproved spontaneous generation
- (1873) - Pasteur advanced the Germ Theory of Disease
- (1877) - Robert Koch showed anthrax was caused by bacteria
This ushered in the golden age of bacteriology. Key discoveries: typhoid bacillus, pneumococcus (1880), tubercle bacillus (1882), cholera vibrio (1883), diphtheria bacillus (1884). The germ theory supplanted all earlier theories. However, it later gave place to the concept of multifactorial causation, as modern diseases like cancer and cardiovascular disease could not be explained by germ theory alone.
12. Sullivan's Index
Sullivan's Index refers to Disability-Free Life Expectancy (DFLE), also called active life expectancy. Defined as "the average number of years an individual is expected to live free of disability if current patterns of mortality and disability continue to apply."
It is related to HALE (Health-Adjusted Life Expectancy) - formerly called DALE - which is the equivalent number of years in full health that a newborn can expect to live based on current rates of ill-health and mortality. It supplements conventional mortality data by reflecting both the quantity and quality of life in a population.
Source: Park's Textbook of Preventive and Social Medicine, ISBN 9789382219163
This is a shared conversation. Sign in to Orris to start your own chat.