tell me the highland arteriosclerosis in case of hypertension, and because of this, usually the aorta is very thick in the initial or proximal 10 centimeters of the aorta. I'm not sure, but let me, I mean, you can correct me. So as the aorta is very thick in the proximal part because of high stress region over there, because immediately coming from the heart, the initial part of the aorta has to be thick to bear the high shearing stress. So in a fact that it is thick, the oxygen diffusion capacity along the wall will be decreased because the second later parts of media and adventitia cannot sufficiently diffuse the oxygen from the lumen because it's very thick. Hence, we have vasa vasorum close to the inner part or the outer part of the adventitia through which the media and the adventitia gets its sufficient blood supply from. So in case of some malignant, in case of some hypertension, not malignant, in case of hypertension, usually there is highly arteriosclerosis of the vasa vasorum which will lead to weakness of the media and which can cause aortic dissections. Can you explain that concept in short and concise with cleatr concept like a USMLE topper?
aorta wall layers vasa vasorum media adventitia intima diagram
Hypertension → Vasa Vasorum Arteriosclerosis → Aortic Dissection
The Core Chain of Events
Systemic HTN
↓
Arteriosclerosis / hyaline thickening of vasa vasorum arterioles
↓
Ischemia of outer aortic media
↓
SMC loss + elastic fiber fragmentation ("medial degeneration")
↓
Weakened media → intimal tear → aortic dissection
Step-by-Step Concept
1. Why the proximal aorta is thick-walled
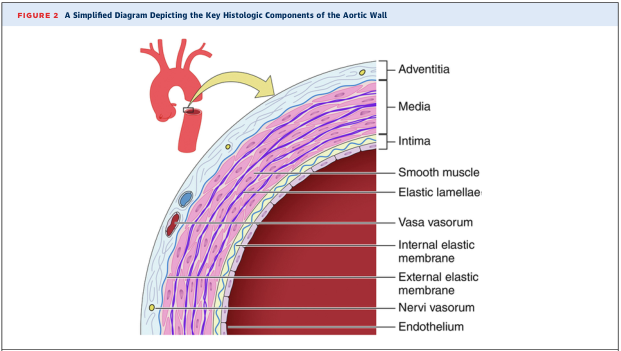
2. The oxygen diffusion problem — why vasa vasorum exist
"Vasa vasorum is present along the adventitia and outer one-third of the media." — Robbins, Cotran & Kumar: Pathologic Basis of Disease
3. What hypertension does to the vasa vasorum
- Narrowing of vasa vasorum lumens → reduced perfusion of the outer media
- Ischemia of the outer media → SMC death, fragmentation of elastic fibers
- Accumulation of mucoid/proteoglycan matrix in place of lost SMCs/elastic fibers
"Systemic hypertension can also cause significant narrowing of arterioles of the vasa vasorum (e.g., in the aorta), which causes outer medial ischemia." — Robbins, Cotran & Kumar: Pathologic Basis of Disease, p. 476
4. Medial degeneration → aortic dissection
- Loss of SMCs and elastic lamellae
- Replacement by basophilic mucoid ground substance
- Structural weakness of the media
Your One Correction
USMLE Mnemonic Summary
| Feature | Detail |
|---|---|
| Site | Ascending aorta (Type A dissection) |
| Risk factor | Chronic hypertension (#1) |
| Mechanism | HTN → arteriosclerosis of vasa vasorum → medial ischemia → SMC/elastic fiber loss → medial degeneration |
| Histology | "Cystic medial necrosis" (mucoid degeneration, elastic fragmentation) |
| Endpoint | Intimal tear → blood dissects medial plane → dissection |
| Other causes of same histology | Marfan syndrome (fibrillin-1 defect → TGF-β excess), Loeys-Dietz, Ehlers-Danlos type IV |