Metformin which class of drug and why first line use?
Reading File
Finding Sources
Searching PubMed
metformin type 2 diabetes first-line treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Here is a complete, textbook-referenced answer:
Metformin - Drug Class and First-Line Status
Drug Class
Metformin is a biguanide - a class of oral antihyperglycemic agents. It is the only biguanide still in clinical use; its predecessor phenformin was withdrawn in 1978 due to a high incidence of severe lactic acidosis. - Brenner and Rector's The Kidney
Mechanism of Action
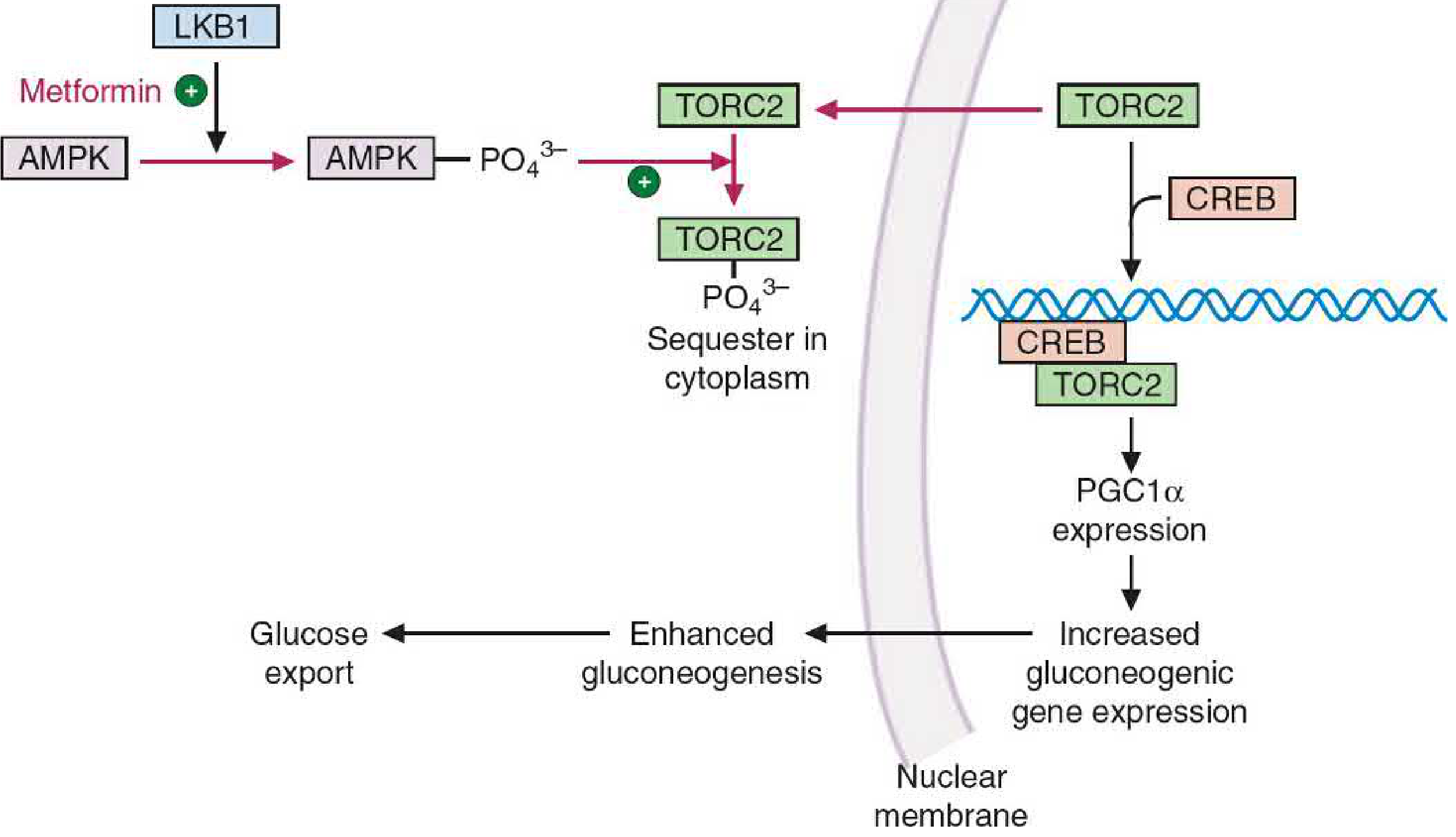
Metformin works primarily through activation of AMPK (AMP-activated protein kinase) via stimulation of the upstream kinase LKB1. This produces several downstream effects:
Three core actions:
| Action | How |
|---|---|
| Inhibits hepatic gluconeogenesis | AMPK phosphorylates TORC2, sequestering it in cytoplasm, blocking CREB-PGC1α transcription of gluconeogenic enzymes (G6Pase, PEPCK) |
| Increases peripheral glucose uptake | AMPK activation enhances muscle glucose uptake via GLUT4 translocation |
| Reduces hepatic lipogenesis | AMPK inhibits acetyl-CoA carboxylase and SREBP-1, reducing fatty acid and cholesterol synthesis |
The net effect: reduced fasting blood glucose and HbA1c without stimulating insulin secretion. - Basic Medical Biochemistry, 6e; Harrison's Principles of Internal Medicine 22E
Why Is It First-Line for Type 2 Diabetes?
Metformin is the most widely used antidiabetic drug in the world and is recommended as first-line therapy by virtually all major guidelines (ADA, EASD, WHO) for the following reasons:
-
No hypoglycemia risk - Because it does not stimulate insulin secretion (it is an insulin sensitizer, not a secretagogue), it does not cause hypoglycemia when used alone.
-
Weight-neutral or modest weight loss - Unlike sulfonylureas or insulin, metformin does not cause weight gain - a significant benefit in the predominantly overweight/obese T2DM population. - Brenner and Rector's The Kidney
-
Cardiovascular safety - The landmark UKPDS trial demonstrated reduced cardiovascular mortality in overweight T2DM patients treated with metformin, a benefit not seen with sulfonylureas or insulin.
-
Long safety record - Over 30 years of clinical use. - Basic Medical Biochemistry, 6e
-
Low cost - Generic availability makes it highly accessible globally.
-
Additional metabolic benefits - Lowers LDL and triglycerides via AMPK-mediated inhibition of lipogenesis; reduces HbA1c by 1-1.5%.
-
Emerging benefits - Harrison's 22E (2025) notes metformin also activates mTOR inhibition (via AMPK) and the transcription factor Nrf2, which may contribute to anti-aging and potentially anti-cancer properties.
Key Pharmacokinetics to Know
- Not metabolized by the liver; excreted unchanged by renal tubular secretion
- Requires dose reduction or cessation in renal impairment (eGFR < 30 mL/min) due to risk of accumulation and lactic acidosis (MALA)
- Small molecule (165 Da), large volume of distribution (3 L/kg) - binds mitochondrial membranes intracellularly
Summary Table
| Property | Detail |
|---|---|
| Class | Biguanide |
| Primary mechanism | AMPK activation → inhibits hepatic gluconeogenesis |
| Hypoglycemia | No (monotherapy) |
| Weight effect | Neutral to slight loss |
| Renal caution | Avoid if eGFR < 30 (lactic acidosis risk) |
| Evidence basis | UKPDS, 30+ years clinical use |
Recent literature note: A 2026 systematic review (PMID 41401897) confirms metformin's additional benefit of reducing central arterial stiffness in T2DM patients, adding further cardiovascular rationale for its first-line use.
Why Preferred anti-diabetic drugs in Type 2 Diabetes with CKD?
Finding Sources
Searching PubMed
antidiabetic drugs type 2 diabetes chronic kidney disease
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading Article
PMID: 41203232
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive textbook and trial data. Here is the full answer:
Preferred Anti-Diabetic Drugs in Type 2 Diabetes with CKD
Managing T2DM in CKD requires careful drug selection because: (1) some agents accumulate in renal failure and become toxic, (2) some agents offer active kidney and cardiovascular protection beyond glucose lowering, and (3) glycemic targets must be individualized based on eGFR, age, and comorbidity burden.
The KDIGO 2022 Clinical Practice Guideline for Diabetes Management in CKD provides the most current framework.
KDIGO 2022 Treatment Algorithm
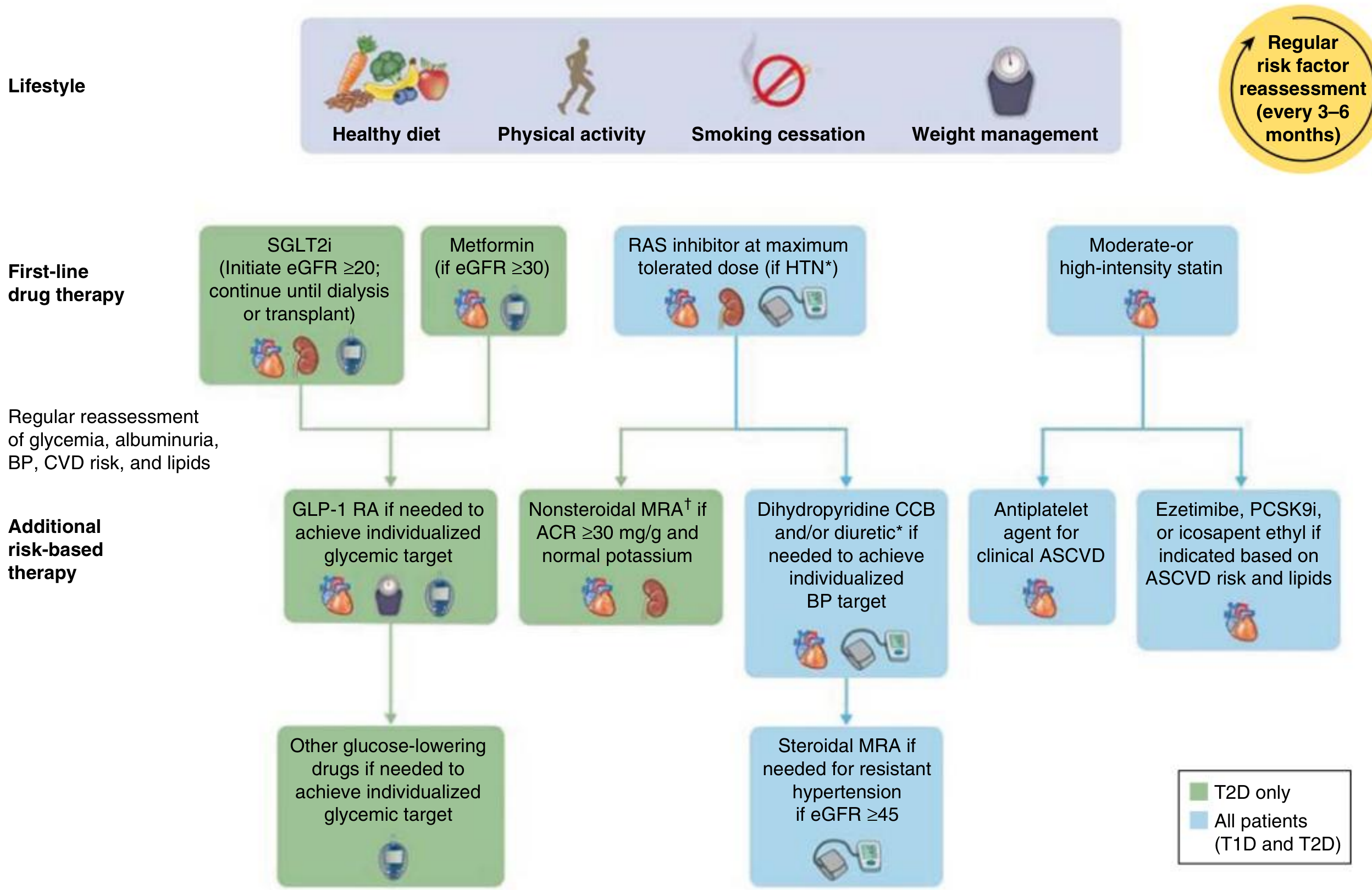
First-Line Drug Therapy (Simultaneous initiation)
1. SGLT2 Inhibitors - THE Most Important Drug in T2D + CKD
Drugs: Empagliflozin, Dapagliflozin, Canagliflozin, Ertugliflozin
Why preferred:
- The magnitude of kidney protection from SGLT2 inhibitors is ~2.5x greater than RAS inhibitors (ACE inhibitors/ARBs) when added on top of maximum RAS blockade. No other drug class has this degree of renoprotection. - Comprehensive Clinical Nephrology, 7e
- Can be initiated if eGFR ≥ 20 and continued until dialysis or transplant
- Even though glycosuric effects diminish at eGFR < 60, the BP-lowering, eGFR-preserving, and albuminuria-reducing effects are preserved at lower eGFR
Key trial evidence:
| Trial | Drug | Key Finding |
|---|---|---|
| EMPA-REG OUTCOME | Empagliflozin | 39% reduction in worsening kidney disease; 55% RRR for kidney replacement therapy |
| CREDENCE | Canagliflozin | 30% reduction in composite (ESKD + doubling creatinine + death); halted early for benefit |
| DAPA-CKD | Dapagliflozin | 39% RRR in composite kidney endpoint - in patients with AND without T2D |
| CANVAS | Canagliflozin | 40% reduction in composite kidney outcome |
Mechanisms of kidney protection:
- Tubuloglomerular feedback (TGF) activation via macula densa NaCl delivery → afferent arteriolar vasoconstriction → reduced glomerular hyperfiltration
- Albuminuria reduction 30-40%
- Reduction of intraglomerular pressure
- BP lowering (4-6 mmHg systolic)
- Weight loss and osmotic diuresis
Note: Initial acute eGFR dip of >10% occurs in ~1/3 of patients but is fully reversible and does not indicate harm.
2026 JAMA Meta-Analysis (PMID 41203232): A landmark 10-trial meta-analysis (70,361 participants) confirmed SGLT2 inhibitors reduce CKD progression risk (HR 0.62) regardless of baseline eGFR - including stage 4 CKD (eGFR < 30) - and regardless of degree of albuminuria. This supports routine use across the full spectrum of CKD.
2. Metformin - Still First-Line BUT with eGFR-Based Restrictions
Why still used:
- Low cost, weight-neutral, no hypoglycemia, CV and all-cause mortality benefit
- Preferred initial antihyperglycemic drug due to high efficacy and tolerability
eGFR-based dosing rules (KDIGO):
| eGFR (mL/min/1.73 m²) | Recommendation |
|---|---|
| ≥ 45 | Full dose - safe to use |
| 30-44 | Reduce dose to 500 mg twice daily |
| < 30 | Discontinue - risk of metformin-associated lactic acidosis (MALA) |
Why dangerous in low eGFR: Metformin is excreted unchanged by renal tubular secretion. In CKD, it accumulates → interferes with hepatic gluconeogenesis from lactate + shifts mitochondrial energy to anaerobic metabolism → lactic acidosis. Mortality of MALA is ~30%. - Comprehensive Clinical Nephrology, 7e
Second-Line (Additional Risk-Based Therapy)
3. GLP-1 Receptor Agonists
Drugs: Liraglutide, Semaglutide (subcutaneous or oral), Dulaglutide
Why preferred in CKD with CVD:
- LEADER trial (liraglutide): 22% RRR in CV death, 15% RRR in all-cause mortality, 23% reduction in kidney endpoint (mainly heavy albuminuria)
- SUSTAIN-6 and PIONEER-6 (semaglutide): Impressive CV benefits confirmed
- Both 2020 ADA and 2022 KDIGO guidelines recommend GLP-1 RAs with proven CV benefit in T2D with established CVD or high CV risk
- Weight loss benefit - important since obesity drives CKD progression
- Can be used at lower eGFR than SGLT2i (with dose adjustment)
2024 Circulation Meta-Analysis (PMID 39210781): GLP-1 RAs alone and in combination with SGLT2i show additive cardiovascular and kidney benefits in T2D - supporting combination use.
4. DPP-4 Inhibitors (Gliptins)
Drugs: Sitagliptin, Saxagliptin, Linagliptin, Alogliptin
Role in CKD:
- Well tolerated even in advanced CKD - can be used with dose adjustment
- Reduce albuminuria
- No CV outcome benefit demonstrated in trials (TECOS, SAVOR-TIMI) - they are glycemia-neutral for CV/renal protection
- Useful as add-on when SGLT2i/GLP-1 RA are contraindicated or not tolerated
Drugs to AVOID in CKD
| Drug | Reason to Avoid |
|---|---|
| Metformin (eGFR < 30) | Lactic acidosis risk |
| Sulfonylureas (e.g., glibenclamide) | Active metabolites accumulate → severe prolonged hypoglycemia |
| Thiazolidinediones (pioglitazone) | Fluid retention → worsens hypertension, heart failure, edema |
| SGLT2i (initiating at eGFR < 20) | Insufficient glycosuric efficacy; risk of euglycemic DKA |
HbA1c Targets in T2D + CKD
The KDIGO 2020 recommendation: target HbA1c 6.5-8.0%, individualized based on:
- Younger patients + early CKD + low hypoglycemia risk → tighter control (< 7%)
- Elderly + advanced CKD + frail + prior CV events → relaxed target (< 8%)
Summary Table
| Drug Class | Preferred in CKD? | eGFR Threshold | Key Benefit Beyond Glucose |
|---|---|---|---|
| SGLT2i | YES - first-line | Initiate ≥ 20; continue to dialysis | Kidney + CV + HF protection |
| Metformin | YES (with dose cut) | Reduce at < 45; stop at < 30 | Cost, weight, CV mortality |
| GLP-1 RA | YES - second-line | Mostly safe; adjust for GI issues | CV protection, weight loss |
| DPP-4i | Safe but limited | Dose-adjust; safe in advanced CKD | Glycemia only |
| Sulfonylureas | AVOID | Accumulate → hypoglycemia | None additional |
| Insulin | Use if needed | Any stage; titrate carefully | Glycemic control |
- Comprehensive Clinical Nephrology, 7th Edition, Chapter 32
This is a shared conversation. Sign in to Orris to start your own chat.