Placenta previa. Gynecology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
"placenta previa" management
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive material. Let me compose the full, well-structured answer.
Placenta Previa
Definition
Placenta previa occurs when the placenta implants over or immediately adjacent to the internal cervical os. It is one of the leading causes of antepartum hemorrhage.
- Placenta previa: placental edge covers the internal os
- Low-lying placenta: placental edge is within 2 cm of the internal os but does not cover it
Note on classification: The older categories of complete, partial, and marginal placenta previa are no longer recommended by current guidelines (NICHD terminology). The clinically relevant distinction is simply whether the placenta covers the os or lies within 2 cm of it.
Incidence
- Affects approximately 0.5% of all third-trimester pregnancies (about 1 in 200 pregnancies at term)
- Diagnosed in ~10% of midtrimester sonograms, but the vast majority resolve before delivery
- Incidence appears to be rising, likely related to increasing cesarean delivery rates
Pathogenesis
The underlying cause is unknown. The prevailing theory is that prior endometrial damage promotes implantation in the lower uterine segment, where the endometrium/decidua is less favorable. Known mechanisms include:
- Trophotropism: the placenta grows toward the better-vascularized fundus, leaving distal portions near the lower segment to regress. This explains the phenomenon of "placental migration," which is not true movement but differential atrophy
- Bleeding arises when the lower uterine segment develops and effaces, or when contractions, intercourse, or cervical examination disturb the placental-decidual interface
Risk Factors
| Risk Factor | Increased Risk |
|---|---|
| Previous placenta previa | 8× |
| Previous cesarean section | 1.5-15× |
| Age >35 years | ~4.7× |
| Age >40 years | ~9× |
| Previous suction curettage for abortion | 1.3× |
| Multiparity | 1.1-1.7× |
| Asian race | 1.9× |
| Cigarette smoking | 1.4-3.3× |
| Cocaine use | Increased |
| Assisted reproductive technology | Increased |
A single prior cesarean delivery increases the risk to ~5% in subsequent pregnancies; this rises further with multiple prior cesarean sections. - Creasy & Resnik's Maternal-Fetal Medicine, p. 1017
Clinical Features
Classic presentation: Painless, bright-red vaginal bleeding in the third trimester (after 20 weeks)
- Bleeding is typically unprovoked, though it may be triggered by intercourse, examination, or labor
- Several small "herald bleeds" often precede major hemorrhage
- In up to 10% of cases there is no bleeding until the onset of labor
- Abnormal fetal lie (transverse or oblique) is more common because the placenta prevents normal fetal polarity
Differential diagnosis of third-trimester bleeding: placental abruption, vasa previa, uterine rupture, cervical/vaginal causes
Imaging & Diagnosis
Transvaginal ultrasound (TVUS) is the gold standard for diagnosing placenta previa.
- Transabdominal US tends to overdiagnose low-lying placenta (especially with empty bladder) and is inferior for definitive localization
- TVUS is safe - multiple studies have confirmed no increased risk of hemorrhage from careful TVUS; the probe is observed on-screen during insertion to avoid a dilated cervix
- Translabial imaging with the abdominal probe is a useful alternative if TVUS is unavailable
Reporting criteria (NICHD):
- Placental edge >20 mm from internal os → report as "normal"
- Placental edge ≤20 mm but not covering the os → report as "low-lying"
- Placental edge covering the os → report as "placenta previa"
Ultrasound images:
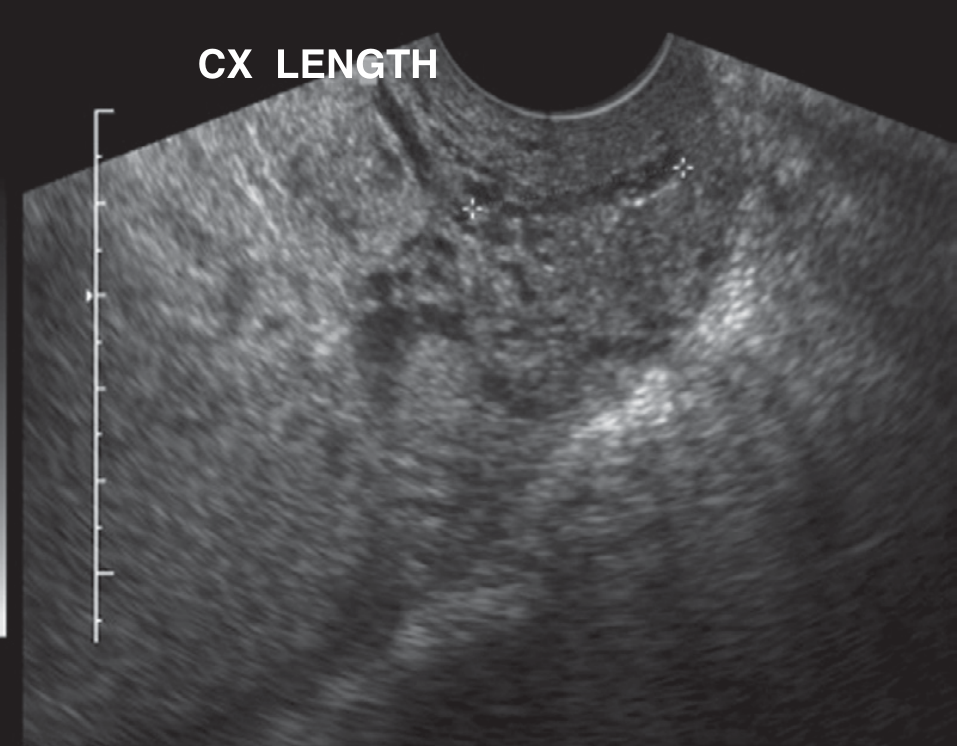
Suspected placenta previa at 17 weeks - abdominal scan showing placenta centrally located over the probable cervical location (note: details of os relationship are not visualized on transabdominal imaging):
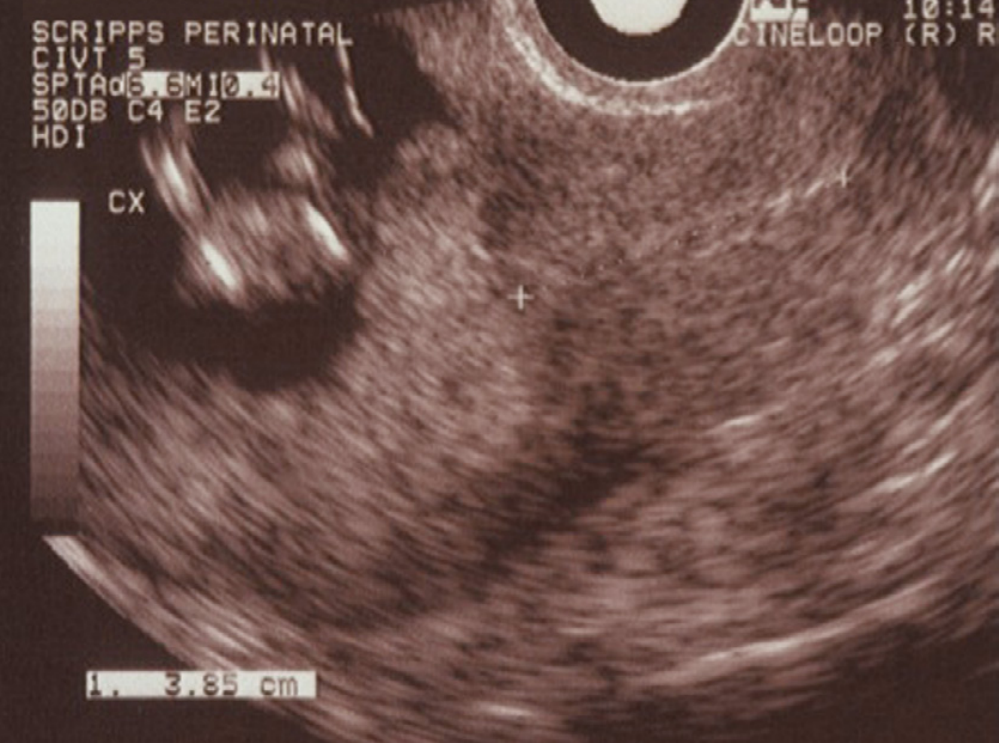
Central placenta previa on transvaginal ultrasound - clearly shows placenta overlying the endocervical os:
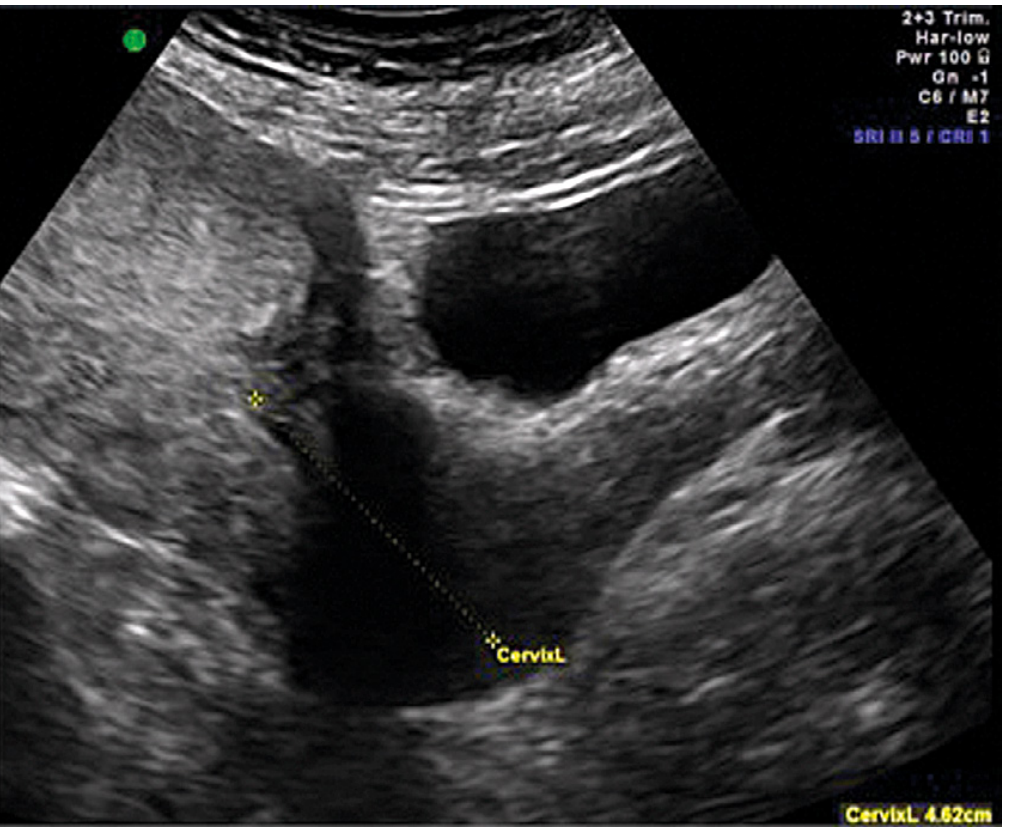
Partial placenta previa at 22 weeks - endovaginal scan showing posterior placenta extending past the endocervical os by 1.5 cm:
Placental Migration
At least 90% of placentas identified as low-lying or previa in early pregnancy resolve by the third trimester. Resolution rates by gestational age at diagnosis:
| Gestational Age at Diagnosis | Approximate % Resolved by Delivery |
|---|---|
| 15-19 weeks | ~95% |
| 20-23 weeks | ~80% |
| 24-27 weeks | ~50% |
| 28-31 weeks | ~40% |
| 32-35 weeks | ~25% |
Follow-up scanning in the early third trimester is recommended for planning. - Creasy & Resnik's Maternal-Fetal Medicine, p. 1018
Associated Complications
- Placenta accreta spectrum (accreta/increta/percreta): the most serious associated complication; the risk increases markedly when placenta previa overlies a prior uterine scar
- Vasa previa: umbilical vessels coursing in the membranes over the os; risk of catastrophic fetal exsanguination with membrane rupture
- Abnormal fetal lie
- Preterm delivery
Emergency Management (Acute Bleeding)
- Do NOT perform digital or speculum vaginal examination until placenta previa has been excluded by ultrasound - disruption of the cervical-placental junction can trigger catastrophic hemorrhage
- Establish two large-bore IVs; obtain CBC, coagulation studies, type and crossmatch
- Perform transvaginal ultrasound to confirm diagnosis
- Obstetric consultation immediately
- Fetal monitoring
- If ultrasound is unavailable and significant bleeding occurs: double-setup examination - patient taken to OR with preparations for emergency cesarean delivery, then careful vaginal exam beginning in the fornices (avoiding direct cervical entry)
Expectant (Conservative) Management
For patients who are not in active labor and bleeding is controlled:
- Hospitalization for observation and fetal monitoring
- Antenatal corticosteroids for gestational ages <37 weeks to promote fetal lung maturity
- Blood crossmatched upon admission
- Pelvic rest (no intercourse, no digital examination)
- Serial ultrasounds to monitor placental position and fetal growth
Timing and Mode of Delivery
| Situation | Delivery Timing |
|---|---|
| Uncomplicated placenta previa | 36-37 weeks by cesarean |
| Suspected placenta accreta | 34-35 weeks by cesarean, after maternal corticosteroids |
- Cesarean delivery is mandatory for all true placenta previas
- Confirm persistence of previa by TVUS within 1-2 weeks before planned delivery
- Amniocentesis for lung maturity is not recommended - it imposes unnecessary delay
- Delivery should be conducted at a center with NICU capabilities appropriate for gestational age
- If placenta accreta is present: multidisciplinary team, planned cesarean-hysterectomy via fundal incision (avoiding the placenta), with ample transfusion capability
Prognosis
- Maternal: guarded due to risk of torrential hemorrhage before and during delivery; placenta accreta is the most common indication for emergency peripartum hysterectomy
- Neonatal: morbidity and mortality more than doubled compared to uncomplicated pregnancies, largely due to iatrogenic preterm delivery; outcomes depend on gestational age at delivery and whether antenatal corticosteroids were given
- Higher reported rates of fetal anomalies, neurodevelopmental delay, and sudden infant death syndrome have been observed in some studies, though reasons remain unclear
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, pp. 1017-1022 | Tintinalli's Emergency Medicine: A Comprehensive Study | Rosen's Emergency Medicine | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.