ATLS (ABCDE)
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a comprehensive overview of the ATLS Primary Survey — ABCDE, drawn from Miller's Anesthesia and Mulholland & Greenfield's Surgery.
ATLS Primary Survey: ABCDE
The primary survey is the structured, sequential assessment of the trauma patient designed to identify and treat immediately life-threatening problems in order of priority. It must be repeated whenever the patient's condition changes.
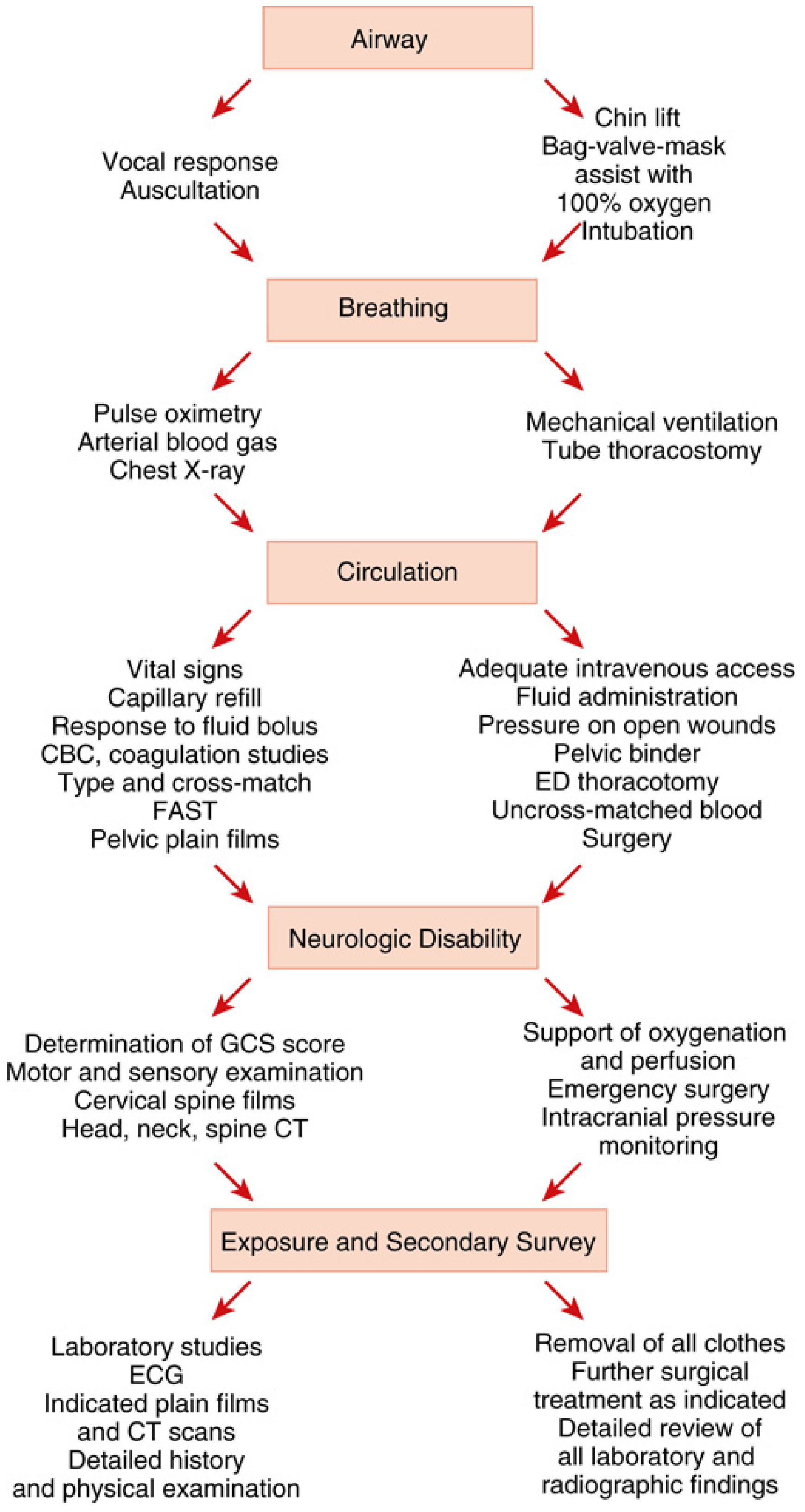
A — Airway (with C-spine protection)
Rationale: Hypoxia is the most immediate threat to life — permanent brain injury and death occur within 5–10 minutes of hypoxic arrest.
Assessment:
- Vocal response (talking = patent airway)
- Auscultation
- Look for obstruction: blood, secretions, foreign bodies, facial/mandibular/neck trauma, altered consciousness
Causes of obstruction in trauma:
- Direct injury to face, mandible, or neck
- Hemorrhage in nasopharynx, sinuses, or mouth
- Diminished consciousness (TBI, intoxication, analgesia)
- Aspiration of gastric contents, blood, or foreign body (dentures, broken teeth)
- Esophageal intubation
Interventions (escalating):
- Chin lift / jaw thrust
- Suction + oral/nasal airway
- Bag-valve-mask with 100% O₂
- Endotracheal intubation (confirm with capnography immediately — esophageal intubation is common and devastating)
- Surgical cricothyroidotomy if all else fails — this takes absolute priority over all other procedures
C-spine immobilization is maintained throughout unless injury has been excluded.
B — Breathing & Ventilation
Rationale: A patent airway does not guarantee adequate ventilation. Oxygenation AND CO₂ clearance must be assessed.
Assessment:
- Pulse oximetry
- Arterial blood gas
- Chest X-ray
- Inspect: respiratory rate, symmetry of chest rise, tracheal deviation, crepitus, subcutaneous emphysema
Causes of inadequate ventilation in trauma:
- Tension pneumothorax
- Open pneumothorax
- Hemothorax
- Flail chest / pulmonary contusion
- Direct tracheobronchial injury
- Cervical spine injury (phrenic nerve)
- Bronchospasm (smoke / toxic gas inhalation)
Interventions:
- Supplemental O₂ for all trauma patients
- Mechanical ventilation if needed
- Needle decompression + tube thoracostomy for pneumo/hemothorax
- Seal open chest wounds (three-sided dressing)
C — Circulation & Hemorrhage Control
Rationale: Hemorrhage is the #1 cause of preventable death in the first 6 hours after trauma. Shock is presumed hemorrhagic until proven otherwise.
Assessment:
- Vital signs: HR, BP, pulse pressure (narrowed = early shock)
- Capillary refill
- Skin: pallor, diaphoresis
- Response to fluid bolus
- Labs: CBC, coagulation studies, type & crossmatch
- FAST (Focused Assessment with Sonography in Trauma)
- Pelvic plain films
Symptoms of shock: Pallor · Diaphoresis · Agitation or obtundation · Hypotension · Tachycardia · Prolonged capillary refill · Diminished urine output · Narrowed pulse pressure
The 5 sites of exsanguinating hemorrhage:
| Site | Detection |
|---|---|
| Pleural space | CXR, auscultation |
| Intra-abdominal | FAST, DPA |
| Pelvis / retroperitoneal | Pelvic XR |
| Long bone fractures / soft tissue | Clinical exam |
| External | Direct visualization |
Interventions:
- Large-bore IV access × 2 (or IO/central if needed)
- Uncrossmatched blood (O-negative) if in extremis
- Activate Massive Transfusion Protocol (MTP) early — target 1:1:1 ratio (pRBC:FFP:platelets)
- Direct pressure on wounds
- Tourniquet for extremity hemorrhage
- Pelvic binder for open-book pelvic fractures
- REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) at trauma centers
- ED thoracotomy if indicated
- Emergent OR for hemorrhage control
Avoid the lethal triad: Hypothermia + Acidosis + Coagulopathy (Trauma-Associated Coagulopathy, TAC)
D — Disability (Neurological Status)
Rationale: Rapid, reproducible assessment of CNS function to detect TBI or spinal injury early — delays in evacuating epidural/subdural hematomas worsen outcomes.
Assessment:
- GCS (Glasgow Coma Scale) — Eye (1–4) + Verbal (1–5) + Motor (1–6) = 3–15
- Pupil size, reactivity, and symmetry
- Sensation and motor function in all four extremities
- Pressure stimuli: fingertip pressure, trapezius pinch, or supraorbital notch pressure
| GCS | Interpretation |
|---|---|
| 13–15 | Mild TBI |
| 9–12 | Moderate TBI |
| ≤ 8 | Severe TBI — intubate |
Abnormal motor responses:
- Abnormal flexion (decorticate): Slow stereotyped arm across chest, forearm rotating, thumb clenched, leg extended
- Normal flexion: Rapid, variable, arm moves away from body
Interventions:
- Any significant neurological deficit → immediate head CT
- Support oxygenation and perfusion (secondary brain injury prevention)
- Cervical spine films / CT
- Neurosurgery for operative lesions (epidural/subdural hematoma)
- ICP monitoring if indicated
E — Exposure & Environment
Rationale: Complete examination requires full exposure; hypothermia must be actively prevented (it worsens coagulopathy and outcomes).
Assessment:
- Completely undress the patient (cut off clothing)
- Full log-roll to examine the back
- Look for: wounds, deformities, bruising, burns, signs of penetrating injury
Interventions:
- Warm blankets and IV fluids to prevent hypothermia
- Laboratory studies
- ECG
- Plain films and CT as indicated
- Detailed history (AMPLE: Allergies, Medications, Past medical history, Last meal, Events/mechanism)
After the Primary Survey: Secondary Survey
The secondary survey — a head-to-toe examination — only begins once:
- The primary survey is complete
- Resuscitation is underway
- Vital functions are improving
The ABCDE survey must be reassessed continuously throughout care. Any deterioration restarts the sequence from A.
Sources: Miller's Anesthesia 10e, Ch. 62; Mulholland & Greenfield's Surgery 7e, Ch. 4
Fracture basics
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a comprehensive overview of Fracture Basics, drawn from Rosen's Emergency Medicine, Miller's Review of Orthopaedics, Rockwood & Green's Fractures in Adults, and Junqueira's Basic Histology.
Fracture Basics
A fracture is a break in the continuity of bone. History of trauma, pain, tenderness, swelling, loss of function, abnormal motion, and deformity all suggest a fracture.
1. Fracture Description Framework
Every fracture should be described systematically:
| Category | Descriptors |
|---|---|
| Skin integrity | Open vs. closed |
| Anatomic location | Bone, side (L/R), region (proximal/middle/distal third) |
| Fracture line direction | Transverse, oblique, spiral, comminuted |
| Completeness | Complete (both cortices) vs. incomplete (one cortex) |
| Position | Displacement, angulation, rotation, shortening |
| Articular involvement | Intra- vs. extra-articular (% of surface) |
| Special types | Avulsion, impaction, depression, compression, stress, pathologic |
By convention, the distal fragment is described relative to the proximal fragment.
2. Fracture Line Types
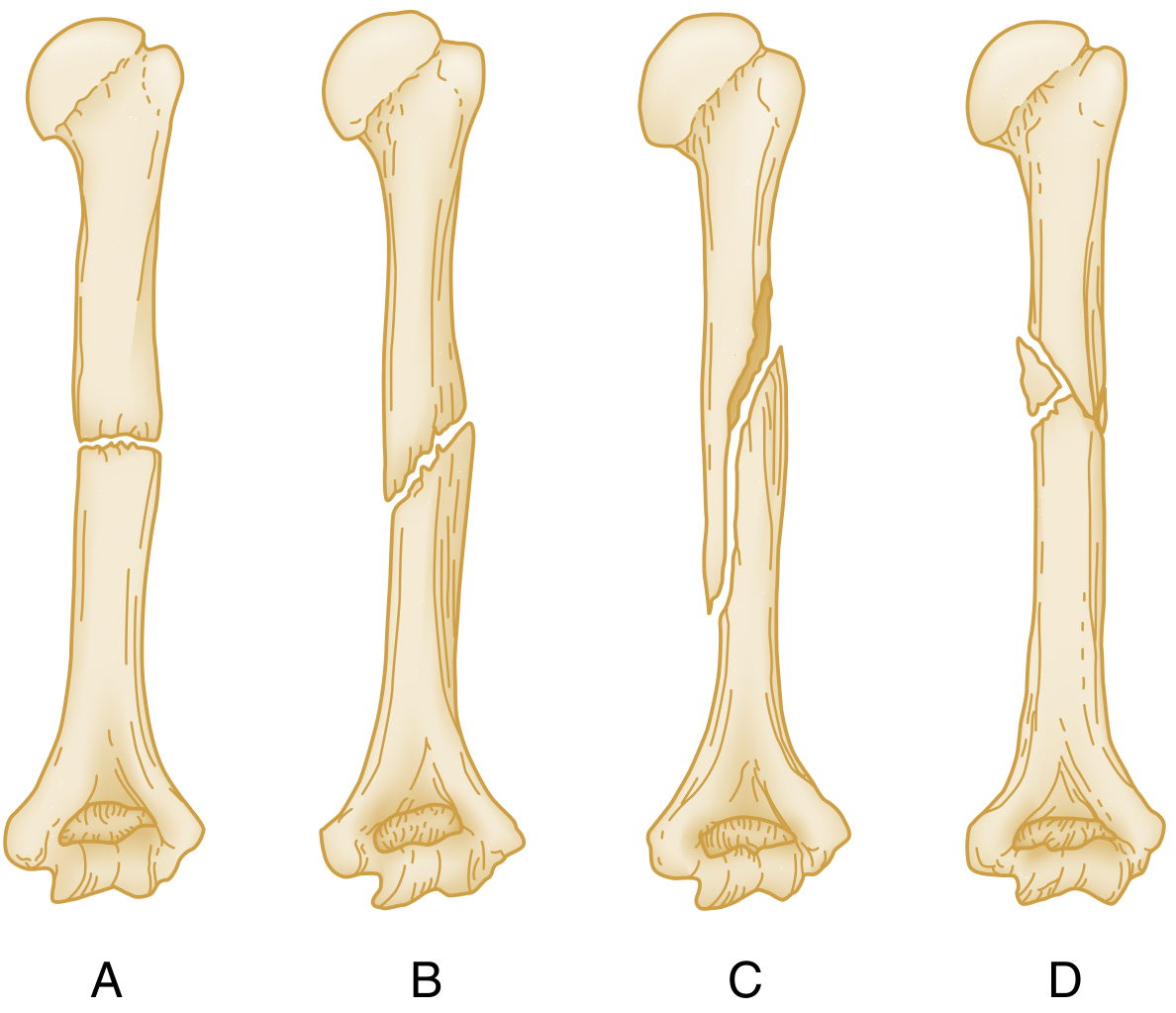
| Type | Mechanism | Notes |
|---|---|---|
| Transverse | Direct/bending force | Perpendicular to long axis |
| Oblique | Angulation force | Runs obliquely along shaft |
| Spiral | Rotational/torque force | Encircles shaft; may suggest non-accidental injury in children |
| Comminuted | High-energy | >2 fragments |
| Segmental | High-energy | Two separate fracture levels; isolates a segment |
| Avulsion | Muscle/ligament pull | Fragment torn at tendon/ligament insertion |
| Stress | Repetitive loading on normal bone | |
| Insufficiency | Normal load on weakened bone | Osteoporosis, radiation, metabolic disease |
| Pathologic | Minimal trauma through diseased bone | Tumour, Paget's, infection |
3. Open vs. Closed
- Closed: Skin and soft tissue overlying fracture are intact
- Open (compound): Fracture communicates with external environment — may not be immediately obvious
- If a wound is near the fracture and doubt exists, treat as open
- Do NOT probe with blunt swabs to determine communication — unreliable and potentially harmful
- Open fractures require urgent surgical debridement and IV antibiotics
4. Displacement & Angulation
- Displacement: Fragments deviate from their normal position (described in mm or % bone width)
- Angulation: Deviation of the long axis; described by the direction the apex points
- Valgus: Apex toward midline
- Varus: Apex away from midline
- Rotation: Distal fragment rotated along the bone axis — may only be apparent clinically (e.g., finger scissoring on flexion)
- Shortening: Overlap or impaction of fragments
5. Fracture Healing
Phases of Secondary Bone Healing
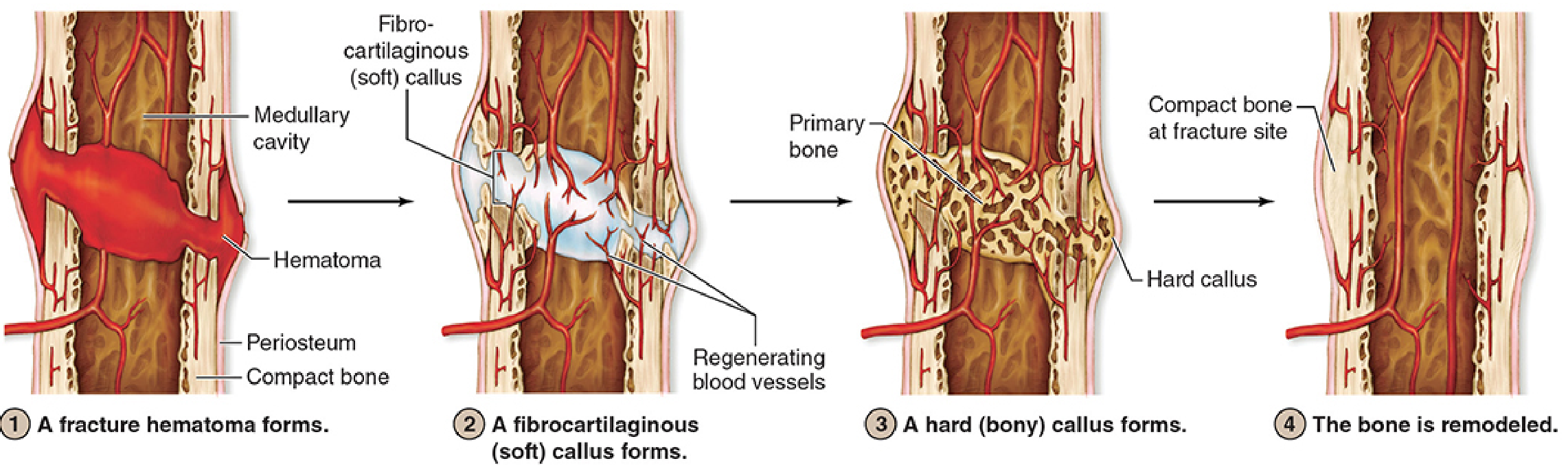
| Stage | What Happens |
|---|---|
| 1. Inflammation / Hematoma | Torn blood vessels bleed → fracture hematoma forms; macrophages phagocytose debris; cytokines (IL-1β, IL-6, TNF-α) recruit progenitor cells |
| 2. Soft (fibrocartilaginous) callus | Periosteum and endosteum proliferate; MSCs differentiate; fibrocartilage procallus bridges the gap; regenerating blood vessels invade |
| 3. Hard (bony) callus | Fibrocartilage undergoes endochondral ossification → woven bone callus |
| 4. Remodeling | Woven bone replaced by lamellar bone; Wolff's law dictates structure along stress lines; original shape and strength restored |
Primary vs. Secondary Healing
| Primary (Direct) | Secondary (Indirect) | |
|---|---|---|
| Condition | Absolute stability, no gap | Relative stability, some movement |
| Mechanism | Haversian remodeling (cutting cones) | Callus formation (endochondral + intramembranous ossification) |
| Fixation | Compression plate | Casting, IM nail, external fixator |
| Callus | None visible on X-ray | Visible periosteal callus |
Key Factors Affecting Healing
- Pro-healing: Good vascularity, periosteum intact, stable fixation, BMPs (BMP-2, BMP-7)
- Impair healing: NSAIDs (inhibit COX-2, impair endochondral ossification), smoking, corticosteroids, infection, diabetes, poor nutrition
- Bone grafts:
- Osteoconductive — scaffold (e.g., demineralized bone matrix)
- Osteoinductive — stimulate bone formation (e.g., BMP)
- Osteogenic — contain living bone-forming cells (e.g., autograft)
6. Complications
Early
| Complication | Key Points |
|---|---|
| Vascular injury | Check distal pulses; ABI if concerned |
| Nerve injury | Specific nerves at risk per fracture (e.g., radial nerve in humeral shaft fractures, median nerve in distal radius fractures) |
| Compartment syndrome | Pain out of proportion + tense compartment; tibia most common; emergency fasciotomy if pressure >30 mmHg or within 30 mmHg of diastolic |
| Fat embolism | Long bone / pelvic fractures; triad: hypoxia + confusion + petechiae |
| Infection | Especially open fractures |
Late
| Complication | Key Points |
|---|---|
| Malunion | Healed in poor position |
| Nonunion | Failure to heal by 6 months; hypertrophic (vascular, needs more stability) vs. atrophic (avascular, needs biology) |
| Delayed union | Healing slower than expected |
| Avascular necrosis | Disrupted blood supply; common: femoral head, scaphoid, talus |
| Post-traumatic arthritis | Intra-articular fractures |
| Refracture | Especially after hardware removal |
7. Principles of Fracture Management
The goals are: Reduce → Hold → Rehabilitate
| Principle | Options |
|---|---|
| Reduction | Closed (manipulation) or open (surgical) |
| Immobilization | Cast/splint · External fixator · IM nail · Plate & screws |
| Rehabilitation | Early mobilisation to prevent stiffness and muscle atrophy |
Rule: If in doubt about fracture stability or open communication — immobilise, image in two planes (orthogonal views), and get orthopaedic input.
Sources: Rosen's Emergency Medicine, Ch. 41; Miller's Review of Orthopaedics 9e; Rockwood & Green's Fractures in Adults 10e; Junqueira's Basic Histology 17e
Shoulder dislocation
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Shoulder Dislocation, drawn from Rockwood & Green's Fractures in Adults, Roberts & Hedges' Clinical Procedures in Emergency Medicine, Schwartz's Principles of Surgery, and the THIEME Atlas of Anatomy.
Shoulder Dislocation
Anatomy & Why the Shoulder Dislocates So Easily
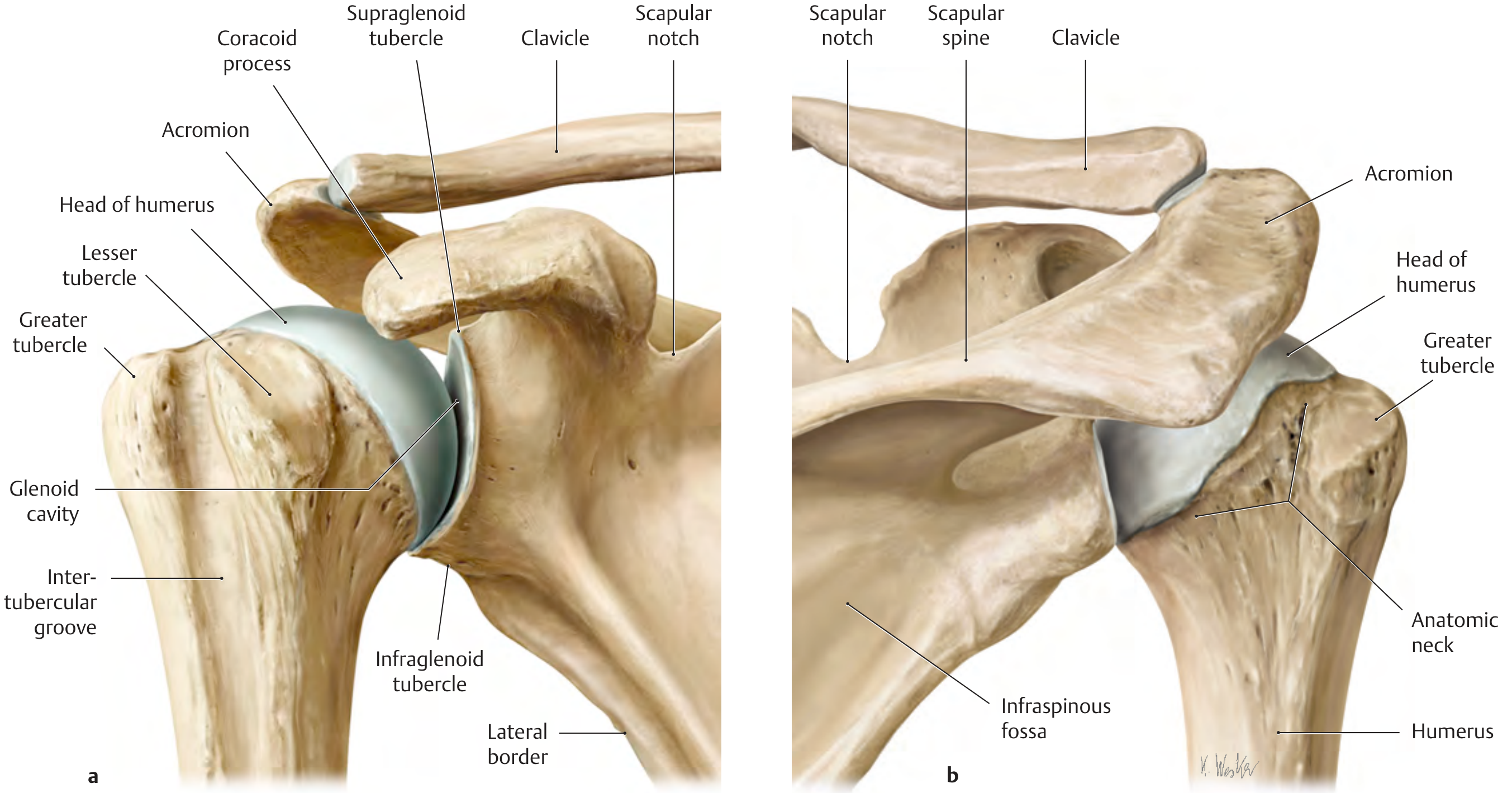
The glenohumeral joint is the most mobile joint in the body — and consequently the most commonly dislocated (~45% of all dislocations). The glenoid cavity is 3–4× smaller than the humeral head; the glenoid labrum deepens it by only ~5 mm. The joint capsule and ligaments are inherently weak, making the rotator cuff the primary dynamic stabilizer.
Types of Dislocation
| Direction | Frequency | Mechanism | Arm Position |
|---|---|---|---|
| Anterior (anteroinferior) | ~95% | Forced external rotation + abduction (FOOSH, throwing, seizure) | Slight abduction, external rotation |
| Posterior | ~2–4% | Forced internal rotation (seizure, electrocution, direct blow) | Internal rotation + adduction ("sling position") |
| Inferior (Luxatio Erecta) | Rare | Hyperabduction force | Arm locked overhead in hyperabduction |
Anterior Dislocation
Clinical Features
- Posterior sulcus visible (loss of normal rounded contour)
- Arm held in slight abduction and external rotation
- Inability to place palm of affected hand on contralateral shoulder
- Palpable fullness anteriorly (humeral head)
Imaging
- AP view — humeral head not in glenoid fossa
- Axillary (glenoid) view — gold standard; confirms direction
- Y-view (scapular lateral) — useful when axillary view not tolerated
Associated Injuries
| Injury | Details |
|---|---|
| Bankart lesion | Tear of anteroinferior glenoid labrum ± avulsion of glenoid rim (bony Bankart) — the essential lesion of shoulder instability |
| Hill-Sachs lesion | Impaction fracture of posterior humeral head against glenoid rim — seen in 33% of primary and 62% of recurrent dislocations |
| Axillary nerve injury | 13.5% incidence; test sensation over deltoid (regimental badge area); 90% recover with expectant management |
| Axillary artery injury | Check capillary refill and radial pulse; more common in elderly |
| Rotator cuff tear | Up to 38% incidence; much higher in patients >40 years |
| Greater tuberosity fracture | If displaced >1 cm post-reduction → rotator cuff tear likely → orthopaedic consult |
| HAGL lesion | Humeral Avulsion of GlenoHumeral Ligaments |
Posterior Dislocation
Clinical Features (Easily Missed!)
- Arm in internal rotation + adduction ("sling position")
- Loss of external rotation and forward flexion
- No obvious deformity — diagnosis commonly delayed
- Causes: seizures, electrocution, direct posterior blow
Imaging
- Often missed on AP view alone — the humeral head may appear falsely normal
- Axillary view is mandatory — shows posterior displacement
- Trough sign on AP — dense sclerotic line on humeral head (reverse Hill-Sachs impaction)
- Fracture of the lesser tuberosity = posterior dislocation until proven otherwise
Associated Injuries
- Reverse Bankart fracture (posterior glenoid rim)
- Reverse Hill-Sachs lesion (anterior humeral head)
- Posterior capsule and labrum tear
- 65% have an associated injury overall
Inferior Dislocation — Luxatio Erecta
- Arm locked in marked hyperabduction with forearm lying on or behind the head
- Associated with neurovascular injury (brachial plexus, axillary vessels) and rotator cuff tears
- Reduction: Overhead traction in abduction with cephalad pressure on the humeral head; assistant applies countertraction caudally via sheet over the shoulder
Reduction Techniques (Anterior Dislocation)
Premedication (procedural sedation or intra-articular lidocaine block) improves muscle relaxation and success.
| Technique | Method | Notes |
|---|---|---|
| External Rotation | Arm adducted, elbow flexed 90°; slowly externally rotate forearm to bed level. No traction. | Low force; high patient tolerance; good for first-line attempt |
| Stimson | Patient prone, arm hanging off stretcher; 5 kg weight attached; 20–30 min. Add scapular manipulation. | Low force; requires patient cooperation |
| Scapular Manipulation | Rotate inferior tip of scapula medially and dorsally while assistant provides traction | Can combine with Stimson; patient prone or seated |
| Spaso Technique | Supine; lift arm vertically toward ceiling + gentle vertical traction + gentle ER; 87.5% success rate | Fast, single-operator; equivalent efficacy to external rotation |
| Milch Technique | Abduct arm overhead, apply gentle traction + slight ER; push humeral head into glenoid if needed | |
| Traction-Countertraction | Two sheets — one around axilla (assistant countertraction), one around forearm (operator traction); gentle adduction while second assistant applies lateral traction | Classic technique; requires 2 assistants |
| Best-of-Both | Patient seated sideways; downward force on flexed forearm + scapular manipulation simultaneously | Combines two effective methods |
Signs of successful reduction:
- Audible/palpable "clunk"
- Immediate pain relief
- Restoration of round shoulder contour
- Patient can place palm of affected hand on contralateral shoulder
Post-reduction: Repeat neurovascular exam + post-reduction radiographs. Immobilise with sling/shoulder immobiliser pending orthopaedic follow-up.
Posterior Dislocation Reduction
- Traction on internally rotated and adducted arm + anteriorly directed pressure on posterior humeral head
- Generous premedication + countertraction via axillary sheet
- If head locked on posterior glenoid → add lateral traction on upper humerus
- Impression defect >20% of articular surface → open reduction required
- Post-reduction: Check patient can place palm on opposite shoulder; orthopedic consultation for all posterior dislocations
Post-Reduction Management
| Factor | Recommendation |
|---|---|
| Immobilisation | Sling/shoulder immobiliser; prolonged immobilisation does not reduce recurrence rates (>1 week not beneficial per meta-analysis) |
| Position of immobilisation | Some evidence favours external rotation (maximises labral contact with glenoid rim vs. internal rotation which increases labral detachment) |
| Age <40 | Higher recurrence risk (up to 70–90% in teenagers); consider early orthopaedic referral for discussion of surgical stabilisation |
| Age >60 | Early mobilisation to prevent stiffness and adhesive capsulitis; follow up at 5–7 days |
| Imaging | MRI to assess soft tissue (labrum, rotator cuff, capsule) |
Recurrent Instability & Surgery
- Arthroscopic Bankart repair — gold standard for most cases (anteroinferior capsulolabral complex)
- Latarjet procedure — coracoid transfer to anterior glenoid rim; for large bony glenoid defects (>25% glenoid bone loss) or engaging Hill-Sachs lesions
- Remplissage — arthroscopic infraspinatus tenodesis into Hill-Sachs defect; reduces engagement
- Open Bankart repair — reserved for revision or complex cases
Sources: Rockwood & Green's Fractures in Adults 10e, Ch. 35; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Schwartz's Principles of Surgery 11e; THIEME Atlas of Anatomy — General Anatomy & Musculoskeletal System
Fracture of humerus
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Finding Sources
Finding Sources
Here is a comprehensive overview of Fractures of the Humerus, covering proximal, shaft, and distal segments, drawn from Rockwood & Green's, Schwartz's Principles of Surgery, and Miller's Review of Orthopaedics.
Fractures of the Humerus
The humerus is divided into three regions for clinical purposes: proximal, shaft (diaphyseal), and distal. Each has a distinct epidemiology, classification, nerve injury risk, and management.
1. Proximal Humerus Fractures
Epidemiology
- Most common in elderly women after low-energy falls onto the shoulder
- Also occur in young patients after high-energy trauma
- Account for ~5% of all fractures; 3rd most common fragility fracture after hip and distal radius
Anatomy — The Neer 4-Part System

Neer's classification divides the proximal humerus into 4 parts:
- Humeral head (articular segment)
- Greater tuberosity (supraspinatus, infraspinatus, teres minor insertions)
- Lesser tuberosity (subscapularis insertion)
- Humeral shaft
A part is considered "displaced" when separated by >1 cm or >45° angulation.
| Neer Classification | Description | Frequency |
|---|---|---|
| 1-part | Any fracture, no segment displaced | ~80% |
| 2-part | One segment displaced | Common |
| 3-part | Two segments displaced | Less common |
| 4-part | All four segments separated | Rare; high AVN risk |
Despite wide use, inter-observer reliability of the Neer system is moderate. CT is recommended for complex patterns.
Blood Supply & AVN Risk
- The humeral head blood supply comes predominantly via the anterior humeral circumflex artery (arcuate artery) and posterior circumflex artery
- 4-part fractures and fracture-dislocations carry >30% risk of avascular necrosis (AVN) of the humeral head
Treatment
| Fracture Type | Management |
|---|---|
| Minimally displaced (1-part) | Sling immobilisation; pendulum exercises by 2 weeks; physio within 2 weeks to prevent stiffness |
| 2-part greater tuberosity | If displaced >5 mm → ORIF (especially in overhead athletes); if <5 mm → conservative |
| 2-part surgical neck | Closed reduction + sling, or ORIF if unstable |
| 3-part | ORIF with locking plate ± tension band |
| 4-part / head-splitting / fracture-dislocation | Hemiarthroplasty or reverse total shoulder arthroplasty (RTSA) (favoured in elderly with osteoporosis); ORIF in young patients with good bone stock |
| Elderly + osteoporosis + comminuted | RTSA gaining popularity |
Post-op: Early pendulum exercises → passive ROM → active ROM → strengthening
2. Humeral Shaft (Diaphyseal) Fractures
Mechanisms
- Direct blow, fall, high-energy trauma
- Torsional force (spiral fracture pattern)
- Pathologic fracture (metastasis is common here)
Key Nerve at Risk: Radial Nerve
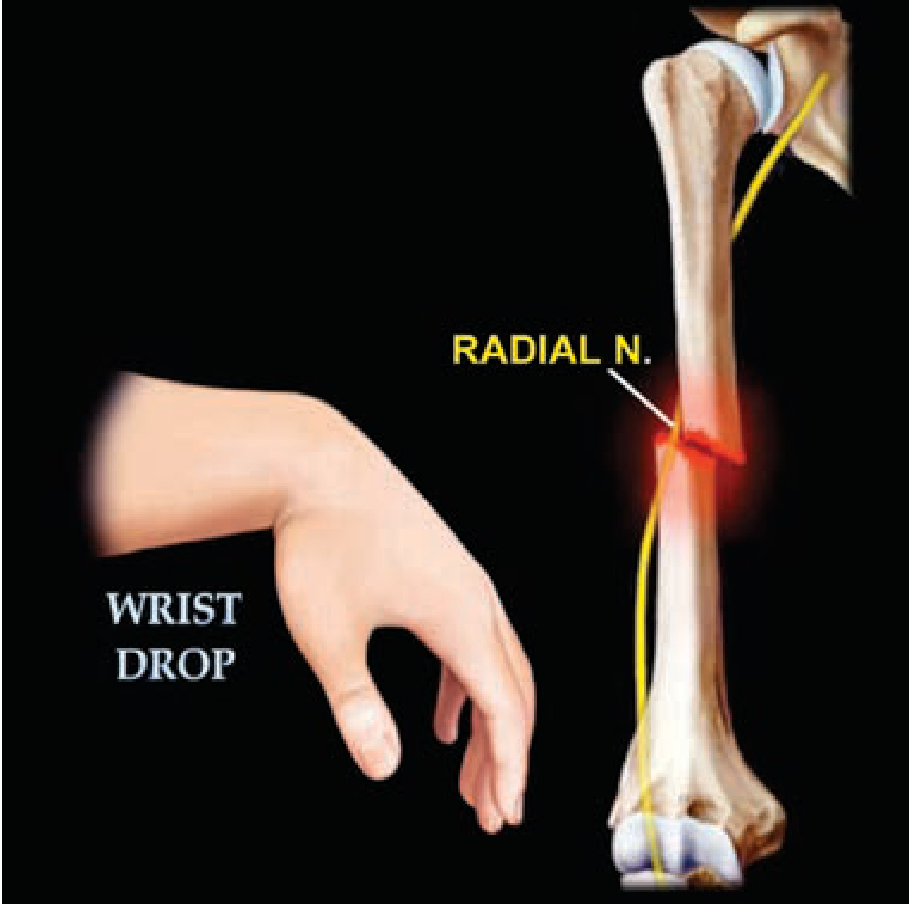
- The radial nerve runs in the spiral (radial) groove on the posterior surface of the humerus
- Incidence of radial nerve palsy: ~11–18% of all humeral shaft fractures
- Holstein-Lewis fracture: Spiral fracture of the distal third of the shaft — highest risk of radial nerve entrapment/injury
- The vast majority of radial nerve palsies are neuropraxias (stretch/contusion) → spontaneous recovery expected within 3–4 months
- EMG at 6–8 weeks helps assess recovery; if no recovery by 3–4 months → surgical exploration
Acceptable Alignment for Non-Operative Treatment
| Parameter | Acceptable Limit |
|---|---|
| Anterior angulation | < 20° |
| Varus/valgus angulation | < 30° |
| Shortening | < 3 cm |
Radial nerve palsy is NOT a contraindication to conservative management (except in open fractures, where nerve must be explored)
Treatment
| Scenario | Management |
|---|---|
| Most closed fractures | Coaptation splint initially → functional brace (plastic clamshell with Velcro) within 1–2 weeks; gentle motion started within 1–2 weeks |
| Unacceptable angulation | ORIF with plate (more stable, allows early weight-bearing) |
| Intramedullary nail | Alternative; risk of shoulder pain at nail entry site |
| Open fracture + radial nerve palsy | Surgical exploration of nerve mandatory |
| Radial nerve palsy (closed fracture) | Expectant management; EMG to monitor; explore if no recovery by 3–4 months |
3. Distal Humerus Fractures
Types
| Type | Description |
|---|---|
| Supracondylar | Above the elbow joint; does not involve articular surface — most common in adults after a fall |
| Transcondylar | Through both condyles |
| Intercondylar (bicondylar) | Intra-articular "T" or "Y" pattern; most complex |
| Single condyle (lateral/medial) | Lateral = Milch classification; can cause cubitus valgus + tardy ulnar nerve palsy |
| Capitellum / trochlea | Coronal shear fractures |
| Epicondyle | Avulsion fractures |
Nerve Injuries at the Distal Humerus
| Fracture | Nerve at Risk |
|---|---|
| Supracondylar (extension type, children) | Anterior interosseous nerve (branch of median) — unable to make "OK sign" |
| Supracondylar | Radial nerve, median nerve |
| Medial epicondyle | Ulnar nerve |
| Lateral condyle malunion → cubitus valgus | Tardy ulnar nerve palsy |
Vascular Injury
- Supracondylar fractures can injure or tether the brachial artery
- Check: radial pulse, capillary refill, and "pink pulseless hand" (pulseless but perfused via collaterals) vs. true ischaemia
Treatment
| Fracture | Management |
|---|---|
| Minimally displaced supracondylar | Posterior long arm splint at 90° elbow flexion |
| Displaced / most distal humerus | ORIF with anatomically contoured dual plates (orthogonal or parallel plating); goal = anatomic articular reduction + early ROM |
| Severely comminuted (elderly) | Total elbow arthroplasty (TEA) |
| Intra-articular fractures | Anatomic reduction of joint surface is paramount; early motion to prevent stiffness |
Elbow fractures are notorious for stiffness — early range of motion is critical to a good outcome.
Summary Table
| Region | Key Nerve Risk | Key Classification | Primary Non-Op Rx | Primary Op Rx |
|---|---|---|---|---|
| Proximal | Axillary nerve | Neer (4-part) | Sling + early pendulums | ORIF locking plate / RTSA |
| Shaft | Radial nerve (spiral groove) | AO/OTA | Functional brace | Plate fixation / IM nail |
| Distal | AIN / ulnar / radial | AO/OTA | Posterior splint (min. displaced) | Dual plate ORIF / TEA |
Sources: Schwartz's Principles of Surgery 11e, Ch. 43; Rockwood & Green's Fractures in Adults 10e; Miller's Review of Orthopaedics 9e
Hip fracture
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Here is a comprehensive overview of Hip Fractures, drawn from Rockwood & Green's Fractures in Adults, Mulholland & Greenfield's Surgery, Grainger & Allison's Diagnostic Radiology, and Morgan & Mikhail's Clinical Anesthesiology.
Hip Fracture
Epidemiology & Public Health Impact
Hip fractures are a major public health crisis:
- Bimodal distribution: rare high-energy fractures in the young; overwhelmingly common fragility fractures in the elderly (mean age ~80 years, female:male ~3:1)
- 15–20% mortality within 3 months; 20–25% mortality at 1 year for trochanteric fractures
- 30–50% lose a degree of functional independence
- ~4.5 million fractures/year worldwide projected by 2050 (up from 1.3 million in 1990)
- Strongly associated with osteoporosis, falls, sarcopenia, polypharmacy, and frailty
Classification by Anatomical Location
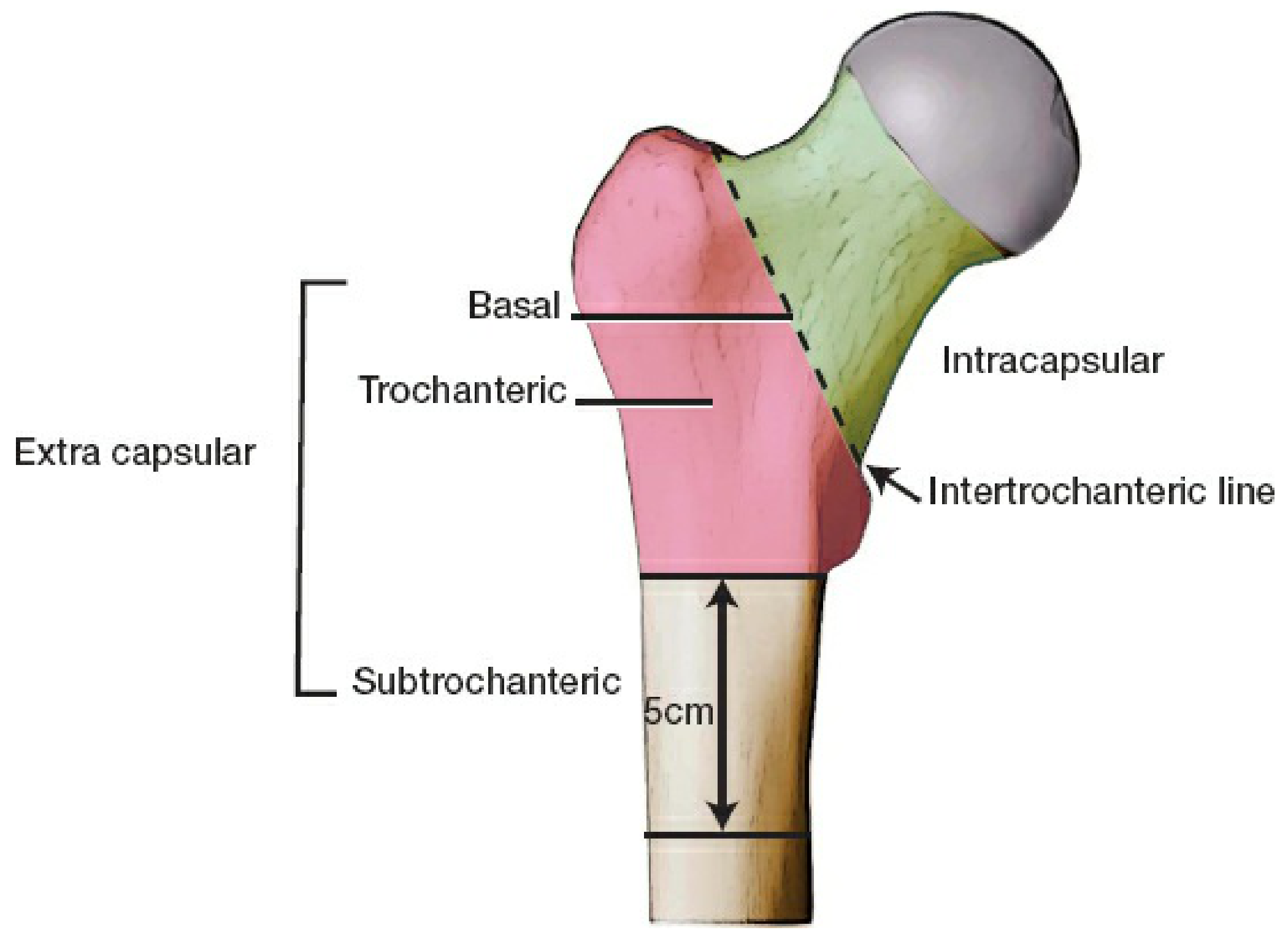
The critical division is intracapsular vs. extracapsular — this determines the risk of avascular necrosis (AVN) and dictates surgical strategy.
| Type | Location | AVN Risk | Key Issue |
|---|---|---|---|
| Intracapsular (femoral neck) | Subcapital, transcervical, basicervical | High (15–35% displaced) | Blood supply to femoral head at risk |
| Extracapsular — Trochanteric | Inter-trochanteric region | Low | Mechanical instability, varus collapse |
| Extracapsular — Subtrochanteric | ≤5 cm distal to lesser trochanter | Low | High bending forces; challenging fixation |
1. Intracapsular (Femoral Neck) Fractures
Blood Supply
The femoral head receives blood from retinacular vessels (branches of the medial and lateral circumflex femoral arteries) that run along the femoral neck. Displacement tears these vessels → AVN of the femoral head in 15–35% of displaced fractures.
Garden Classification
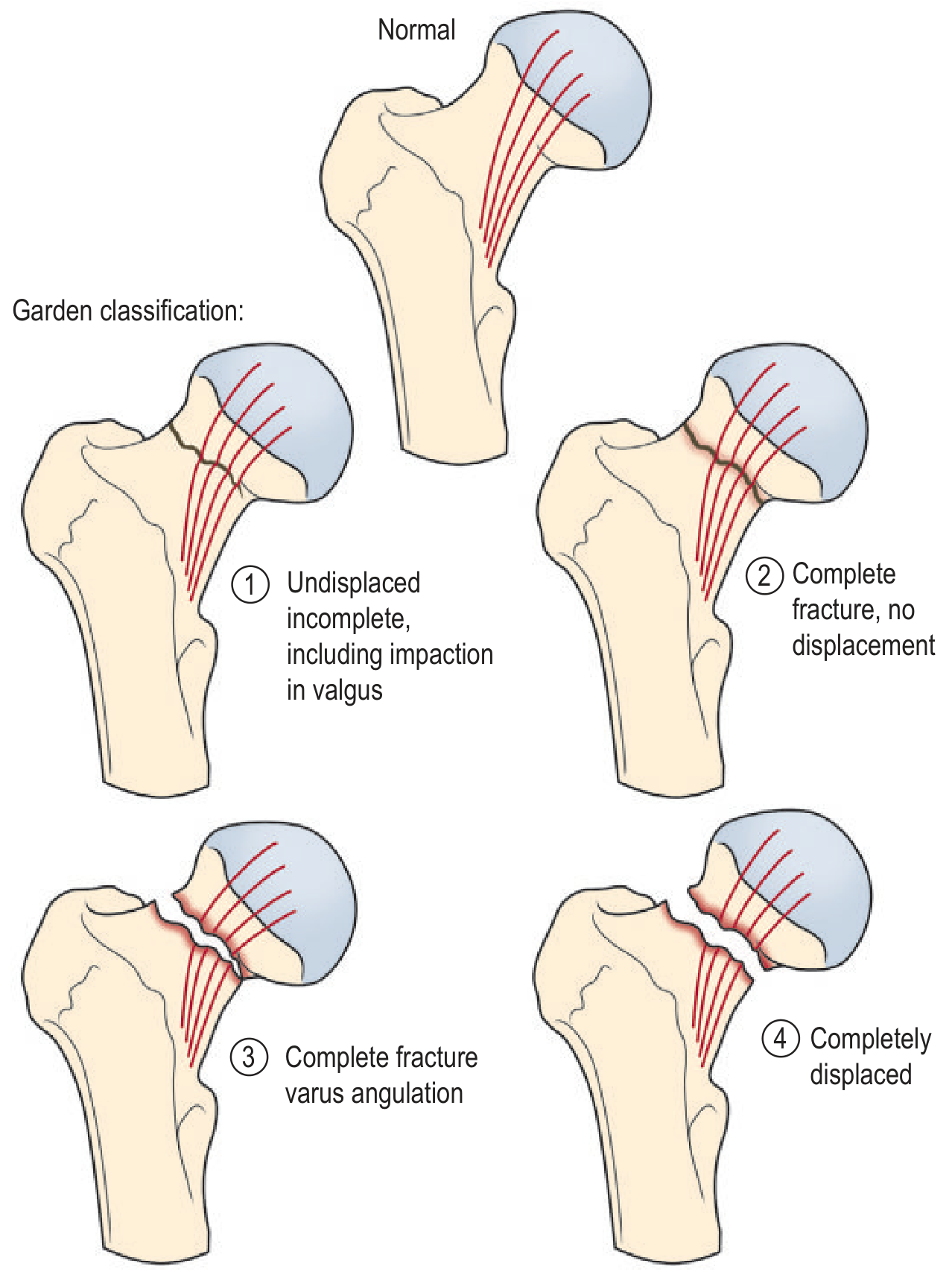
| Garden Grade | Description | AVN Risk |
|---|---|---|
| I | Undisplaced incomplete (impacted in valgus) | Low |
| II | Complete, no displacement | Low |
| III | Complete, varus angulation | High |
| IV | Completely displaced | High |
Clinically simplified as: Undisplaced (I + II) vs. Displaced (III + IV)
Treatment
| Patient Group | Fracture | Treatment |
|---|---|---|
| Young patient (<60 yrs) | Undisplaced (Garden I/II) | Internal fixation — multiple cannulated screws or dynamic hip screw (DHS); preserve the femoral head |
| Young patient | Displaced (Garden III/IV) | Urgent ORIF (emergency to restore blood supply); if irreducible → hemiarthroplasty |
| Elderly, independently mobile | Any displacement | Total Hip Arthroplasty (THA) — better functional outcomes than hemiarthroplasty in active patients |
| Elderly, low demand / frail | Displaced | Hemiarthroplasty (cemented preferred for stability and pain) |
| Poor bone stock | Undisplaced | Hemiarthroplasty/THA rather than fixation |
Key principle: Displaced intracapsular fractures in the elderly are generally best treated with arthroplasty rather than fixation (high failure and revision rate with fixation due to AVN and non-union).
2. Extracapsular — Trochanteric Fractures
These fractures have a good blood supply but are mechanically unstable — they collapse into varus without surgical fixation.
OTA/AO Classification
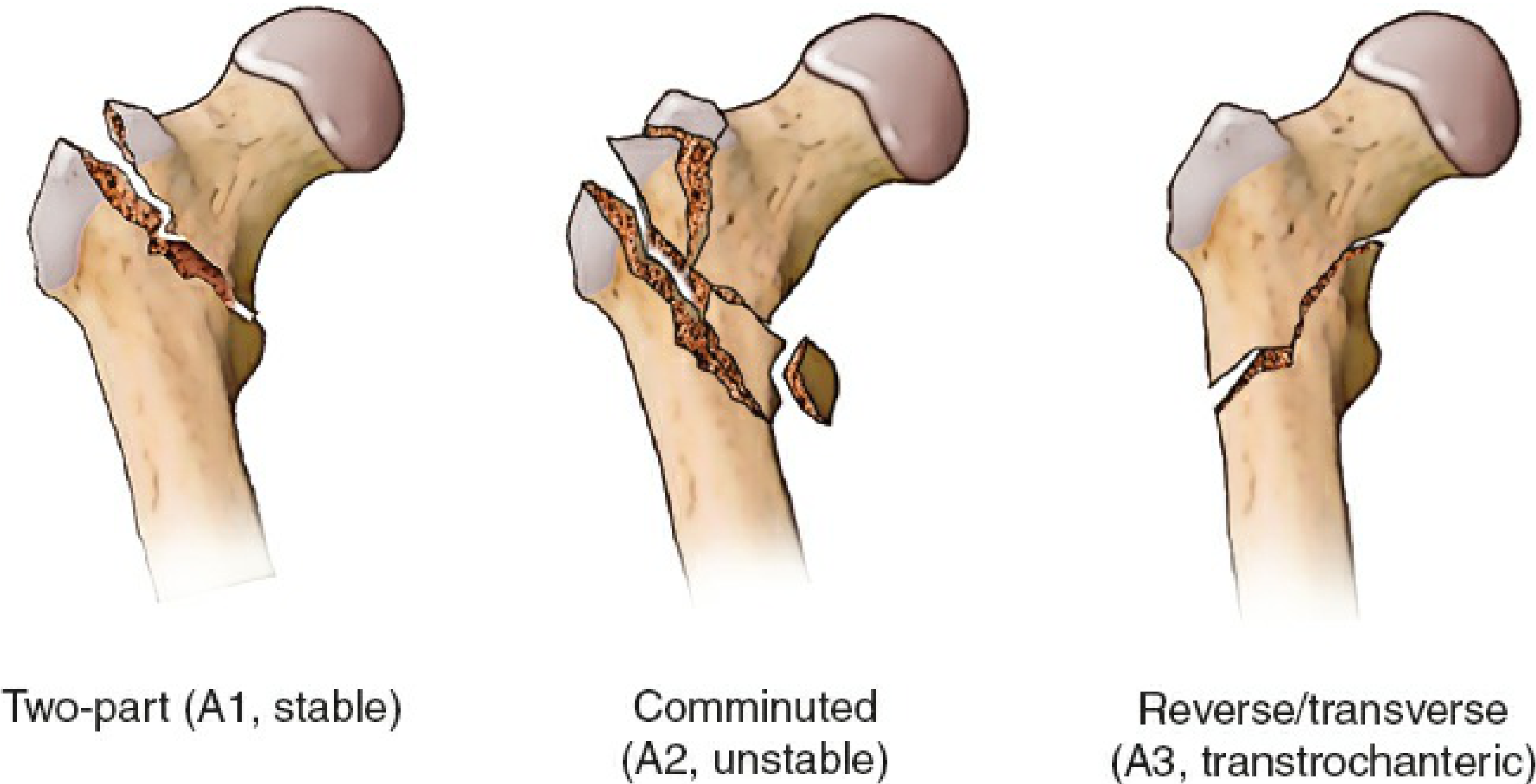
| AO Type | Pattern | Stability | Lateral Wall |
|---|---|---|---|
| 31.A1 | Two-part; fracture through trochanters | Stable | Intact |
| 31.A2 | Comminuted; lesser trochanter detached; ≥3 main fragments | Unstable | Intact but compromised |
| 31.A3 | Reverse oblique or transverse; fracture line extends laterally | Very unstable | Incompetent |
Treatment
| Pattern | Device |
|---|---|
| A1 / A2 (intact lateral wall) | Sliding Hip Screw (Dynamic Hip Screw, DHS) + side plate; allows controlled collapse and impaction |
| A3 / reverse obliquity / subtrochanteric extension / compromised lateral wall | Intramedullary nail (cephalomedullary nail, e.g., PFNA, Gamma nail) — controls rotation, resists bending, allows weight-bearing |
Key point for DHS: Screw tip must be close to the articular surface (tip-apex distance <25 mm) to prevent cut-out.
3. Subtrochanteric Fractures
- Region of highest mechanical stress in the skeleton (bending + compressive forces)
- Occur at medial calcar — area of cortical stress concentration
- Associated with bisphosphonate therapy (atypical subtrochanteric fractures with prodromal thigh pain and a "banana" lateral bow on plain X-ray)
- Treatment: Intramedullary nail (long, to the knee, to avoid stress risers)
Clinical Presentation
| Feature | Finding |
|---|---|
| History | Fall from standing height (elderly); high-energy in young |
| Pain | Groin, hip, inner thigh; referred to knee |
| Limb position | Shortened + externally rotated (displaced); neutral position (undisplaced) |
| Inability to weight-bear | Typical, but undisplaced fractures may still walk |
| Tenderness | Over greater trochanter or groin |
~15% of hip fractures are occult on plain X-ray — use MRI (gold standard) or CT if high clinical suspicion with normal X-ray.
Perioperative Management
Timing of Surgery
- Target: within 24–48 hours of admission (once medically optimised)
- Delay >48 hours associated with higher mortality, increased pressure sores, DVT, pneumonia
- Brief delay acceptable for reversing anticoagulation or optimising significant cardiorespiratory comorbidity
Anaesthesia
- Spinal vs. general: No significant difference in 60-day mortality or delirium in large prospective studies; slightly shorter hospital stay with regional anaesthesia
- Regional analgesia: Fascia iliaca block or 3-in-1 femoral nerve block — effective pre- and post-operative pain control; avoids respiratory depression of intrathecal opioids
Perioperative Considerations
- Thromboprophylaxis: LMWH or direct oral anticoagulants post-op; mechanical prophylaxis (TED stockings, pneumatic compression) pre-op
- Delirium prevention: Avoid anticholinergics, benzodiazepines; early mobilisation; adequate analgesia; sleep hygiene
- Orthogeriatric co-management: Geriatrician involvement from admission reduces mortality and complications
- Bone health: Osteoporosis treatment (bisphosphonates, denosumab) must be initiated prior to discharge — a hip fracture is a sentinel event for future fractures
Falls Risk Factors to Address
- Polypharmacy review (antihypertensives, tranquillisers, alcohol)
- Visual correction
- Balance and strength physiotherapy
- Home hazard assessment
Complications
| Complication | Notes |
|---|---|
| AVN of femoral head | Intracapsular fractures; 15–35% of displaced; may present months–years later |
| Non-union | More common with displaced intracapsular fractures treated with fixation |
| Fixation failure / screw cut-out | DHS: tip-apex distance >25 mm; osteoporosis |
| DVT / PE | High risk; mandatory prophylaxis |
| Pneumonia | From immobility; early mobilisation is protective |
| Delirium | Very common post-op in elderly hip fracture patients |
| Pressure sores | From prolonged bed rest |
| Mortality | ~20–25% at 1 year |
Summary Decision Framework
Hip Fracture
│
├── Intracapsular (femoral neck)
│ ├── Undisplaced (Garden I/II)
│ │ ├── Young → Internal fixation (cannulated screws)
│ │ └── Elderly / poor bone → Hemiarthroplasty
│ └── Displaced (Garden III/IV)
│ ├── Young → Urgent ORIF (or hemi if irreducible)
│ ├── Active elderly → THA
│ └── Frail elderly → Hemiarthroplasty (cemented)
│
└── Extracapsular
├── Trochanteric (A1/A2, intact lateral wall) → DHS
├── Trochanteric (A3 / reverse oblique) → IM nail
└── Subtrochanteric → Long IM nail
Sources: Rockwood & Green's Fractures in Adults 10e, Ch. 54; Mulholland & Greenfield's Surgery 7e, Ch. 28; Grainger & Allison's Diagnostic Radiology; Morgan & Mikhail's Clinical Anesthesiology 7e, Ch. 38
Femur fracture
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Here is a comprehensive overview of Femur Fractures, covering the shaft and distal femur in detail, drawn from Rockwood & Green's Fractures in Adults 10e.
Femur Fractures
The femur is the largest, strongest bone in the body. Fracturing it requires substantial force — making it a marker of high-energy trauma and a cause of significant haemorrhage, systemic injury, and mortality.
Overview: Regions of the Femur
| Region | Covered In |
|---|---|
| Proximal femur (femoral neck, trochanteric, subtrochanteric) | ← See Hip Fracture topic |
| Femoral shaft (diaphysis) | This section |
| Distal femur (supracondylar/condylar) | This section |
Part 1: Femoral Shaft (Diaphyseal) Fractures
Epidemiology & Mechanism
Femoral shaft fractures show a bimodal distribution:
- Young males (15–25 years): High-energy trauma — MVA, motorcycle accidents, falls from height, pedestrian injuries, gunshot wounds
- Elderly females (>75 years): Low-energy falls on osteoporotic bone
- Atypical femur fractures (50–70 years): Bisphosphonate-associated; transverse subtrochanteric or midshaft fractures with prodromal thigh pain and lateral cortical thickening ("beaking")
Fracture patterns by force:
- Bending force → transverse ± butterfly fragment
- Rotational force → spiral or oblique
- Axial force → associated hip/knee injuries
- Higher energy → comminution ↑
Haemorrhage
The femoral shaft lies within the thigh musculature — closed femoral shaft fractures can result in 1.0–1.5 L of blood loss into the thigh. In multiply injured patients, this is a major contributor to haemorrhagic shock. Stabilise early.
Associated Injuries
In a review of 26,357 femur fractures:
- Lung injury: 18.9%
- Intracranial injury: 13.5%
- Liver: 6.2%
- Tibia/fibula fractures: 20.5%
- Ribs/sternum: 19.1%
- Ipsilateral femoral neck fracture: 5.8% — missed in 20–50% of cases initially
Always image the full femur, including the hip and knee. Protocol: internal rotation AP hip view + fine-cut CT of the hip (2 mm axial/sagittal) + post-op radiographs → 91% reduction in missed femoral neck fractures.
Classification — Winquist & Hansen (Comminution)
| Grade | Comminution | Cortical Contact |
|---|---|---|
| 0 | None | 100% |
| I | Small butterfly <25% | ≥75% |
| II | Butterfly ~25–50% | ≥50% |
| III | Butterfly ~50–75% | Minimal |
| IV | Complete; no cortical contact | None (segmental) |
Higher grade = requires statically locked nail to prevent shortening and rotation.
Treatment
Timing: Stabilise the femur within 24 hours in multiply-injured patients → reduces pulmonary complications (Bone et al.).
1. Temporary Stabilisation
| Method | Use |
|---|---|
| Hare traction splint (skin traction) | Prehospital / field — restore length, reduce pain |
| Skeletal traction (distal femur or proximal tibia pin) | In-hospital bridge to definitive surgery in polytrauma or haemodynamically unstable patients |
| External fixation | Damage control orthopaedics — polytrauma, open fracture with contamination, vascular injury needing repair, medullary contamination |
Skeletal traction pin placement:
- Distal femur pin: placed medial → lateral (avoids femoral artery at adductor hiatus)
- Proximal tibia pin: placed lateral → medial (avoids peroneal nerve)
- Weight: ~15% of body weight (15–20 lb)
2. Definitive Fixation
Intramedullary Nailing (IMN) — gold standard for most femoral shaft fractures
| Parameter | Detail |
|---|---|
| Entry point | Antegrade (piriformis fossa or greater trochanter tip) or Retrograde (via knee, intercondylar notch) |
| Reamed vs. unreamed | Reamed preferred — improves union rates; reaming does not increase mortality in trauma patients |
| Locking | Static locking (proximal + distal interlocking screws) — controls length and rotation in comminuted fractures |
| Weight bearing | Immediate weight-bearing allowed after static locking even in comminuted fractures |
Indications for IMN:
- Most closed and open femoral shaft fractures
- Segmental and comminuted fractures
- Multiple trauma (within 24 hours when stable)
Relative contraindications to IMN:
- Canal too narrow (unable to ream)
- Pre-existing implant filling the canal (e.g., THA)
- Associated ipsilateral femoral neck fracture (use separate fixation)
- Open growth plates (piriformis entry avoided; trochanteric entry used)
- Severe polytrauma with chest/head injury → temporary external fixation first
Plate Fixation (less common for shaft):
- Used when IMN is contraindicated or in certain fracture patterns
- Open approach (lateral): extensive dissection → higher blood loss, infection risk
- MIPO (minimally invasive plate osteosynthesis): smaller incisions, preserves blood supply, but higher risk of malreduction
- Plate is not load-bearing → immediate weight-bearing carries implant failure risk
Part 2: Distal Femur (Supracondylar/Condylar) Fractures
Definition
The distal 15 cm of the femur, from the condyles to the junction of metaphysis and diaphysis.
Epidemiology
- Bimodal: Young (high-energy) and elderly (fragility fracture)
- Elderly distal femur fracture = analogous to hip fracture in terms of morbidity; 5-year mortality >50%
- Often complicates total knee arthroplasty (periprosthetic fracture)
OTA/AO Classification
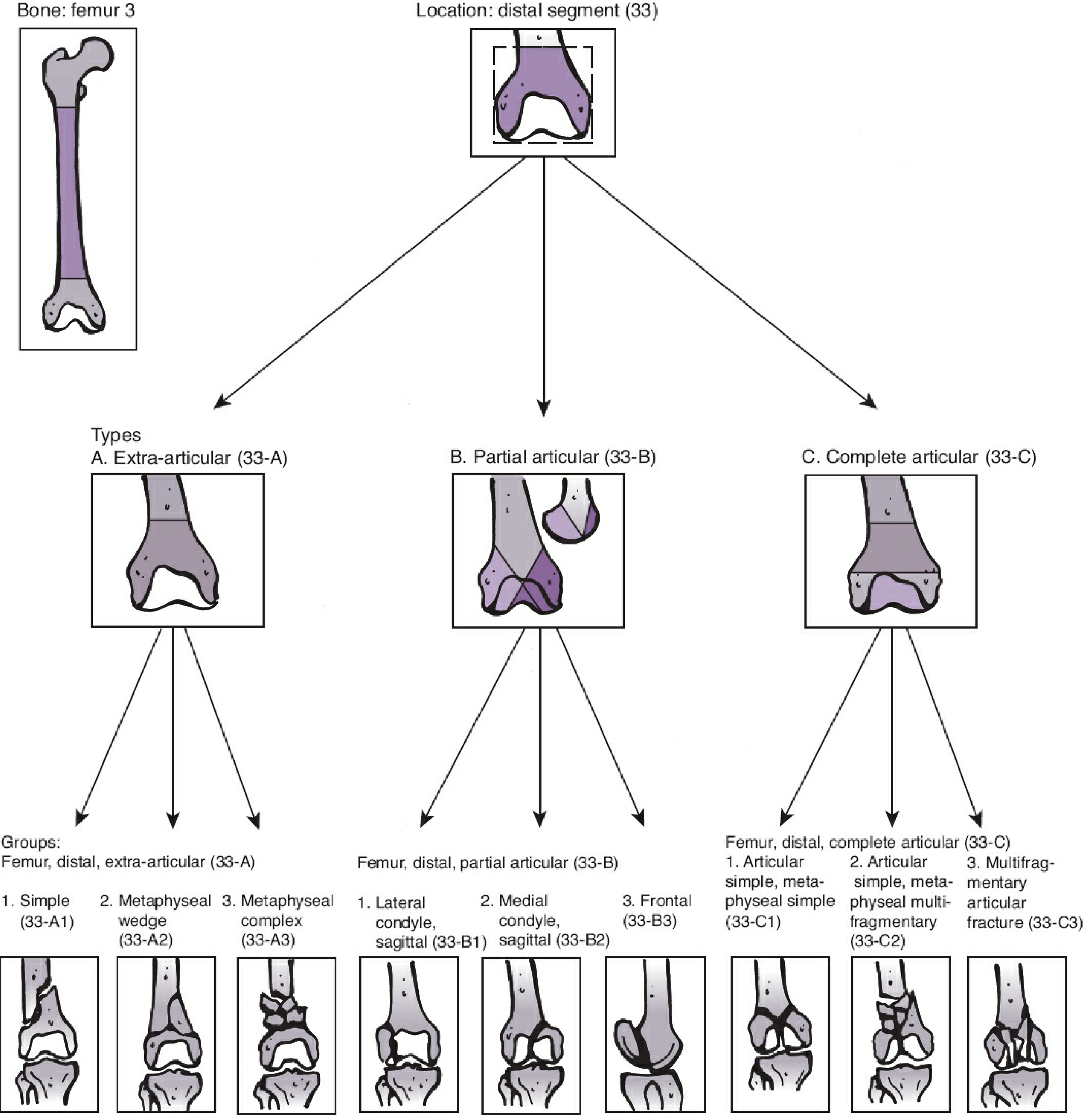
| Type | Description |
|---|---|
| 33-A (Extra-articular) | Supracondylar; joint surface not involved |
| 33-B (Partial articular) | One condyle involved; rest of shaft in continuity |
| 33-C (Complete articular) | Bicondylar; complete separation from shaft ("T" or "Y" fracture) |
Each type is subdivided 1–3 by increasing comminution.
Hoffa fracture: Coronal plane fracture through a single condyle — found in 40% of intercondylar fractures; frequently missed on plain X-ray — CT mandatory.
Key Anatomy
- Distal femur is trapezoidal on end — implants placed anteriorly on AP view may protrude posteriorly and cause pain
- Popliteal artery lies posterior to the distal femur — at risk in displaced fractures
- Peroneal and tibial nerves in the popliteal fossa — check neurovascular status
Deforming Force
The gastrocnemius pulls the distal fragment into hyperflexion/posterior angulation — this must be corrected at reduction (knee flexion during surgery reduces this deformity).
Treatment
| Fracture | Management |
|---|---|
| Minimally displaced extra-articular | Posterior long-arm splint with knee at 90° → early motion |
| Most displaced / articular fractures | ORIF — lateral locking plate (± medial plate for very comminuted cases); goal = anatomic articular reduction + stable fixation + early ROM |
| Retrograde IM nail | Good for extra-articular and some partial articular fractures; also useful in periprosthetic fractures above TKA |
| Periprosthetic above TKA | Retrograde nail if adequate distal space; locked plating if not |
| Severely comminuted, elderly | Total Knee Arthroplasty (TKA) or distal femur replacement (megaprosthesis) |
Intra-articular fractures: Anatomic reduction of the joint surface is paramount — tolerances <2 mm step-off — to reduce risk of post-traumatic arthritis.
Stiffness is the most common complication of distal femur fractures — early range of motion is critical.
Complications Summary
| Complication | Notes |
|---|---|
| Haemorrhagic shock | 1–1.5 L blood loss in closed shaft fracture |
| Fat embolism syndrome | Especially with bilateral or high-energy femur fractures; triad: hypoxia + petechiae + confusion |
| Missed ipsilateral neck fracture | Up to 50% missed on initial presentation — use CT protocol |
| Malunion | Especially with non-operative treatment; leg length discrepancy, angular or rotational deformity |
| Non-union | Union rates with IMN ~97–100%; higher with plate and open fractures |
| Knee stiffness | Most common after distal femur fractures and prolonged traction |
| Post-traumatic arthritis | Intra-articular distal femur fractures |
| Infection | Open fractures; pin tract infections with external fixation (>50%) |
| Implant failure | Plates especially prone in osteoporotic bone without early mobilisation |
Sources: Rockwood & Green's Fractures in Adults 10e, Ch. 57 (Femoral Shaft), Ch. 58–59 (Distal Femur); Mulholland & Greenfield's Surgery 7e
Osteoarthritis
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Here is a comprehensive overview of Osteoarthritis, drawn from Robbins & Kumar Basic Pathology, Miller's Review of Orthopaedics, and Schwartz's Principles of Surgery.
Osteoarthritis (OA)
Also called degenerative joint disease (DJD), OA is the most common joint disease — characterised by progressive degeneration of articular cartilage, subchondral bone changes, and osteophyte formation.
OA is primarily a degenerative disorder; inflammation is a secondary contributor, not the primary driver (unlike rheumatoid arthritis).
Epidemiology & Risk Factors
| Factor | Detail |
|---|---|
| Prevalence | ~40% of people >70 years affected; exponential increase after age 50 |
| Primary (idiopathic) | ~95% of cases; appears in older adults without predisposing cause; oligoarticular |
| Secondary | ~5%; younger patients; predisposing conditions below |
Risk Factors:
- Age (most important)
- Obesity (mechanical loading + metabolic effects)
- Female sex (especially post-menopausal)
- Previous joint injury (trauma, meniscectomy, ACL tear)
- Joint deformity (varus/valgus malalignment, hip dysplasia, FAI)
- Repetitive occupational loading
- Genetic predisposition (polymorphisms in matrix components and signalling molecules)
- Systemic diseases: diabetes, haemochromatosis, acromegaly, Wilson's disease
OA vs. Rheumatoid Arthritis — Key Differences
| Feature | Osteoarthritis | Rheumatoid Arthritis |
|---|---|---|
| Primary mechanism | Mechanical injury to cartilage | Autoimmunity |
| Inflammation | Secondary; exacerbates damage | Primary driver |
| Joints affected | Weight-bearing (hips, knees); DIP/PIP/1st CMC in hand | Small joints (MCP, PIP, wrist); symmetric |
| Pathology | Cartilage degeneration, osteophytes, subchondral cysts; minimal synovitis | Inflammatory pannus, severe synovitis, joint fusion (ankylosis) |
| Serum antibodies | None | ACPA, rheumatoid factor (up to 80%) |
| Systemic involvement | No | Yes (lungs, heart, skin) |
Pathogenesis
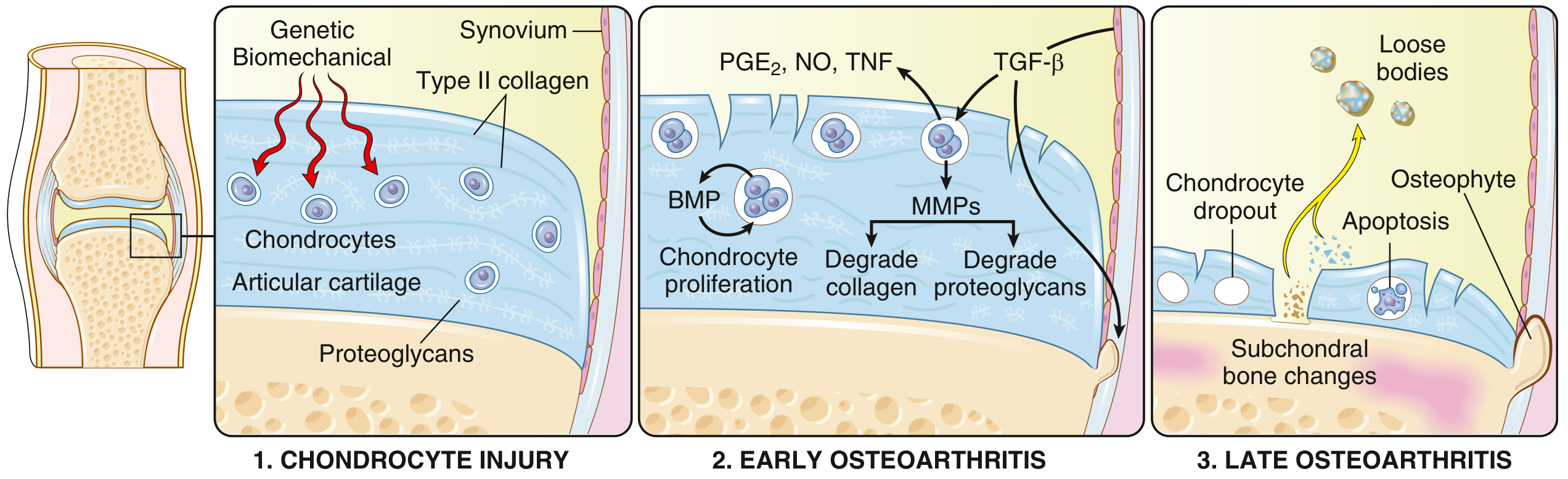
Stage 1 — Chondrocyte Injury
- Biomechanical stress + genetic predisposition → chondrocyte injury
- Type II collagen and proteoglycan matrix alterations begin
Stage 2 — Early OA
- Chondrocytes proliferate (attempt at repair) and secrete:
- MMPs (matrix metalloproteinases) → degrade type II collagen and proteoglycans
- PGE₂, NO, TNF → pro-inflammatory mediators
- TGF-β, BMP → attempted repair signals
- Degradation exceeds repair → net cartilage loss
- Water content of cartilage ↑ initially (proteoglycan loss) → softening, fibrillation
Stage 3 — Late OA
- Progressive chondrocyte apoptosis and dropout
- Loss of articular cartilage (exposed subchondral bone)
- Subchondral bone changes:
- Sclerosis (eburnation — ivory-like polished bone surface)
- Subchondral cysts (fluid forced through micro-fractures)
- Osteophyte (bone spur) formation at joint margins
- Cartilage fragments → loose bodies in joint
- Secondary synovitis from debris phagocytosis
Gross & Microscopic Pathology
| Feature | Finding |
|---|---|
| Gross | Softened, fibrillated, ulcerated cartilage; exposed eburnated bone; marginal osteophytes; subchondral cysts |
| Microscopic | Chondrocyte cloning (proliferative clusters), matrix pallor, vertical clefts (fibrillation), hypocellular zones, tidemark duplication |
| Synovium | Mild hyperplasia; scattered inflammatory cells (mononuclear); no destructive pannus |
Joints Affected
| Joint | Notes |
|---|---|
| Knee | Most commonly symptomatic; medial compartment affected first (varus deformity) |
| Hip | Superior-pole OA most common; causes groin pain |
| DIP joints (fingers) | Heberden's nodes (osteophytes at DIP) |
| PIP joints (fingers) | Bouchard's nodes |
| 1st CMC (thumb base) | Very common; "squaring" of the thumb base |
| Cervical and lumbar spine | Facet joint OA → spondylosis; osteophytes may cause radiculopathy or spinal stenosis |
| 1st MTP (great toe) | Hallux rigidus/valgus |
Clinical Features
| Feature | Description |
|---|---|
| Pain | Activity-related, worse with use, better with rest (early); constant at rest in advanced disease |
| Morning stiffness | Brief, <30 min (cf. RA where >1 hour) |
| Joint swelling | Bony (osteophytes); may have effusion |
| Crepitus | Grating/crunching on movement |
| Reduced ROM | Progressive joint restriction |
| Deformity | Varus knee (bow-legged); angular deformity as disease advances |
| No systemic features | No fever, weight loss, or extraarticular manifestations |
Investigations
Radiograph (Plain X-ray) — Cornerstone of Diagnosis
The 4 cardinal radiographic features (mnemonic: LOSS):
| Feature | Explanation |
|---|---|
| Loss of joint space | Asymmetric narrowing (medial compartment knee) |
| Osteophytes | Bone spurs at joint margins |
| Subchondral sclerosis | Increased density of bone beneath cartilage |
| Subchondral cysts | Geodes — lucent areas in subchondral bone |
X-ray correlates poorly with symptoms — many radiologically severe cases are asymptomatic, and symptomatic patients may have mild radiographic changes.
Kellgren-Lawrence Grade (knee OA):
| Grade | Findings |
|---|---|
| 0 | Normal |
| 1 | Doubtful narrowing; possible osteophyte |
| 2 | Definite osteophyte; possible narrowing |
| 3 | Moderate narrowing + multiple osteophytes |
| 4 | Severe narrowing; subchondral sclerosis; bone-on-bone |
Other investigations:
- MRI: Cartilage thickness, bone marrow oedema, meniscal pathology — useful for pre-surgical planning and diagnosing early OA
- Bloods: Normal CRP/ESR, RF, ANA — used to exclude inflammatory arthritis
- Joint aspiration: Clear, viscous fluid; WBC <2000/µL (cf. septic arthritis >50,000/µL)
Management
Non-Pharmacological (First-Line for All)
| Intervention | Evidence |
|---|---|
| Weight loss | 1 kg weight loss = 4 kg reduction in knee load; most effective intervention in obese patients |
| Exercise (aerobic + strengthening) | Reduces pain and improves function as much as NSAIDs; quadriceps strengthening key for knee OA |
| Physiotherapy | Gait training, joint protection, muscle strengthening |
| Walking aids / orthotics | Unloader braces (valgus brace for medial knee OA); wedge insoles |
| Patient education / self-management | Improves outcomes |
Pharmacological
| Drug | Notes |
|---|---|
| Paracetamol (acetaminophen) | First-line analgesic; modest effect |
| Topical NSAIDs (diclofenac gel) | Effective for knee OA; fewer GI side effects |
| Oral NSAIDs / COX-2 inhibitors | Effective for pain; use lowest dose, shortest duration; consider PPI co-prescription; caution in CVD, renal disease |
| Intra-articular corticosteroids | Short-term relief (weeks–months); good for flares or pre-rehabilitation |
| Intra-articular hyaluronic acid | Evidence mixed; some guidelines no longer recommend |
| Duloxetine | Useful for central sensitisation component; chronic knee OA |
| Opioids | Last resort; significant side effects; avoid in elderly |
| Glucosamine / chondroitin | Evidence inconclusive; no longer routinely recommended |
Surgical
| Procedure | Indication |
|---|---|
| Arthroscopic washout / debridement | No longer recommended for OA (NICE, ACR) — no benefit over sham surgery in RCTs |
| Osteotomy | High tibial osteotomy (HTO) for medial compartment knee OA in younger active patients with varus deformity; realigns mechanical axis |
| Unicompartmental knee arthroplasty (UKA) | Single-compartment disease; preserved ACL; less invasive, faster recovery |
| Total Knee Arthroplasty (TKA) | End-stage symptomatic knee OA; 10-15 year implant survival >90–95% |
| Total Hip Arthroplasty (THA) | End-stage hip OA; one of the most successful operations in medicine |
Indications for arthroplasty: Persistent pain despite adequate non-operative treatment + radiographic end-stage OA + functional limitation — not based on age alone.
Sources: Robbins & Kumar Basic Pathology; Miller's Review of Orthopaedics 9e; Schwartz's Principles of Surgery 11e
Osteomyelitis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Osteomyelitis, drawn from Robbins, Cotran & Kumar Pathologic Basis of Disease, Rosen's Emergency Medicine, and Schwartz's Principles of Surgery.
Osteomyelitis
Definition: Infection of bone and bone marrow — virtually always secondary to infection. May be a complication of systemic infection or manifest as a primary solitary focus.
Classification by Route of Infection
| Route | Context | Key Features |
|---|---|---|
| Haematogenous | Children (most common), elderly, IV drug users | Bacteraemia seeds metaphysis; usually single organism |
| Contiguous spread | Soft tissue infection, pressure ulcers, diabetic foot | Polymicrobial; spreads to adjacent bone |
| Direct inoculation | Open fractures, surgery, prosthetic joint implantation, puncture wounds | Polymicrobial; organisms from skin/environment |
Microbiology
| Setting | Organisms |
|---|---|
| All ages (most common) | S. aureus — 80–90% of culture-positive cases; binds bone matrix collagen via cell wall proteins |
| Neonates | Group B Streptococcus, E. coli |
| Children | S. aureus (MRSA most common in AHO); Kingella kingae in <5 yrs |
| Adults | S. aureus; Staphylococcus epidermidis (implant-associated) |
| Sickle cell disease | Salmonella + S. aureus (areas of osteonecrosis → nidus for seeding; impaired splenic function) |
| IV drug users | Pseudomonas aeruginosa, Candida, S. aureus |
| Diabetic foot | Polymicrobial (Gram-positive + Gram-negative + anaerobes) |
| Open fractures / post-trauma | Polymicrobial; environmental organisms |
| Immunocompromised | Mycobacterium tuberculosis, fungi |
| Note | Specific organisms identified in only ~50% of cases |
Pathogenesis & Morphology
Acute Osteomyelitis (first days–weeks)
- Bacteria proliferate → neutrophilic reaction → necrosis of bone and marrow within 48 hours
- Bacteria spread through Haversian canals → reach periosteum
- In children, periosteum loosely attached → subperiosteal abscess forms, dissects along bone
- Periosteal lifting → further impairs blood supply → extends necrosis
- Soft tissue abscess → can channel to skin as draining sinus
Chronic Osteomyelitis (weeks → years)
- Chronic inflammatory cells recruited → cytokines stimulate bone resorption + fibrous ingrowth
- Sequestrum: Dead, devascularised infected bone (fails to resorb)
- Involucrum: Shell of reactive new bone laid down around the infected/necrotic bone (periosteal new bone formation)
- Sinus tracts may fistulise to skin
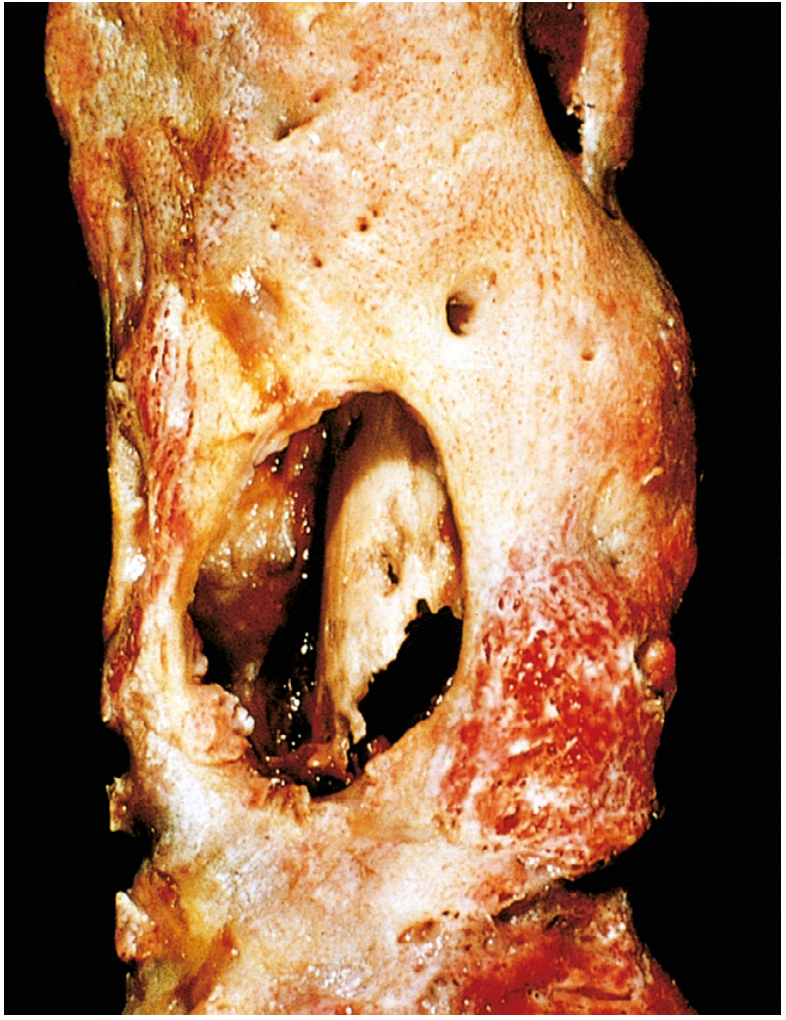
| Term | Definition |
|---|---|
| Sequestrum | Dead, separated cortical bone within infected cavity |
| Involucrum | New periosteal bone encasing the sequestrum |
| Cloaca | Openings in the involucrum through which pus drains |
| Brodie's abscess | Subacute form — localised intraosseous abscess in metaphysis, walled off by reactive bone; often in children |
Age-Specific Distribution
Children — Acute Haematogenous Osteomyelitis (AHO)
- Ages 3 months to 16 years; male:female = 2–3:1
- Long bones in ~80%: distal femoral metaphysis most common
- Metaphysis targeted due to sluggish blood flow in metaphyseal sinusoids (terminal capillaries loop, allowing bacteria to settle)
- In neonates: Metaphyseal vessels penetrate the growth plate → epiphysis and metaphysis both involved; septic arthritis frequently coexists (~50% have multifocal disease)
- In older children (after growth plate closure): Vessels anastomose → epiphysis and subchondral regions more susceptible
Adults
- Usually post-surgical, post-traumatic, or from contiguous spread
- Vertebral osteomyelitis common (haematogenous spread to vertebral body endplates)
Cierny-Mader Classification (Chronic Osteomyelitis)
| Stage | Description |
|---|---|
| I (Medullary) | Infection confined to the medullary cavity |
| II (Superficial) | Surface of bone involved (contiguous spread from soft tissue) |
| III (Localised) | Full-thickness cortical sequestrum; bone still structurally stable |
| IV (Diffuse) | Permeative; bone mechanically unstable |
Combined with host status:
- Class A: Healthy host
- Class B: Compromised host (local or systemic)
- Class C: Treatment worse than disease
Clinical Features
| Feature | Detail |
|---|---|
| Acute | Fever, rigors, malaise, headache, point tenderness over bone, warmth, swelling, erythema |
| Children | Sudden limp, refusal to bear weight, point tenderness |
| Chronic | Dull pain; sinus tracts; palpable sequestrum/involucrum; episodes of acute flare after years of dormancy |
| Vertebral | Severe back pain not relieved by rest; tenderness over spinous process; fever |
| Sympathetic joint effusion | Adjacent joint may swell even without septic arthritis |
Investigations
Bloods
| Test | Finding |
|---|---|
| WBC | ↑ in acute (may be normal in chronic) |
| CRP | ↑ (sensitive; best for monitoring treatment response) |
| ESR | ↑ (less specific; slower to normalise) |
| Blood cultures | Positive in ~40% of AHO; mandatory before antibiotics |
Imaging
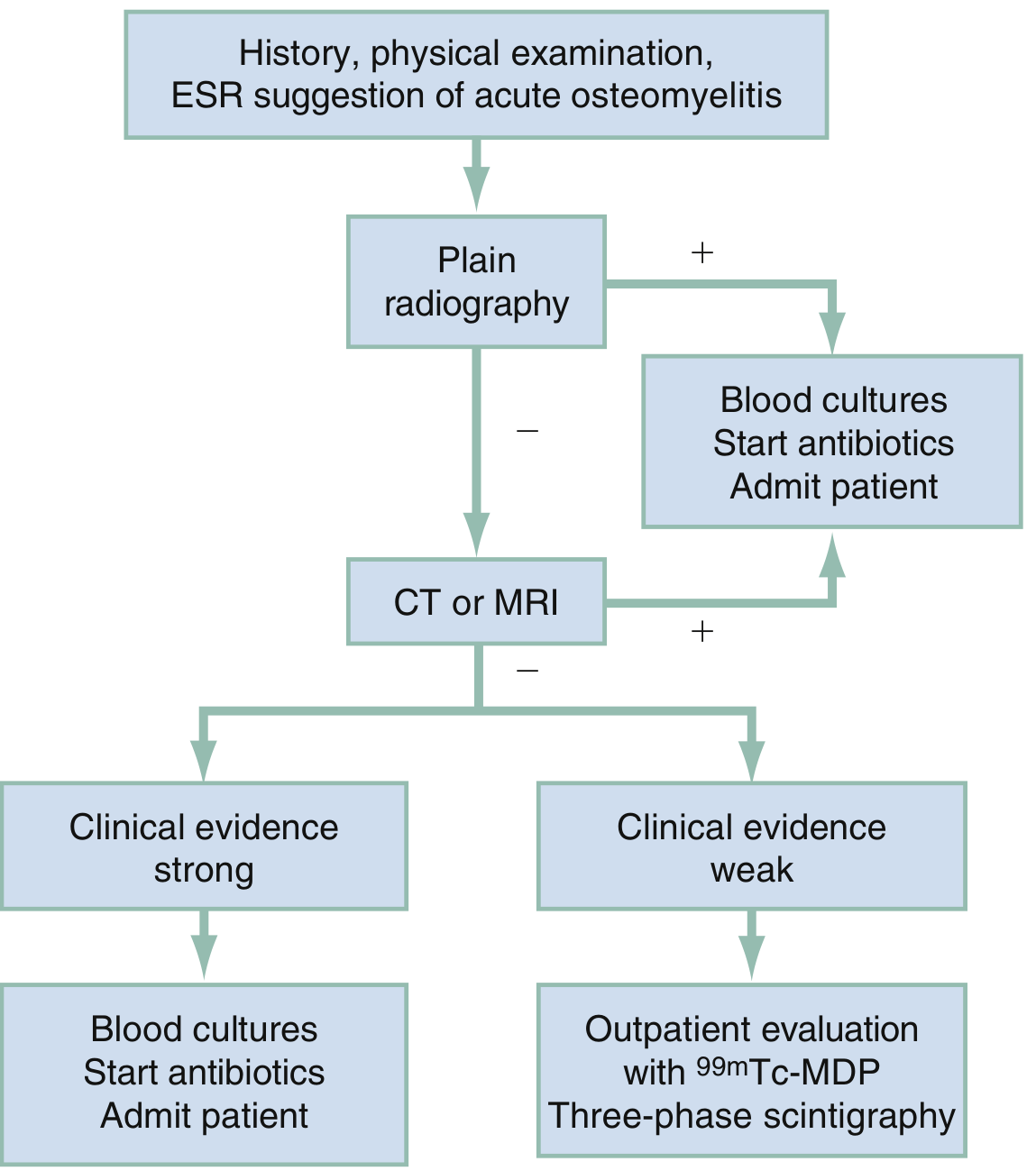
| Modality | Details |
|---|---|
| Plain X-ray | First-line; changes not visible until 10–21 days after onset (lytic focus, periosteal reaction, sclerosis); sequestrum/involucrum in chronic disease |
| MRI | Gold standard — sensitivity ~90%; earliest changes (bone marrow oedema on T2/STIR); identifies extent, soft tissue involvement, epidural abscess (vertebral osteomyelitis); with + without contrast |
| CT | Best for delineating cortical destruction, sequestrum, and guiding needle biopsy |
| Bone scintigraphy (⁹⁹mTc-MDP) | Sensitive but non-specific; useful when MRI unavailable or equivocal; three-phase scan |
| White cell scan / PET | Useful in implant-associated infections where MRI artefact is a problem |
Microbiological Diagnosis
- Bone biopsy / culture — gold standard for organism identification
- Culture positive in ~50% of cases (PCR assays improving this)
- Blood cultures before antibiotics
- Do NOT start antibiotics before cultures in stable patients
Specific Subtypes
Vertebral Osteomyelitis (Spondylodiscitis)
- Often haematogenous (urinary tract, skin, dental source)
- Lumbar > thoracic > cervical
- Disk avascular → bacteria proliferate → diskitis often coexists
- Complications: psoas abscess (lumbar), retropharyngeal abscess (cervical), epidural abscess (<15% but can cause paraplegia)
- MRI whole spine with contrast is the investigation of choice
- Treatment: IV antibiotics ± CT-guided biopsy; surgery for cord compression, abscess, instability, or failure of antibiotics
Diabetic Foot Osteomyelitis
- Contiguous spread from neuropathic/ischaemic ulcers
- Probe-to-bone test: if bone palpated through ulcer → osteomyelitis very likely (positive predictive value ~90%)
- Polymicrobial; MRI most sensitive; treatment often requires prolonged antibiotics ± surgical debridement
Posttraumatic / Implant-Associated
- Open fractures: Gustilo classification guides antibiotic cover
- Implant-associated: hardware left in place if stable and fracture not yet healed; remove if unstable or fracture healed
- Biofilm on implants makes eradication difficult without hardware removal
Treatment
Antibiotics
| Phase | Details |
|---|---|
| Empirical | Anti-staphylococcal cover: Flucloxacillin IV (MSSA) or Vancomycin (MRSA suspected); adjust after culture results |
| Duration | Acute: 4–6 weeks total (IV initially, then oral step-down when clinically improving); Chronic: longer, patient-specific |
| IV to oral switch | When: afebrile, CRP falling, tolerating orals, organism confirmed susceptible to oral agent |
| MRSA | Vancomycin, daptomycin, or linezolid |
Surgical Indications
| Indication | Action |
|---|---|
| Failed antibiotic therapy | Surgical debridement |
| Abscess (subperiosteal/soft tissue) | Incision and drainage |
| Sequestrum present | Sequestrectomy (dead bone must be removed) |
| Chronic osteomyelitis | Debridement, dead space management (local antibiotics — calcium sulphate beads, antibiotic-impregnated cement), bone grafting, flap reconstruction |
| Vertebral: cord compression, instability, abscess | Surgical decompression, drainage, stabilisation |
| Implant-associated (unstable) | Remove hardware; external fixation |
| Diabetic foot: extensive necrosis | Debridement ± amputation |
Dead Space Management
After debridement, the cavity must be filled:
- Local antibiotic beads (PMMA + gentamicin/vancomycin)
- Calcium sulphate beads
- Vascularised muscle flap
- Bone transport (Ilizarov) for large defects
Complications
| Complication | Notes |
|---|---|
| Chronic osteomyelitis | 5–25% of acute cases; episodes of flare after years of dormancy |
| Septic arthritis | Especially in infants; rapid articular cartilage destruction |
| Pathologic fracture | Through area of bone destruction |
| Growth disturbance | Epiphyseal involvement in children → shortened/deformed limb |
| Epidural abscess | Vertebral osteomyelitis → paralysis |
| Secondary amyloidosis | Chronic infection |
| Squamous cell carcinoma | Malignant transformation in chronic draining sinus tract (Marjolin's ulcer) |
| Sarcoma | Rare; in chronically infected bone |
| Bacteraemia/sepsis | Especially in acute haematogenous disease |
Mycobacterial (TB) Osteomyelitis — Special Mention
- Pott's disease: TB osteomyelitis of the spine (thoracolumbar most common)
- Bloodborne from pulmonary/extrapulmonary focus
- Presents with localised pain, low-grade fever, weight loss; cold abscess may track (paravertebral, psoas)
- More destructive and resistant than pyogenic; diagnosis often delayed (present for years)
- Treat with standard anti-TB regimen (6–9 months); surgery for cord compression or instability
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Rosen's Emergency Medicine; Schwartz's Principles of Surgery 11e
Diabetic foot
Finding Sources
Finding Sources
Reading File
Reading File
This is a shared conversation. Sign in to Orris to start your own chat.